Throat Culture Is Necessary After Negative Rapid Antigen Detection Tests
Clinical Pediatrics Volume 46 Number 3 April 2007 241-246 © 2007 Sage Publications 10.1177/0009922806290219 http://clp.sagepub.com hosted at http://online.sagepub.com
Ayesha Mirza, MD,¹ Peter Wludyka, PhD,4 Thomas T. Chiu, MD, MBA,2 Mobeen H. Rathore, MD1,3 Summary: This study was conducted to determine if culture confirmation is needed for a negative rapid antigen detection test. Data on 18 509 tests done in patients younger than 18 years old were reviewed. Of the 14 167 (76.5%) that were negative, 968 (6.8%) were associated with positive cultures. No significant seasonal variation was noted. Significant differences were found between hospital and pediatric practices in the percentage of patients with a negative rapid antigen detection test who actually had group A β-hemolytic streptococcus (3.5% to 9.8%). This study supports the
recommendation of culture confirmation of a negative rapid antigen detection test and validation of results within an individual practice if confirmatory cultures are not being performed. This study showed a high false-negative rate of the negative rapid antigen detection test and variation among hospital and pediatric practices for rates of positive culture after a negative rapid antigen detection test.
Introduction
Because it is difficult to make a clinical diagnosis of GABHS, laboratory confirmation of GABHS infection using rapid antigen detection tests (RADTs) or culture is recommended for children with pharyngitis.1,3 Several RADTs for the detection of GABHS are commercially available and widely used in clinical practice. Compared with cultures, the sensitivity of the various commercially available RADTs varies considerably, from 70% to 90%.3 Some of the newer tests that use optical immunoassay and chemiluminescent DNA probes are more sensitive than older RADTs and may even be as sensitive as culture.3 Despite the popularity of RADTs, few studies have been done to compare the performance of various tests against each other and in different clinical settings. The controversy continues about the use of RADTs alone or confirmation of a negative RADT result with a throat culture.4,5 The American Academy of Pediatrics (AAP) recommends that clinical suspicion of GABHS pharyngitis be confirmed with a RADT, and if the result is negative, a throat culture be obtained to ensure that the patient does not have GABHS infection. Because
A
cute pharyngitis is one of the most common illnesses for which children seek medical care. Pediatricians in the United States make the diagnosis of acute pharyngitis, acute tonsillitis, or streptococcal sore throat more than 7 million times annually.1 Although viruses cause most of the infections, group A β-hemolytic Streptococcus (GABHS) accounts for 15% to 30% of cases of acute pharyngitis in children. Making an accurate diagnosis is essential to provide patients with appropriate antimicrobial therapy to shorten the duration of illness and, of more importance, to prevent the suppurative and nonsuppurative complications of GABHS.2 From the 1Pediatric Infectious Diseases and Immunology and 2 Department of Pediatrics, University of Florida Health Science Center; 3Wolfson Children’s Hospital, and the 4University of North Florida Center for Research and Consulting in Statistics, Jacksonville, Florida. Address correspondence to: Mobeen H. Rathore, MD, 653-1 West 8th Street, Jacksonville, FL 32209.
Keywords: group A β-hemolytic streptococcus, rapid antigen detection tests, throat culture.
241
Clinical Pediatrics / Vol. 46, No. 3, April 2007
of the high specificity of these RADTs (>95%), a positive RADT result is confirmatory and does not require follow-up cultures. The AAP further recommends that any physicians using RADTs without a follow-up culture may wish to compare their results with those of culture to validate adequate sensitivity in their practice.6 We conducted a study to determine the need of follow-up throat culture for the diagnosis of GABHS pharyngitis after a negative RADT result. The study was not designed to compare the performance of the 2 RADTs used or the RADT with culture methods. We hypothesized that the high positive predictive value of RADTs would forgo the need for confirmatory follow-up cultures for a negative RADT result. We also wanted to compare different private pediatric practices with each other and to the microbiology laboratory at Wolfson Children’s Hospital (WCH) to determine differences.
