Border/East Hume Cancer Network
Patient Pathway Mapping Project Head and neck tumour stream: larynx, pharynx and oral cancer
July 2013
Head and Neck PPM Report
Page 1 of 106
TABLE OF CONTENTS 1.
EXECUTIVE SUMMARY ............................................................................................................................... 6
2.
AIM AND OBJECTIVES ..............................................................................................................................10
3.
PROJECT SCOPE ........................................................................................................................................11 3.1 Border/East Hume Cancer Network .......................................................................................................11 3.2 Patient Pathways Mapping Project ........................................................................................................12
4.
METHODOLOGY .......................................................................................................................................14
4.1 Operationalising the Patient Management Framework.............................................................................14 4.2 Participation of health professionals ..........................................................................................................16 4.3 Participation of consumers .........................................................................................................................16 4.3.1 Ethics approval ....................................................................................................................................16 4.4 Retrospective review of medical records ...................................................................................................16 4.5 Patient flow data analysis ...........................................................................................................................17 4.6 Assessment of scope of clinical practice ....................................................................................................17 4.7 Presentation of results ...............................................................................................................................18 5.
RESULTS ....................................................................................................................................................19
5.1 Data collected .............................................................................................................................................20 5.1.1 Participation of health professionals...................................................................................................20 5.1.2 Participation of consumers..................................................................................................................20 5.1.3 Retrospective review of medical records ............................................................................................20 5.2 Patient flow data analysis ...........................................................................................................................20 5.3 Supportive care...........................................................................................................................................22 5.4 Multidisciplinary care .................................................................................................................................23 5.4.1 Profile of Border/East Hume MDTMs..................................................................................................23 5.4.2 Number of patients presented at the MDTMs ....................................................................................23 5.4.3 Membership of the MDTM ..................................................................................................................24 5.5 Assessment of scope of clinical practice ....................................................................................................26 5.6 Generic successes and gaps in the care pathway across all tumour streams ............................................31 5.7 Specific successes and gaps in the care pathway for head and neck cancer .............................................40 6.
RECOMMENDATIONS ..............................................................................................................................45
6.1 Multidisciplinary Care .................................................................................................................................45 6.2 Care coordination .......................................................................................................................................46 6.3 Supportive care...........................................................................................................................................47 Head and Neck PPM Report
Page 2 of 106
6.4 Reducing Unwanted Variations in Care ......................................................................................................48 7.
DISCUSSION ..............................................................................................................................................49
8.
ACKNOWLEDGMENTS ..............................................................................................................................50
9.
REFERENCES .............................................................................................................................................51
10. APPENDICES .............................................................................................................................................52 Appendix 1: Patient Management Frameworks toolkit ...................................................................................52 Appendix 2: Supplementary Health Professional Interview Questions............................................................59 Appendix 3: Consumer Participant Questionnaire ...........................................................................................61 Appendix 4: Background to the Patient Pathways Mapping Project................................................................85 A4.1 Frameworks to guide cancer reform in Victoria ......................................................................................85 A4.1.1 Cancer Services Framework for Victoria ...........................................................................................85 A4.1.2 Victorian Cancer Action Plan 2008-2011...........................................................................................85 A4.2 The Victorian Integrated Cancer Services ................................................................................................87 A4.3 Establishment of tumour streams ............................................................................................................88 A4.4 Patient Management Frameworks...........................................................................................................88 A4.5 The four priority service improvement areas for statewide reform ........................................................90 A4.5.1 Multidisciplinary care ........................................................................................................................90 A4.5.2 Care coordination..............................................................................................................................92 A4.5.3 Supportive care .................................................................................................................................92 A4.5.4 Reducing variations in care ...............................................................................................................93 Appendix 5: Profile of the Hume Region ..........................................................................................................95 A5.1 Geographic coverage................................................................................................................................95 A5.1.1 Overview of the Hume cancer networks...........................................................................................95 A5.1.2 Sub regions within the Hume cancer networks ................................................................................97 A5.2 Population ...............................................................................................................................................97 A5.3 Cancer Profile .........................................................................................................................................100
