J Neurosurg 117:795–799, 2012
Intermuscular lipoma of the gluteus muscles compressing the sciatic nerve: an inverted sciatic hernia Case report Eudaldo M. López-Tomassetti Fernández, M.D., Juan Ramón Hernández Hernández, M.D., Ph.D., Jose Ceballos Esparragon, M.D., Angel Turegano García, M.D., and Valentin Nuñez Jorge, M.D., Ph.D. Department of Gastrointestinal Surgery, Hospital Universitario Insular de Gran Canaria, Las Palmas, Las Palmas de Gran Canaria, Spain The authors report the case of a 50-year-old woman with a benign intermuscular lipoma of the gluteus compressing the sciatic nerve in its course through the sciatic notch. This benign soft-tissue tumor extended into the pelvis, displacing the rectum laterally. Resection was necessary to alleviate symptoms and prevent irreversible damage of the nerve. Wide exposure of the piriformis muscle and sciatic nerve via a transgluteal approach allowed safe lesion removal, and thus avoiding a laparotomy to resect the intrapelvic extension of the tumor. This report features a curious case of soft-tissue tumor growth across the sciatic foramen forming an inverted sciatic hernia. The authors’ proposed approach was simple and safe and avoided a laparotomy. (http://thejns.org/doi/abs/10.3171/2012.7.JNS111714)
Key Words • gluteal lipoma • peripheral nerve • sciatica • sciatic hernia
L
is the most common form of soft-tissue tumor. It is composed of adipose tissue, and treatment is not usually necessary unless the lesion becomes painful, is cosmetically unacceptable, restricts movement, or is malignant. Most of the time, lipomas are localized in the subcutaneous tissue and are asymptomatic, but they can also occur in deeper locations, compressing nerves. However, peripheral nerve compression by lipoma is infrequently reported in the medical literature. Herein, we report a case of deep-seated lipoma compressing the sciatic nerve and surgically removed to avoid sciatic nerve damage. ipoma
Case Report History and Examination. This 50-year-old woman J Neurosurg / Volume 117 / October 2012
with right-sided sciatic pain for the past year was referred to our hospital for further evaluation and treatment. She had an unremarkable medical history, and during the medical interview with the surgeon she reported gradually increasing constipation, pelvic pain, and rectal tenesmus without bleeding. Physical examination revealed sharp pain intensified by lifting the affected right leg straight. No gluteal mass was palpable, and compression of the sciatic nerve caused pain radiating down the posterior thigh, aggravated by dorsiflexion. She had no history of cancer, accidents involving the hips, or unexplained weight loss. Abdominal exploration was unremarkable with no gross evidence of neoplasia. Digital rectal examiThis article contains some figures that are displayed in color online but in black-and-white in the print edition.
795
E. M. López-Tomassetti Fernández et al. nation revealed good sphincter tone and a smooth mass in the right ischiorectal fossa. Hematological and biochemical workup, including complete blood count, renal function, liver function, and coagulation profile, all showed normal results, and electrophysiological studies of the right lower extremity were interpreted as normal. A CT scan was ordered for a strong suspicion of rectal cancer. Scanning revealed a large, well-defined solid mass measuring 15 × 5 × 4 cm (Fig. 1) and traversing the greater right sciatic foramen (Fig. 2). Magnetic resonance imaging was performed to depict the sciatic nerve in great anatomical detail over the sciatic notch. It showed a well-defined intermuscular lipoma that was compressing the sciatic nerve, traversing the greater sciatic foramen through the infrapiriformis area. It lay partly within the pelvis and partly within the gluteus muscle. Endoscopic ultrasound–fine needle aspiration did not provide conclusive cytological results. A final presumptive diagnosis of benign soft-tissue lipoma was made, and the patient underwent surgery after she was correctly informed.
Operation. Surgical intervention revealed a large, well-delimited lipoma. Tumor dissection was performed using a transgluteal approach, mainly because the lipoma had its origin in the gluteus muscles and the patient had radiographic features that made us believe this approach would be successful. The operation was accomplished by dissecting
Fig. 2. Upper: Computed tomography scan showing a well-delimited intermuscular lipoma (arrow). Lower: Coronal CT demonstrating herniation (arrows).