Methods The Institutional Review Board of University of Florida, Jacksonville, approved the study. Data on all RADTs done at 3 pediatric practices in Jacksonville, Florida (Practice A, B, and C) between March 1995 and November 2001 and at WCH between June 1999 and November 2001 were collected retrospectively. Data from WCH between March 1995 and May 1999 were not available. The 3 pediatric practices used the Qtest™ Kit (Becton Dickinson, Sparks, Md) and the WCH laboratory used Signify (Abbott Laboratories, Abbott Park, Ill). Nurses and medical assistants collected the specimens and performed the RADTs in the pediatric practices. At WCH, nurses obtained the specimens, and medical technologists performed the RADTs in the laboratory. The reported specificity and sensitivity is 96.3% and 94.2% for the RADT used by the 3 practices and 97.5% and 90.5% for the RADT used at WCH laboratory.7,8 Specimens were collected according to standard practice by using 2 swabs. Staff were trained to culture the surface of both tonsils and the posterior pharyngeal walls, taking care to avoid the mouth and other areas of the pharynx.9 One swab was used for the RADT. If the result was negative, the second swab was submitted for conventional culture. A RADT result was considered false negative if a culture was positive for GABHS in a patient with a negative RADT result.
α=.001 Limits:
0.10 Proportion TCX+
242
0.08
UDL P=.068
0.06
LDL
0.04 0.02 PractA
PractB
PractC
WCH
Practice Group Sizes: Min n=1598 Max n=5197
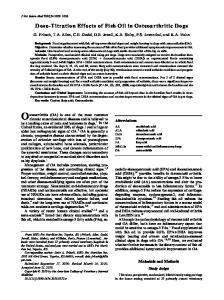
Figure 1. Analysis of means chart for comparing proportion of RADT-negative individuals who had GABHS for the 4 practices.
Cultures at the 3 pediatric practices were sent to reference laboratories according to the patient’s insurance. The 3 reference laboratories used standard sheep blood agar plate cultures incubated in 5% carbon dioxide. At WCH, Group A Selective Strep Agar with 5% sheep blood (ssA, Becton Dickinson) was used according to the manufacturer’s instructions.
Statistical Analysis Analyses were performed using the SAS system (SAS Institute, Cary, NC). Categoric response data were analyzed using categoric data methods, including the analysis of means (ANOM) for proportions, and when appropriate, Cochran-Mantel-Haenszel methods for seasonal variation. The ANOM is similar in power to the Pearson χ2 test but has the added feature of producing a decision chart.10 The ANOM allowed us to plot the proportion of RADTnegative individuals who actually had GABHS for each practice on a decision chart with upper and lower decision lines (Figure 1). If the proportion of RADT-negative individuals who actually had GABHS plotted outside the decision lines for any practice, then the equal proportion hypothesis was rejected (ie, equal proportion of RADT-negative individuals who actually had GABHS). The proportion of RADTnegative individuals who actually had GABHS were compared by practice using the ANOM with a significance level of P = .001. All pair wise differences were also tested with family wide level of significance of 0.01 using the Marascuillo procedure. Because the disease status of those that were RADT-positive was not known (throat cultures were
Throat Culture After Negative RADT / Mirza et al
Table 1.
RADT− RADT+
243
Aggregate Data Showing a Cross-Tabulation of the Total Number of Children in the Study With Regard to RADT and Culture Results GABHS (culture+)
GABHS (culture−)
Totals
968 A nG
13199 B (4342-A) nNG = 18509 − nG
14167 (RADT−) 4342 (RADT+) 18509 (total RADT)
GABHS = group A β-hemolytic streptococcus; nG (A) = total number of children with GABHS (culture+); nNG (B) = total number of children who were RADT+ without GABHS (culture−).
Table 2. Site Practice A Practice B Practice C Total offices WCH Overall total
Comparison of RADT Results at Individual Sites +
−
TCx
80 96 512 688 280 968
N
RADT
RADT
2731 2019 6894 11644 6865 18509
494 421 1697 2612 1730 4342
2237 1598 5197 9032 5135 14167
+
TCx
−
2157 1502 4685 8344 4855 13199
% RADT− TCx+ Individuals (95% CI) 3.5 6.0 9.8 7.6 5.5 6.8
(2.8-4.3) (4.8-7.2) (9.0-10.7) (7.1-8.2) (4.8-6.1) (6.4-7.2)
% NPV 96.4 93.9 90 92 95 93
Table shows the numbers of rapid antigen detection tests (RADTs), throat cultures (TCx) performed, percentage of RADT-negative individuals with disease (with 95% confidence intervals [CI]) and negative predictive value (NPV). WCH = Wolfson Children’s Hospital.