Head and Neck PPM Report
Page 3 of 106
LIST OF TABLES Table 1: Tumour types identified as priority areas for the Border/East Hume Cancer Network.................... 13 Table 2: Tumour types identified as priority areas for the West Hume Cancer Network............................... 13 Table 3: Incidence of head and neck cancer in the five-year period 2004-2008 by LGA for Hume region, Albury and Southern NSW .............................................................................................................. 19 Table 4: Patient flow analysis for Head and Neck Cancer ............................................................................... 21 Table 5: MDTMs in the Border/East Hume Cancer Network .......................................................................... 23 Table 6: Number of patients presented at the Border/East Hume Cancer Network MDTMs ........................ 24 Table 7: Border/East Hume Cancer Network head and neck clinic membership ........................................... 25 Table 8: Border/East Hume Cancer Network scope of clinical practice checklist ........................................... 27 Table 9: Generic successes and gaps in the care pathway across all tumour streams ................................... 31 Table 10: Successes and gaps particular to Head and Neck malignancies ...................................................... 40 Table 11: Recommendations for multidisciplinary care .................................................................................. 45 Table 12: Recommendations for care coordination ........................................................................................ 46 Table 13: Recommendations for supportive care ........................................................................................... 47 Table 14: Recommendations for reducing unwanted variations in care ........................................................ 48 Table 15: Victorian and NSW LGAs included in this Patient Pathways Mapping Project ................................ 96 Table 16: Hume region, Albury and southern NSW population forecasts ..................................................... 98 Table 17: Hume, Albury and southern NSW population change 2011 - 2021 ................................................ 99
Head and Neck PPM Report
Page 4 of 106
LIST OF FIGURES Figure 1: Schematic representation of the optimal treatment pathway for the head and neck tumour stream ............................................................................................................................................. 15 Figure 2 : Supportive care referrals ................................................................................................................. 22 Figure 3: Systematic approach to quality in cancer services ........................................................................... 86 Figure 4: Map of the Victorian Integrated Cancer Services............................................................................. 87 Figure 5: The seven steps of the patient journey identified in the PMFs ....................................................... 89 Figure 6: Victoria’s model for multidisciplinary care....................................................................................... 91 Figure 7: Model for safety and quality in Victorian cancer services ............................................................... 94 Figure 8: Map of the Hume RICS West Hume and Border/East Hume Cancer Networks ............................... 95 Figure 9: Map of the Local Government Areas from Victoria and NSW that form part of the broader population catchment for cancer services in the Hume region....................................................... 96 Figure 10: Primary Care Partnership divisions in the Hume region ................................................................ 97 Figure 11: Total cancer incidence by LGA, Hume region, Albury and southern NSW for the 5-year period 2004-2008 ..................................................................................................................................... 100 Figure 12: Average annual cancer incidence by sex and age group, Hume region and Albury for the 5-year period 2004-2008 .......................................................................................................................... 101 Figure 13: Average annual cancer mortality by sex and age group, Hume region and Albury for the 5-year period 2004-2008 .......................................................................................................................... 102 Figure 14: Average annual cancer incidence by sex and cancer type in the Hume region for the 5-year period 2004-2008 .......................................................................................................................... 103 Figure 15: Average annual cancer incidence by sex and cancer type in Albury for the 5-year period 20042008 ............................................................................................................................................... 104 Figure 16: Average annual cancer mortality by sex and cancer type in the Hume region for the 5-year period 2004-2008 ..................................................................................................................................... 105 Figure 17: Average annual cancer mortality by sex and cancer type in Albury for the 5-year period 20042008 ............................................................................................................................................... 106
Head and Neck PPM Report
Page 5 of 106
1. EXECUTIVE SUMMARY The Victorian Department of Health (DH) has a significant cancer reform agenda that aims to improve planning and delivery of treatment and support to patients so that appropriate care is provided in a timely manner as close to the patients home as possible.1 Two leading policy documents guiding Victoria’s cancer reforms are the Cancer Services Framework and Victoria’s Cancer Action Plan (VCAP). The Cancer Services Framework identified structures and processes that support optimal cancer care, including the development of the Patient Management Frameworks (PMFs) in 2006 to guide the delivery of consistent cancer care for a range of tumour streams.2 The PMFs were developed to provide a consistent statewide approach to care management across the ten identified tumour streams and are intended to improve patient outcomes by focussing discussion on the critical steps of the patient journey in order to identify priority areas for improvement. They aim to reduce unwanted variation in care and describe optimal referral pathways for cancer care from diagnosis to endof-life care, inclusive of treatment and supportive care. This project aimed to identify the successes and gaps in the implementation of the PMFs across all stages of the patient journey for each of the four priority service improvement areas for statewide reform (multidisciplinary care, care coordination, supportive care, reducing unwanted variation in care). Further information about the background to the conduct of this project, including a detailed description of the Patient Management Frameworks and the process with which they were evaluated in this project is provided in Appendix 4 and 5. Project data were collected via a variety of mechanisms including consumer questionnaires and interviews, health professional interviews, and data analysis. The successes and gaps in service provision were identified from these data and are presented in Section 5 of this report. Based on these findings, recommendations for cancer service improvement were developed and prioritised, as presented below.