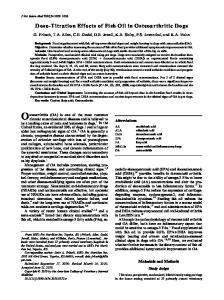
Fig. 1. A: Computed tomography scan showing a lipoma herniating through the sciatic foramen. Arrow indicates extrinsic compression of the rectum by the mass. B: Computed tomography scan demonstrating extrinsic compression of the rectum by the mass. Arrow indicates the lipoma herniating through the sciatic foramen. C: Computed tomography scan showing no extension of the mass lesion beyond the confines of the pelvis and intramuscular gluteus (dotted black line).
796
through the gluteus maximus muscle by splitting its fibers along a line that connects the major trochanter and middle portion of the sacrum, corresponding to the course of the piriformis muscle (Fig. 3). The muscle was well delimited without atrophy and was very easily identified. Blunt dissection and gentle separation allowed us to secure hemostasis ensuring a clean dry surgical field and complete removal of the capsule in an extracapsular plane—indispensable for ensuring complete resection of the lesion. Pelvic extension of the tumor was resected using blunt dissection to avoid intrapelvic trauma and bleeding. The surgical field was copiously irrigated with warm normal saline, and after ensuring that there was no bleeding, 2 closed-suction drains (deep and superficial) were placed in the operative field. J Neurosurg / Volume 117 / October 2012
Sciatic compression by huge lipoma
Fig. 3. A: Schematic indicating surgical access gained via a transgluteal approach. B: Schematic showing retraction of the right glu teus maximus muscle. Exposure was maintained using autostatic retractors. C: Schematic depicting surgical exposure of the lipoma. A Foerster clamp provides traction for removal of the mass. Blunt dissection was performed using the finger. With gently sweeping maneuvers, the lipoma was separated from the muscles. Printed with the permission of E. López-Tomassetti Fernández, 2012.
Postoperative Course. Drainage volume declined from 150 ml of serohematic fluid on the 1st postoperative day to 100 ml on the 2nd postoperative day. Both drains were removed on the 3rd postoperative day once total drainage volume was < 50 ml/24 hours. The patient’s postoperative course was uneventful, and sciatic pain improved immediately after surgery. Postoperative electrophysiological studies showed normal results, and she only had minor difficulty in walking, with mild discomfort in the right leg that improved through a rehabilitation program 4 months after surgery. The tumor was a single mass of adipose tissue measuring 15 × 4 × 4 cm. Histopathological examination revealed an encapsulated mass of mature adipose tissue traversed by small vessels with no atypia, hyperchromasia, or mitotic activity (Fig. 4). Six months after surgery a routine follow-up CT scan showed unilateral atrophy of the gluteus medius muscle and no sign of recurrence (Fig. 5).
Fig. 4. Photomicrograph of whole-tissue section of the lipoma showing proliferation of adipose tissue with some fibrous connective tissue. Adipocytes were irregular in size with large vacuolated cytoplasm. Nuclei were barely visible. H & E, original magnification × 10.
lipoma of the gluteus extended into the pelvis through the sciatic notch (as an inverted sciatic hernia) leading to sciatica. The most recent literature review6 revealed that only 99 cases of sciatic hernia have been reported since 1900 and that it is a rare cause of sciatic neuralgia. According to that review, the most commonly found hernia contents, clearly described in 97 operative reports, included ovary (28%), ureter11 (25%), small intestine (23%), and colon (18%). Involvement of the peripheral nerves by soft-tissue tumors (ganglions, hemangiomas, desmoids, ganglioneuromas, lymphangiomas, myoblastomas, and lipomas) is infrequent.2,5 The most common cause of peripheral nerve compression, based on the literature, is the ganglion cyst, and compression of the peripheral nerves by lipomas has been described as very rare. A recent review2
Discussion
Sciatic neuropathy due to benign, compressing softtissue tumors of the thigh is a very rare condition that can lead to irreversible damage and paralysis.1 This report shows a case of soft-tissue tumor growth across the sciatic foramen that shares clinical features similar to a sciatic hernia. Papen first documented sciatic hernia in 1750.7 It is described as a herniation of abdominal contents through the greater or lesser sciatic foramen, and patients most commonly present with an uncomfortable mass in the gluteal area. In the present case, a benign intermuscular J Neurosurg / Volume 117 / October 2012
Fig. 5. Computed tomography scans obtained in the patient before (A) and after (B and C) surgery. Although there was lipoma herniation (black line) before surgery (A), there was no sign of recurrence after surgery (B and C). Even though the patient was asymptomatic, there was gluteus medius atrophy.