not performed), the sensitivity of the RADT could not be estimated with certainty. Reasonable minimum and maximum values for an estimate could be made, however. This idea will be illustrated using the aggregate data, where nG (A) is the total number of children in the study with GABHS and nNG (B) is the total number of children who were RADTpositive without GABHS (Table 1). The quantities A and B are unknown. Because sensitivity is the fraction of those with GABHS with RADT-positive result, it follows that sensitivity = A/(A + 968). Similarly, specificity = 13100/(13199 + 4342-A). Because of the high specificity of the RADTs used, for the purposes of this study, we assumed all positive RADT results were true positives.11 Maximum estimated sensitivity of the RADT was therefore calculated and determined to be at most 82%, implying that the minimum false-negative rate is 18%. This approach was applied to each of the practices to reproduce sensitivity estimates.
Results During the study period, 18509 RADTs were performed, and the results of 4342 (23.5%) were positive. The 14167 (76.5%) negative RADTs were all followed
by a throat culture for GABHS, and 968 (6.8%; 95% confidence interval [CI], 6.4%-7.2%) were associated with positive cultures. During the 7-year review period for the 3 pediatric practices, 11644 RADTs were performed, of which 2612 were positive and 9032 were negative. For the negative RADTs, a follow-up throat culture for GABHS was positive in 688 (7.6%; 95% CI, 7.1%-8.2%). During the 3-year review period at WCH, 6865 RADTs were done and 1730 (25%) were positive. For the 5135 negative RADTs, 280 follow-up throat cultures for GABHS were positive (5.5%; 95% CI, 4.8%-6.1%) (Tables 2 and 3). The percentage of RADT-negative patients who actually had GABHS was compared by practice, and pair wise differences were tested. All pair wise differences were significant except for Practice B versus WCH (Table 4). The 3 pediatric practices together, when compared with WCH, had an overall higher percentage of RADT-negative patients who had GABHS, 7.6% versus 5.5% (P < .001), with an odds ratio of 1.43 (95% CI, 1.24-1.65). There was, however, a considerable variation in the percentage of RADT-negative patients who had GABHS among the 3 practices, 9.8% for Practice C, 6.0% for Practice B, and 3.5% for Practice A (Table 2). The only practice with significant seasonal variation in the percentage of RADT-negative patients
244
Clinical Pediatrics / Vol. 46, No. 3, April 2007
Table 3. Prevalence of GABHS (%)
Site Practice A Practice B Practice C WCH
Comparison of Prevalence of GABHS at Individual Sites
574/2731 517/2019 2209/6894 2010/6865
(21) (26) (32) (29)
RADT+
RADT− Culture−
RADT− culture+
Minimum Sensitivity
Maximum Sensitivity
494 421 1697 1730
2237 1598 5197 5135
80 96 512 280
76% 73% 70% 81%
86% 81% 77% 86%
Table shows prevalence of group A β-hemolytic streptococcus (GABHS), cultures and rapid antigen detection tests (RADTs) performed and sensitivity of RADTs (minimum sensitivity associated with specificity = 90% and maximum sensitivity associated with specificity = 100%). WCH = Wolfson Children’s Hospital.
Table 4. Pair Wise Comparison Among Practice Centers for Percentage RADT− Individuals With GABHS Pairs Practice A-Practice B Practice A-Practice C Practice A-WCH Practice B-Practice C Practice B-WCH Practice C-WCH
Difference
Significant at α 0.01
−2.43 −6.28 −1.88 −3.84 0.55 4.4
Significant Significant Significant Significant Not significant Significant
RADT = rapid antigen detection test. WCH = Wolfson Children’s Hospital.
who had GABHS was Practice A (P = .0057). There was no seasonal variation when controlling for practice (Table 5).