Multidisciplinary Care Number
Recommendation
1
Processes and procedures for the Head and Neck Clinic are refined, including to advocate for attendance by the full compliment of core disciplines and enhanced access to non core members, and further consideration of an appropriate venue for patient examination
2
Best practice models of multidisciplinary care continue to be promoted to local health professionals, specifically with respect to encouraging all specialists treating Head and Neck cancers in the Border/East Hume Cancer Network to refer to, and attend, the Head and Neck Clinic
1
Clinical Networks: A framework for Victoria 2008 Department of Human Services
2
Patient management frameworks 2006 Department of Human Services
Head and Neck PPM Report
Short-term
Long-term
Page 6 of 106
3
The resources and implications of accessing investigative equipment (including nasoendoscope) required for assessment of patients at the Head and Neck clinic are explored
4
Hume RICS continues to contribute to local and statewide initiatives to improve multidisciplinary team meeting administration, including to support the implementation of sustainable, standardised software and to contribute to statewide minimum datasets
5
Evaluate and enhance GP involvement in multidisciplinary teams, including participation in local MDTMs
Care coordination Number
Recommendation
1
Health professionals and consumers should be well informed about the range of different treatment and supportive care options, particularly those available close to the patient’s home
2
Hume RICS continues to promote engagement with the community health sector, and Home and Community Care (HACC) services, particularly in relation to linking rural and remote patients with their local support services where possible
3
Relevant federal and statewide strategies working towards improving communication channels between all health professionals, including GPs, should be promoted widely (such as the Human Services Directory (HSD) and e-referral
4
Communication systems are improved to ensure that patient medical information is available in a timely manner to all relevant clinicians, including the GP
5
Transition of care (discharge planning) processes should be improved to promote continuity of care, particularly between metropolitan and regional/rural health services, private hospitals and primary health services, and also between specialist cancer services, primary health and palliative care
6
The potential barriers in accessing appropriate services should be identified and strategies developed to address them
7
Protocols are developed and implemented to ensure that patients being transferred from a metropolitan treatment centre back to the Border/East Hume Cancer Network are referred to the relevant local support nurse/Cancer Care Coordinator in a timely manner
8
Processes are established to promote the development of cancer care management plans and palliative care pathways (as guided by the Goulburn Valley Health End of Life project)
9
Review of lymphoedema models of care, including early intervention, are supported
Head and Neck PPM Report
Short-term
Long-term
Page 7 of 106
10
Resources are developed for GPs that support appropriate and timely referral of people diagnosed with cancer to specialist cancer services and community services as appropriate
Supportive care Number
Recommendation
1
Health services are supported to ensure that all newly diagnosed cancer patients have access to supportive care screening (including the utilisation of a screening tool developed specifically for patients aged over 70 years) and that these results are documented in the patient’s central medical record
2
Supportive care screening is implemented at designated follow up intervals, including recurrence
3
The importance of supportive care discussion within a multidisciplinary team meeting is promoted and that this discussion is documented
4
Health services are supported to develop service models which include prevention, early intervention, treatment and support for cancer patients. Such services may include lymphoedema services, speech therapy, dietetics, counselling, PEG feeding and home oxygen
5
Hume RICS continues to provide and promote practical support and information for consumers (including the Hume RICS website, tailored standardised information packs and professional development sessions for specialist cancer staff) and continues to focus on improving information and access to travel, accommodation and financial supports
6
Options for access to pastoral care should be investigated and promoted
7
Partnerships with palliative care services are enhanced and a health promotion approach to palliative care is supported, including advocating for the importance of early intervention
8
Transport, financial, and emotional support continue to be raised as issues for rural communities in accessing oncology treatment
9
Continue to raise awareness of the specific supportive care needs of priority population groups including Aboriginal and Torres Strait Islander, adolescent and young adults, and culturally and linguistically diverse communities
10