797
E. M. López-Tomassetti Fernández et al. indicated that most publications are restricted to case reports or small series of patients. The frequency of publications about affected nerves is variable, but reportedly the radial nerve is most typically affected, followed by the median and ulnar nerves. Lipomas most often involve the upper extremity over lower limb nerves, and patients usually seek medical attention due to entrapment neuropathy. Ultrasound is very useful for superficial tumors; however, MRI provides more information in those situations in which the local anatomy is complex, as in our case. Surgical treatment results have demonstrated good outcomes in pain relief and neurological recovery in most reported cases. To our knowledge, two well-documented descriptions of a lipoma4,10 herniating through the sciatic foramen have been reported. As in spinal surgery, surgery for sciatic hernia is usually reserved for when the sciatic nerve is compressed or suspicious symptoms for malignant degeneration occur.1,3,4 Lipoma (ICD-O code 8850/0) is the most common soft-tissue mesenchymal neoplasm in adults, composed of mature fat cells without atypia. It usually presents as a painless soft-tissue mass, although larger ones can be painful when they compress peripheral nerves. Pathologists separate deep lipomas from lesions in an intramuscular or intermuscular location. Intramuscular and intermuscular lipomas do not show any specific gross features except that a portion of skeletal muscle is often attached to the periphery of the tumor. Intramuscular lipoma either can be well demarcated from surrounding skeletal muscle or shows an infiltrative growth pattern with mature adipocytes infiltrating and encasing skeletal muscle fibers that often show signs of atrophy. The infiltrating form of intramuscular lipoma has a higher local recurrence rate; therefore, total removal of the involved muscle or a compartmental resection has been suggested to minimize local recurrence. In our case, preoperative CT scanning and MRI helped us to define the lesion more precisely, indicating that it was an intermuscular (between muscle fascicles) lipoma of the gluteus that was compressing the sciatic nerve. The preoperative diagnosis of these deep lipomatous lesions is important to plan treatment8,9 and in our case allowed the surgeon to plan a surgical route both in advance and during surgery. Complete resection of the lipoma was achieved with digital dissection, and no muscle resection was necessary to get clear margins, as later verified by surgical pathology. Skipworth et al.10 documented a case of giant lipoma very similar to our case. In that particular case, MRI demonstrated a large fatty mass traversing the greater sciatic foramen, and it was necessary to perform a combined abdominoperineal approach to remove the tumor. Histopathological examination of the tumor revealed a lipoma-like, welldifferentiated liposarcoma. In our case the tumor had its origin in the gluteus, and the lipoma extended through the sciatic foramen as an “inverted” hernia; thus, a transgluteal approach was only necessary to remove the lipoma. Importantly, we did not need to plug the sciatic notch with autologous tissue or prosthetic mesh because the piriformis muscle was clearly identified and did not show any sign of atrophy. 798
To resect this tumor we always had in mind safe exposure of the sciatic and femoral cutaneous nerves. To expose the anatomical relationship of the piriformis muscle, the Adson self-retaining wound spreader was very useful, permitting visual control for digital dissection of the lipoma. Once identified, the lipoma was secured with a Foerster forceps, and digital dissection was performed. Sharp dissection was unnecessary because the lipoma did not show any infiltrative growth pattern at surgery and was well delimited. Our approach was similar to but not the same as surgical decompression of the sciatic nerve for a suspected piriformis syndrome. The procedure is a standard posterior approach to the hip, modified only by reducing the length of the incision necessary to expose the piriformis muscle. The incision is made in the direction of the gluteus maximus fibers, extending from the sciatic notch just below the posterior superior iliac spine medially, toward the greater trochanter laterally. Extension of the incision beyond the trochanter is not necessary for adequate exposure. The fascia overlying the gluteus maximus is incised in line with its fibers, and the muscle belly is then bluntly separated for exposure and resection of the tumor. Piriformis syndrome can be treated in a variety of ways, but commonly the tendinous insertion of the piriformis muscle at the greater trochanter is sharply released from its insertion. Then the piriformis muscle is dissected back to the sciatic notch for thorough inspection of the anatomical relationship between its muscle belly and the sciatic nerve. Once dissection and inspection are complete, 1.5–2 cm of the distal stump of the piriformis muscle is resected. If a bifid muscle belly is present, the separation between these must be completed so that there is no risk of retracted muscle further entrapping the nerve.