Discussion Breese and Disney12 first described using a throat swab to identify GABHS on a sheep blood agar plate in 1954. Although it has been accepted as the gold standard for the diagnosis of GABHS pharyngitis for nearly 5 decades, there is no universally accepted procedure for performing a blood agar plate culture.3 Table 5. Sites Practice A Practice B Practice C WCH Total
Availability of the RADT has provided an alternate and faster way to diagnose patients with GABHS in busy pediatric practices. Although RADT kits may be more expensive, the ability to obtain quicker results enabling physicians to make treatment decisions during the office visit and potentially limiting the overuse of antibiotics make RADT more cost effective.13 Despite this, the relatively low sensitivity of RADTs remains the limiting factor when making universal recommendations for the use of these tests alone without follow-up throat cultures. The variation of a RADT across the clinical spectrum of patients tested for GABHS pharyngitis is substantial.12 Test sensitivity seems to be directly related to the overall clinical likelihood of GABHS pharyngitis (spectrum bias). Sensitivity is higher in patients who seem to have a greater likelihood of having GABHS pharyngitis on clinical grounds compared with those suspected of having a viral infection.14,15 It has been suggested that physicians use epidemiologic and clinical data to determine if a RADT should be ordered to increase the sensitivity of these tests.16-18 In a busy pediatric practice, however, this recommendation may be difficult to follow. In some instances, the patients may have been screened and an RADT performed even before evaluation by a physician.
Seasonal Distribution of Positive Throat Culture After Negative RADT
Winter Dec-Feb (%) 15 31 157 67 270
(2.7) (7.2) (10.1) (5.8) (7.3)
WCH = Wolfson Children’s Hospital.
Spring Mar-May (%) 19 26 143 49 237
(3.1) (6.4) (10.7) (4.9) (7.1)
Summer Jun-Aug (%) 12 11 87 78 188
(2.6) (3.4) (9.6) (6) (6.3)
Autumn Sep-Nov (%) 34 28 125 86 273
(5.7) (6.3) (8.9) (5.2) (6.6)
Throat Culture After Negative RADT / Mirza et al
The results obtained with RADTs for GABHS infections are influenced by the skill, experience, and expertise of the person collecting the specimen.3 False-negative RADT results may also be seen in those patients who have light growths of GABHS on cultures, which may be due to the poor swabbing technique used.11 To the best of our knowledge, our study has the largest number of patients who had a RADT performed in both private practice and a hospital setting to determine the sensitivity of RADTs. This allowed for comparison among the practices and to the WCH microbiology laboratory. The results of our study show that there is considerable variation among private pediatric practices, even when the same test is used. The variation in test results may reflect differences in the method of collection of the specimens (although all providers were given similar training) and also the experience of the person performing the test and the selection of patients by clinical criteria. Although we assumed for the purposes of this study that the 3 practices and the hospital microbiology laboratory performed all procedures with equal proficiency, the results of the study suggest otherwise. This study offers a real-world pediatric practice experience where no medical technologists were used in the office for performing RADTs and the swabs for throat cultures were sent to commercial referral laboratories determined by the patient’s insurance. The hospital results were better compared with the 3 practices together, with a negative predictive value of 94.5%. Practice A, however, showed superior results when compared with the hospital, with a negative predictive value of 96.4%. It is therefore possible from our assumption and published recommendations to forgo culture confirmation in some practices as recommended by the AAP (ie, if the RADT used in that particular practice could be confirmed to have a high sensitivity).6 However, this cannot be universally recommended even among the 4 sites in this study. Although we could not calculate absolute sensitivity given that positive RADTs were not confirmed by culture, the calculated maximum sensitivities of the RADT in our study were 77% to 86% (Table 3). Previously published studies indicate that most pediatricians would consider this level of sensitivity unacceptably low for their routine practice.5 Practice C, which had the highest proportion of RADT-negative patients who actually had GABHS
245
(9.8%), also had the greatest number of patients tested for GABHS pharyngitis than the other 2 practices. Whether performing more tests in a busy office could potentially have led to spectrum bias or else affected the quality of the test performed is a possibility. At the same time, this practice also had the highest prevalence of GABHS (Table 3). This was a retrospective analysis, therefore, we were unable to perform an in depth study of RADTnegative patients with GABHS and compare the growth on blood agar plates to the false-negative RADT. The study design also did not permit comparison of clinical scores with test results, which might have offered a possible explanation of the difference in results among the various practices and the hospital.14-18 No overall seasonal variation was noted when controlling for practice.