A model is developed to facilitate increased access to psychosocial oncology support for public and private patients in community and inpatient settings across both sides of the NSW/Victorian border
Head and Neck PPM Report
Short-term
Long-term
Page 8 of 106
Reducing Unwanted Variations in Care Number
Recommendation
1
Consideration should be given to restricting surgery to 1 or 2 sites within the Border/East Hume Cancer Network due to the low volume of head and neck cancers
2
Medical oncology education for small rural health services and GPs should be facilitated, including pain and side effect management for cancer patients
3
Systems for timely access to allied health services and practical supports are developed, particularly for patients in private hospitals
4
In consultation with the Hume Medicare Local, Hume RICS provides GPs with access to oncology/specialist referral criteria and pathways, as informed by the findings of the West Hume Cancer Network GP project
5
Waiting times around access to theatres should be investigated to better understand the implications and impacts
6
Earlier referral processes from metropolitan settings to rural radiation services are investigated in order to avoid delays experienced by patients in accessing local radiotherapy services
7
Support the work undertaken by the Albury Wodonga Regional Cancer Centre Consortium to advocate for improved access to public medical oncology and radiotherapy
8
Further investigate the inequities in financial supports (including subsidies for dietary supplements, HACC services, community/district nursing) to identify the differences for public/private patients and NSW/Victorian residents
9
An education needs analysis should be conducted in order to develop and facilitate appropriate professional development for a broad range of health professionals involved in the care of patients with cancer; particularly as related to issues such as death and dying, treatmentrelated sexual issues, health literacy and self care
10
Support health services in exploring opportunities to implement and/or further extend their use of CHARM to improve systems relating to safety, quality and efficiency
Head and Neck PPM Report
Short-term
Long-term
Page 9 of 106
2. AIM AND OBJECTIVES The aim of the Patient Pathway Mapping Project was to identify opportunities for ‘whole system’ improvement and development, for consistent and coordinated cancer care across the Hume Region. The objectives of this project were to use the Patient Management Frameworks (PMFs) to guide planning for service improvement activities by:
Identifying the differences between the actual patient pathway and the optimal patient pathway as described by the Patient Management Frameworks, for each selected tumour stream Identifying strengths, gaps and duplications in the actual pathway of patients for each tumour stream Providing recommendations to support improvements focusing on delivering optimal treatment and support to patients, at each step of the care pathway
Head and Neck PPM Report
Page 10 of 106
3. PROJECT SCOPE 3.1 Border/East Hume Cancer Network The Border/East Hume Cancer Network is a cross-border collaboration of public and private health services and clinicians, as shown in Appendix 5. Patients who attend these services are drawn from a large regional population of close to 250,000 from the Victorian Local Government Areas (LGA) of Wodonga, Indigo, Towong, Wangaratta, Alpine, Mansfield and Benalla, and from the Murray region of southern NSW. The principal public hospitals providing cancer services in the Border/East Hume Cancer Network are:
Albury Wodonga Health (Albury and Wodonga campuses) – AWH Northeast Health Wangaratta – NHW
The principal private (Ramsay Health) hospitals providing cancer services are:
Albury Wodonga Private Hospital – AWPH Murray Valley Private Hospital – MVPH Wangaratta Private – WP
Albury Wodonga Health (AWH) and Northeast Health Wangaratta (NHW) are publically funded services and provide diagnostic, surgical, chemotherapy and allied health services (please note that for AWH chemotherapy is only available at the Albury campus). Depending on the procedure/treatment regime, privately insured or Department of Veteran’s Affairs (DVA) patients may elect to have surgery and/or chemotherapy at one of the private hospitals listed above. Other smaller rural hospitals across the Border/East Hume Cancer Network may provide inpatient or outpatient supportive care services to cancer patients. In the Border/East Hume Cancer Network, radiation oncology and medical oncology are supplied by private providers. Radiotherapy is provided by Radiation Oncology Victoria (ROV) at the Murray Valley Radiation Oncology Centre in Wodonga. ROV is a private provider of radiotherapy services across metropolitan Melbourne and country Victoria. Border Medical Oncology (BMO) is a private practice that provides medical oncology consultancy in Wodonga. A public medical oncology registrar and Oncology Nurse Practitioner are also employed by Albury Wodonga Health and they work in partnership with the medical oncologists at BMO. The Border/East Hume Cancer Network has also attracted the services of