Conclusions
Herein we reported on an interesting case of lipoma herniation that produced sciatic nerve compression and rectal tenesmus due to lateral rectal displacement. Surgical intervention was necessary to remove the tumor. The transgluteal approach allowed proper visualization of the sciatic nerve, and removal of the lipoma was safely accomplished using blunt dissection without force. A disadvantage of this approach is the partly blind dissection of the pelvic extension of the lipoma. Nonetheless, we think this approach is simple and safe; thus, in similar cases a laparotomy may be avoided. Disclosure The authors report no conflict of interest concerning the materials or methods used in this study or the findings specified in this paper. Author contributions to the study and manuscript preparation include the following. Conception and design: López-Tomassetti Fernández, Turegano García. Drafting the article: López-Tomassetti Fernández. Critically revising the article: all authors. Reviewed submitted version of manuscript: all authors. Approved the final version of the manuscript on behalf of all authors: López-Tomassetti Fernández. Study supervision: López-Tomassetti Fernández, Hernández Hernández, Nuñez Jorge.
J Neurosurg / Volume 117 / October 2012
Sciatic compression by huge lipoma References 1. Botwin KP, Shah CP, Zak PJ: Sciatic neuropathy secondary to infiltrating intermuscular lipoma of the thigh. Am J Phys Med Rehabil 80:754–758, 2001 2. Flores LP, Carneiro JZ: Peripheral nerve compression secondary to adjacent lipomas. Surg Neurol 67:258–263, 2007 3. Hunt JA, Thompson JF: Giant infiltrating lipoma of the thigh causing sciatica. Aust N Z J Surg 67:225–226, 1997 4. Kerry RL, Tygart RL, Glas WW: Lipoma: a “reversed” perineal sciatic hernia. Am J Surg 107:883–884, 1964 5. Kim DH, Murovic JA, Tiel RL, Moes G, Kline DG: A series of 146 peripheral non-neural sheath nerve tumors: 30-year experience at Louisiana State University Health Sciences Center. J Neurosurg 102:256–266, 2005 6. Losanoff JE, Basson MD, Gruber SA, Weaver DW: Sciatic hernia: a comprehensive review of the world literature (19002008). Am J Surg 199:52–59, 2010 7. Martel L: Pointede hernie ischiatique: impotence fonctionelle du membre inferieur pendant 5 mois operation Guerison. Loire Med 19:165–174, 1900 8. Murphey MD, Carroll JF, Flemming DJ, Pope TL, Gannon FH, Kransdorf MJ: From the archives of the AFIP: benign
J Neurosurg / Volume 117 / October 2012
musculoskeletal lipomatous lesions. Radiographics 24:1433– 1466, 2004 9. Nishida J, Morita T, Ogose A, Okada K, Kakizaki H, Tajino T, et al: Imaging characteristics of deep-seated lipomatous tumors: intramuscular lipoma, intermuscular lipoma, and lipoma-like liposarcoma. J Orthop Sci 12:533–541, 2007 10. Skipworth RJ, Smith GH, Stewart KJ, Anderson DN: The tip of the iceberg: a giant pelvic atypical lipoma presenting as a sciatic hernia. World J Surg Oncol 4:33, 2006 11. Spring DB, Vandeman F, Watson RA: Computed tomographic demonstration of ureterosciatic hernia. AJR Am J Roentgenol 141:579–580, 1983 Manuscript submitted October 20, 2011. Accepted July 11, 2012. Please include this information when citing this paper: published online August 17, 2012; DOI: 10.3171/2012.7.JNS111714. Address correspondence to: Eudaldo López-Tomassetti Fer nández, M.D., Department of Surgery, Avenida Marítima del Sur, s/n, Las Palmas, Las Palmas de Gran Canaria 35016, Spain. email:
[email protected].
799