Conclusion Although the development of easy-to-use RADTs has changed clinical practice considerably, the sensitivity of these assays remains nonstandardized.3 Considerable variation still exists in clinical practice, so standard follow-up cultures should not be abandoned just yet. Any practice wishing to do so should follow the AAP guidelines and verify the results of the particular test they use against cultures in their own practice and develop a strong quality assurance program. Until such time, primary care providers should continue to obtain throat cultures when RADT results are negative.
Acknowledgment The authors would like to thank the physicians and staff at the 3 pediatric practices and the microbiology laboratory at Wolfson Children’s Hospital for their cooperation and help during the conduct of this study. Special thanks to Diane Halstead, PhD, Ken Horn, MD, and Sandra Morales, MD.
References 1. Gerber MA. Diagnosis and treatment of pharyngitis in children. Pediatr Clin N Am. 2005;52:729-747. 2. Randolph MF, Gerber MA, DeMeo KK, Wright L. The effect of antibiotic therapy on the clinical course of streptococcal pharyngitis. J Pediatr. 1985;106:870-875.
246
Clinical Pediatrics / Vol. 46, No. 3, April 2007
3. Gerber MA, Shulman ST. Rapid diagnosis of pharyngitis caused by group A streptococcci. Clin Micro Rev. 2004;17:571-580. 4. Mayes T, Pichichero ME. Are follow-up throat cultures necessary when rapid antigen detection tests are negative for group A streptococci. Clin Pediatr. 2001;40:191-195. 5. Armengol CE, Schlager TA, Hendley JO. Sensitivity of a rapid antigen detection test for group A streptococci in a private office setting: answering the Red Book’s request for validation. Pediatrics. 2004;113:924-926. 6. American Academy of Pediatrics. Group A Streptococcal Infections. 2003 Red Book. Report of the Committee on Infectious Diseases, 25th ed. Elk Grove Village, Ill: American Academy of Pediatrics; 2003:573-584. 7. Becton, Dickinson and Company. Qtest Strep, Package Insert. Sparks, Md; 2004. 8. Abbott Laboratories. Signify Strep A, Package Insert. Abbott Park, Ill; 2000. 9. Brien JH, Bass JW. Streptococcal pharyngitis: optimal site for throat culture. J Pediatr. 1985;106:781-783. 10. Nelson PR, Wludyka PS, Copeland KAF. The Analysis of Means: A Graphical Method for Comparing Means, Rates, and Proportions. ASA-SIAM Series on Statistics and Applied Probability. Philadelphia: SIAM; Alexandria, Va: ASA; 2005. 11. Edmonson BM, Farwell KR. Relationship between the clinical likelihood of group A streptococcal pharyngitis
12.
13.
14.
15.
16.
17.
18.
and the sensitivity of a rapid antigen detection test in a pediatric practice. Pediatrics. 2005;115:280-285. Breese BB, Disney FA. The accuracy of diagnosis of beta streptococcal infections on clinical grounds. J Pediatr. 1954;44:670-673. Webb KH. Does culture confirmation of high sensitivity rapid streptococcal test make sense? A medical decision analysis. Pediatrics. 1998;101:e2. Hall CH, Kieke B, Gonzales R, Belongia EA. Spectrum bias of a rapid antigen detection test for group A betahemolytic streptococcal pharyngitis in a pediatric population. Pediatrics. 2004;114:182-186. DiMatteo L, Lowenstein S, Brimhall B, Reiquam W, Gonzales R. The relationship between the clinical features of pharyngitis and the sensitivity of a rapid antigen test: evidence of spectrum bias. Ann Emerg Med. 2001; 38:648-652. Centor RM, Witherspoon JM, Dalton HP, Brody CE, Link K. The diagnosis of strep throat in adults in the emergency room. Med Decis Making. 1981;1:239-246. Wald ER, Green MD, Schwartz B, Barbadora K. A streptococcal score card revisited. Pediatr Emerg Care. 1998; 14:109-111. Attia MW, Zaotis T, Klein JD, Meier FA. Performance of a predictive model for streptococcal pharyngitis in children. Arch Pediatr Adolesc Med. 2001;155:687-691.