many generalist private medical practitioners, including surgeons, pathology and radiology agencies, an oncology pharmacist, psychologists and allied health providers (including physiotherapists, dietitians, lymphoedema therapists, continence nurses), who contribute substantially to cancer care. With respect to supportive services in the Border/East Hume Cancer Network, the Cancer Institute NSW provides funding for a 1.0FTE Cancer Care Coordinator, a 0.5FTE Multidisciplinary Team Meeting Administrator and a 0.6FTE Oncology Social Worker. Hume RICS also provides funding for a 0.5FTE Multidisciplinary Team Meeting Administrator in the Border/East Hume Cancer Network (to enable the cross-border position to be employed on a full-time basis) and a 0.8FTE Cancer Resource Nurse. There are Breast Care Nurses in Albury/Wodonga, Benalla and Alpine (funded by the McGrath Foundation) and in Head and Neck PPM Report
Page 11 of 106
Wangaratta (funded by Northeast Health Wangaratta). The Leukaemia Foundation funds a Support Coordinator for Albury/Wodonga and surrounds. A number of surgeons in private practice also employ nurses to provide support to their patients. Palliative care clinical teams are located at Albury Wodonga Health (Wodonga campus), Northeast Health Wangaratta and Mercy Health Albury. There is a community-based consultancy service provided by the NSW Murrumbidgee Local Health District and Ovens and King Community Health/Gateway Health in Victoria, including dedicated Clinical Nurse Consultant positions. There are also community based palliative care services provided by District Nurses/Home Nursing in rural areas such as Alpine, Corryong, Benalla, Tallangatta and Mansfield. Visiting palliative care physicians attend from NSW (from Sacred Heart Hospital in Sydney) and Victoria (from St Vincent’s Hospital Melbourne). Stakeholders in the Border/East Hume Cancer Network have crafted a collaborative model of regionally based health care to service all in the region who seek cancer care. This collaboration was led in the mid2000’s through the Border Cancer Collaboration who developed partnerships and processes to reduce the impediments faced by those accessing cancer services caused by state and other jurisdictional boundaries. There are also linkages to metropolitan services and clinicians in Melbourne and Sydney and rare/complex cases are referred to these services as required. Whilst the Border/East Hume Cancer Network hosts a number of local Multidisciplinary Team Meetings (described in further detail in Section 5.4), remote linkages to metropolitan meetings are also available.
3.2 Patient Pathways Mapping Project Patient pathways mapping in the Border/East and West Hume Cancer Networks were undertaken for the tumour streams as shown in Table 1 and Table 2. The Border/East and West Hume Clinical Reference Groups, as well as the respective Network committees (who act as advisory bodies to Hume RICS) were consulted to identify the top priority tumour types in each network. These tumour types were then allocated to their corresponding tumour streams, and mapped against the relevant PMFs (as presented in Table 1 and Table 2). It is important to note that the primary focus of this project was on the services provided within the Border/East Hume Cancer Network. Whilst consideration was given to the experiences of patients required to travel outside of the region for components of their care, this was not a main focus of the project and detailed investigation of the services provided outside of the region (including at metropolitan sites) was not conducted.
Head and Neck PPM Report
Page 12 of 106
Table 1: Tumour types identified as priority areas for the Border/East Hume Cancer Network Tumour type
Tumour stream
PMF
Ovarian
Gynaecological
Ovarian
Melanoma
Skin
Melanoma
Larynx, pharynx and oral
Head & Neck
Larynx, pharynx and oral
Prostate
Genitourinary
Prostate
Testicular
Genitourinary
Testicular
Pancreatic
Upper Gastrointestinal
Pancreatic
Colon & Rectal
Colorectal
Colon & Rectal
Intermediate grade Non-Hodgkin lymphoma
Haematological
Intermediate grade Non-Hodgkin lymphoma
Non-small cell lung
Lung
Non-small cell lung
Cerebral metastases
Central Nervous System
Cerebral metastases
Malignant glioma
Central Nervous System
Malignant glioma
Table 2: Tumour types identified as priority areas for the West Hume Cancer Network Tumour type
Tumour stream
PMF
Non-small cell lung
Lung
Non-small cell lung
Colon & Rectal
Colorectal
Colon & rectal
Breast
Breast
Breast
Prostate
Genitourinary
Prostate
Ovarian
Gynaecological
Ovarian
Melanoma
Skin
Melanoma
Larynx, pharynx and oral
Head & Neck
Larynx, pharynx and oral
Intermediate grade Non-Hodgkin lymphoma
Haematological
Intermediate grade Non-Hodgkin lymphoma
Head and Neck PPM Report
Page 13 of 106
4. METHODOLOGY This project compared the actual patient treatment pathway with the optimal pathway as described in the Patient Management Framework “Head and neck tumour stream: larynx, pharynx and oral cancer”. Project data were collected via a variety of mechanisms including consumer questionnaires and interviews, health professional interviews, and data analysis.
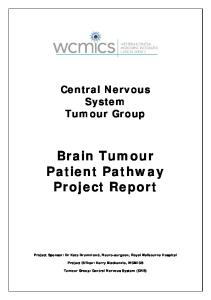
4.1 Operationalising the Patient Management Framework A schematic representation of the optimal treatment pathway for the head and neck tumour stream was developed by the Project Team, based on the information provided in the PMF and is presented in Figure 1. This was used alongside the project data collection tools in order to identify the key steps of the optimal treatment pathway, and consequently the gaps and successes of the actual patient pathway.
Head and Neck PPM Report
Page 14 of 106
Figure 1: Schematic representation of the optimal treatment pathway for the head and neck tumour stream 3 At greatest risk: Smokers Those with heavy alcohol consumption Betel nut/tobacco chewers (for oral cancers)
Patient Treatment Pathway – Larynx, Pharynx & Oral (Optimal) Based on larynx, pharynx & oral cancer PMF from Victorian DoH
Patient referred for Multidisciplinary Team Meeting discussion (MDTM)
Patient visits GP with symptoms which may include: Hoarse voice Difficulty swallowing Persistent sore throat (esp. with earache) Neck or parotid lump Mouth ulcer or mass Leukoplakia of oral mucosa Non-dental mouth or jaw pain Altered speech Spitting up blood
Treating specialist presents at MDTM; care plan formulated
Lead clinician informs patient of care plan
Referral options include: ENT/HN surgeon (larynx or pharynx) ENT/HN surgeon/Oral Maxillo-Facial surgeon (oral)
Patient decides on treatment Y/N? No Yes
Abnormality found
Diagnosis & Staging Biopsy of primary tumour or FNA of neck lump (if necessary under US guidance) Assessment of same by pathologist experienced in HN cancers Staging via clinical & endoscopic examination & appropriate imaging (CT and/or PET if available) *Synoptic reporting with path staging following surgical resection (see Treatment box)
No treatment Consider follow-up plan, may include palliation or end-oflife care
Treatment – may be one or a combination of: Surgery (see * in Diagnosis & Staging box) Radiotherapy Chemotherapy
Follow-up maintenance/review, can include rehabilitation of speech & swallowing, and follow-up of adequate oral intake All clear
Survival; consider monitoring plan
Abnormalities found
Investigative tests may include: Clinical examination, inc laryngoscopy and/or biopsy Imaging (CT, MRI, PET) as required
No Abnormality
Results
No treatment Consider follow-up plan
More treatment Results No more treatment
Consider follow-up plan, which may include palliation or end-of-life care
3
Patient management framework Head and neck tumour stream: Larynx, pharynx and oral cancer 2006 Department of Human Services
Head and Neck PPM Report
Page 15 of 106
4.2 Participation of health professionals Individual semi-structured interviews were conducted with clinicians and other health professionals to identify the successes and gaps in the implementation of the PMFs. The interview tool that was utilised for this project was based on the Department of Health resource “Patient Management Frameworks – toolkit” (attached as Appendix 1). It incorporated the key elements of multidisciplinary care, care coordination, supportive care and variations in care, at each stage of the cancer journey from diagnosis, through to end of life care. Supplementary health professional interview questions were also utilised (attached as Appendix 2).
4.3 Participation of consumers Consumer participation in the project was designed as an ‘opt in’ approach. Flyers were distributed to numerous health service sites including general practitioners, regional hospitals and community health centres. The recruitment strategy also included circulating invitations to regional cancer support groups and the Hume RICS Community Participation Network, as well as advertising through local newspapers and other media. Consumers were offered the opportunity to participate in an individual interview, complete a questionnaire or participate in a small group forum. The questionnaire and interview questions that were developed for this project (attached as Appendix 3) were informed by previously utilised patient surveys.4 5
4.3.1 Ethics approval Ethics applications were submitted to the Albury Wodonga Health Human Research Ethics Committee (HREC) and the Northeast Health Wangaratta HREC. The ethics submission to Albury Wodonga Health HREC included project research approval for Albury Wodonga Health (both Albury and Wodonga hospital campuses), Albury Wodonga Private Hospital, Murray Valley Private Hospital, Goulburn Valley Health and Kilmore District Hospital. The submission to Northeast Health Wangaratta HREC included project research approval for this site only. The purpose of the HREC submissions was to seek approval for Hume RICS to advertise for the recruitment of potential participants (cancer patients) in hospital settings within the Hume Region, and to conduct subsequent interviews, questionnaires and small group forums to collect information about their cancer care experiences.
4.4 Retrospective review of medical records Within the Victorian Admitted Episodes Dataset (VAED), ICD-10 diagnostic and procedural codes were used to identify a sample of patients with a new cancer diagnosis that had undergone treatment. Patients were selected from the datasets available for the 2009/10 and 2010/11 financial years. Up to 25 patients were randomly selected for each nominated tumour stream from each of the four Hume sub-regions. The actual number of patients reviewed was fewer for the low volume cancers according to the number of diagnoses within the specific period.
4 5
National Survey of NHS Patients Questionnaire (1999-2000), Centre for Social Research, Picker Institute Europe Victorian Cancer Patient Experience Survey Tool 2011, Victorian Department of Health
Head and Neck PPM Report
Page 16 of 106
A proforma was developed to record standardised information from the medical records, however as described in more detail below, there were major limitations in utilising information extracted from medical records. It should also be noted that the information retrieved from the medical records for the purposes of this project differed to that collected as part of the Victorian Cancer Service Performance Indicator reports. It was intended that information extracted from the medical record would be collected regarding presentation at MDTM, evidence of correspondence with General Practitioners, details of treatment and supportive care referrals. However, it was often difficult to generate a thorough and accurate representation of the patients entire care pathway based on the medical record review. This was due to patient care often being delivered across multiple sites in the Border/East Hume Cancer Network, which has a mix of public/private services, each with their own individual medical record. By examining the medical record at the site where the patient had the bulk of their treatment (eg. chemotherapy), it was often not possible to determine all of the relevant treatment and referrals initiated before they were admitted for chemotherapy (eg. from the site where they had their surgery) etc. Ideally patients would have been followed longitudinally through their care pathway across multiple health service sites, but this was not possible in the absence of a linked dataset that enabled patients to be easily tracked through the system. Therefore, a decision was made to exclude the majority of the information obtained from the medical record review due to concerns the data did not accurately represent the patient journey. However, information obtained from the medical record review regarding supportive care referrals was felt to be representative enough in order to be summarised for inclusion in this report, represented as Fitch’s tiered approach to providing supportive care.
4.5 Patient flow data analysis The VAED was again utilised to analyse patient flow of local residents to service providers both within and external to Hume RICS during the 2009/10 and 2010/11 financial years. The dataset was used to identify local residents of each of the four Hume sub-regions, then analysed to determine the service site at which these patients had an inpatient episode of care. A further analysis was completed to determine the type of care delivered by ICD-10 diagnostic and procedural codes for each of the nominated tumour streams. Unfortunately, as the Albury Wodonga Health- Albury Campus does not yet submit data in to the VAED, analysis of this activity was unable to be undertaken. Inpatient activity delivered at this service site is therefore not able to be determined and is not included in the analysis. It is anticipated that during 20132014 Albury campus will develop systems and procedures in order to be able to report their data to the VAED.
4.6 Assessment of scope of clinical practice The Patient Management Frameworks provide clear guidelines regarding the scope of clinical practice in order to provide quality and safe practice. As described in the PMFs, scope of practice reflects both the expertise and experience of the individual as well as the organisational capability for the provision of safe, Head and Neck PPM Report
Page 17 of 106
high quality cancer services. The guidelines presented in the PMF were used to develop a checklist that was completed for each of the health service sites within the Border/East Hume Cancer Network to determine their ability to provide the recommended level of service and expertise.
4.7 Presentation of results As described in Appendix 4, the focus of this Patient Pathways Mapping Project was to investigate the success with which the PMFs have been implemented at each step of the patient pathway, across each of the four key priority areas of:
multidisciplinary care care coordination supportive care reducing unwanted variation in practice (quality monitoring and support)
Accordingly, the successes and gaps in the care pathway for Head and Neck cancers in the Border/East Hume Cancer Network were described across these four priority areas. There were also a number of successes and gaps identified that were relevant across all tumour streams, and these have been presented separately to the tumour-specific successes and gaps. The results have been presented in a tabular format and directly reference the steps in the patient pathway listed in the PMF. Whilst there are seven steps of the patient pathway presented in the PMF, the focus of this project centred primarily around the six stages from initial diagnosis and referral through to end of life care. Recommendations across the four priority areas were developed and circulated to the Hume RICS Border/East Hume Clinical Reference Group for comment and classification as short-term or long-term activities.
Head and Neck PPM Report
Page 18 of 106
5. RESULTS This section presents the results of the Patient Pathways Mapping Project in the Border/East Hume Cancer Network. Table 3 presents data specifically related to the incidence of head and neck cancer in the five year period 2004-2008 for LGAs in the Victorian Hume region, as well as the NSW LGAs that are part of the broader population catchment for cancer services provided in the Hume region. Presented in this table are the data for Albury (which has been combined with Wodonga), as well as the combined incidence data for the LGAs of Corowa, Greater Hume, Berrigan, Deniliquin, Murray, Conargo, Jerilderie and Urana (collectively referred to in this report as Southern/Border NSW). Please note that Victorian LGA incidence data was sourced from the Cancer Council Victoria and NSW LGA incidence data was sourced from NSW Cancer Registry. Across Hume, Albury and Southern/Border NSW LGAs, there were a total of 326 cases of head and neck cancer for the five year period 2004-2008, which equates to approximately 65 cases per year. Table 3: Incidence of head and neck cancer in the five-year period 2004-2008 by LGA for Hume region, Albury and Southern/Border NSW 6 LGA Name
Cases
Albury/Wodonga
53
Southern/Border NSW*
41
Indigo
18
Wangaratta
29
Alpine
14
Towong
11
Mansfield
5
Benalla
9
Greater Shepparton
52
Mitchell
27
Moira
30
Murrindindi
22
Strathbogie
15
TOTAL for five-year period
326
* Combined figures for the LGAs of Corowa, Greater Hume, Berrigan, Deniliquin, Murray, Conargo, Jerilderie and Urana
6
Data obtained from Cancer Council Victoria and NSW Cancer Registry
Head and Neck PPM Report
Page 19 of 106
5.1 Data collected Data for this project were collected from a variety of sources, including health professional interviews, consumer questionnaires and interviews, medical record reviews, health service checklists and data analysis.
5.1.1 Participation of health professionals A total of 28 clinicians and health professionals were interviewed for the entire Patient Pathways Mapping Project (across all 9 tumour streams for the Border/East Hume Cancer Network), including medical oncologists, radiation oncologists, surgeons, physicians, general practitioners, registrars, oncology nurses, Nurse Unit Managers, Nurse Practitioners, Cancer Care Coordinators, research nurses, palliative care nurses, social workers, dietitians and other nurses who are involved in the care of cancer patients.
5.1.2 Participation of consumers For the entire Patient Pathways Mapping Project (across all 9 tumour streams for the Border/East Hume Cancer Network), a total of 43 consumers were interviewed (26 completed a written questionnaire, 5 participated in a small group forum and 12 consumers participated via a phone interview).
5.1.3 Retrospective review of medical records A total of 20 medical records were reviewed for patients who had received treatment specifically for head and neck cancers in Upper and Central Hume.
5.2 Patient flow data analysis Table 4 below illustrates the number of patients who contributed to hospital inpatient episodes of care for residents of the Hume region in the 2009-10 and 2010-2011 financial years. This specifically relates to residents of the Upper Hume sub region (Wodonga, Indigo and Towong LGAs) and Central Hume sub region (Wangaratta, Alpine, Mansfield and Benalla LGAs) but does NOT include residents of NSW. The diagram shows the number of patients who are residents of the Upper Hume and Lower Hume sub regions who received components of their care both within the Hume region (Central Hume, Upper Hume, Goulburn Valley and Lower Hume sub regions), and outside the Hume region (LMICS, NEMICS, SMICS, WCMICS, BSWRICS) and at other private hospitals across the state. As described previously, unfortunately, as the Albury Wodonga Health- Albury Campus does not submit data in to the VAED, analysis of this activity was unable to be undertaken. Inpatient activity delivered at this service site is therefore not able to be determined and is not included in the analysis. Additionally, due to privacy reasons, where there is less than 5 patients, the exact number can not be listed and instead must be represented as