Metastatic Tumor Volume and Extranodal Tumor Extension Clinical Significance in Patients With Stage II Breast Cancer Eva Drinka, MD; Pamela Allen, PhD, MPH; Andrew McBride, MD; Thomas Buchholz, MD; Aysegul Sahin, MD
� Context.—Lymph node status and the number of lymph node (LN) positive for cancer cells are the most important prognostic factors in breast cancer. Extranodal tumor extension (ENTE) has been used as a histopathologic feature to classify patients into high risk versus low risk for local recurrence. However, in the current era of early detection and systemic therapy, the prognostic significance of ENTE is not as well defined in patients with 1 to 3 LNs positive for cancer. Objective.—To determine whether the amount of tumor burden in an axillary dissection or the presence of ENTE provides any additional information regarding patient outcome in patents with 1 to 3 positive LN results. Design.—Clinical and pathologic factors were identified for 456 patients with breast cancer at the University of Texas MD Anderson Cancer Center, Houston, who had pT1 tumors and 1 to 3 LNs positive for cancer and were treated by mastectomy, with or without postmastectomy radiotherapy, between 1978 and 2007.
Results.—Of the 456 patients, 257 (56.4%), 141 (31.6%), and 58 (12.7%) patients had 1, 2, or 3 positive LN results, respectively. Extranodal tumor extension was present in 99 patients (21.7%) and was absent in the remaining 357 cases (78.3%). Seventy-six patients (16.7%) received radiation therapy. Patients had both worse overall survival time and disease-free survival when ENTE was present, regardless of the amount, as long as the treatment era was not included in the multivariate analysis (pre-2000 versus post-2000). However, ENTE was no longer significant on multivariate analysis when the year of treatment was taken into account. Conclusions.—The number of positive LNs remains an important predictor of survival in patients with 1 to 3 positive LN results, but the prognostic significance of ENTE in this cohort of patients has diminished over time. (Arch Pathol Lab Med. 2015;139:1288–1294; doi: 10.5858/arpa.2014-0375-OA)
L
positive for cancer cells.1–3 The National Cancer Institute’s database PDQ (Physician Data Query) on breast cancer prevention currently defines patients at highest risk for local recurrence as those with 4 or more positive LN results, grossly evident extranodal tumor extension (ENTE), primary tumors larger than 3 cm, and very close or positive deep margins in resection of the primary tumor.4–7 Radiation therapy has been shown to decrease locoregional recurrence rates in this high-risk group, even among patients who also receive adjuvant chemotherapy.8 However, the role of RT in patients with breast cancer and 1 to 3 positive LN results who are generally considered to be at low or intermediate risk for locoregional recurrence in the current era of breast cancer management is not well defined. Histopathologic factors, in addition to those already considered, in determining locoregional recurrence risk have been investigated in an effort to try to select patients with breast cancer and 1 to 3 positive LN findings who would benefit from RT. Several studies,9–15 including an internal study at the University of Texas MD Anderson Cancer Center (Houston), have suggested that postmastectomy RT should be considered in patients at low risk for locoregional recurrence if those patients have other adverse risk factors for recurrence, such as young age, tumor size greater than 2 cm, extracapsular extension, 3 positive LN
ymph node (LN) status and the number of LNs positive for cancer cells are the most important prognostic factors in patients with breast cancer. Postoperative chest wall and regional LN adjuvant radiation therapy (RT) traditionally has been given to patients with breast cancer considered to be at high risk for locoregional recurrence following mastectomy. Multiple experts and consensus groups, including the American Society of Radiation Oncology and the American Society of Clinical Oncology, recommend postmastectomy RT in addition to systemic therapy in high-risk patients who have 4 or more LNs
Accepted for publication January 26, 2015. Published as an Early Online Release March 13, 2015. From the Departments of Pathology (Drs Drinka and Sahin), Radiation Oncology (Drs Allen and Buchholz), and the Office of Executive Vice President and Physician-in-Chief (Dr Buchholz), University of Texas MD Anderson Cancer Center, Houston; and the Department of Radiation Oncology, University of Arizona School of Medicine, Phoenix (Dr McBride). The authors have no relevant financial interest in the products or companies described in this article. Reprints: Aysegul A. Sahin, MD, Department of Pathology, University of Texas MD Anderson Cancer Center, 1515 Holcombe Blvd, Unit 0085, Houston, TX 77030 (e-mail: asahin@mdanderson. org). 1288 Arch Pathol Lab Med—Vol 139, October 2015
Extranodal Tumor Extension—Drinka et al
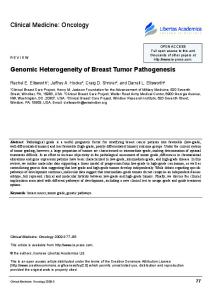
Figure 1. Two millimeters of carcinoma perforating through the lymph node capsule (hematoxylin-eosin, original magnification 320).
results, inadequate axillary dissection, close/positive surgical margins, skin/nipple invasion, or lymphovascular invasion. At MD Anderson Cancer Center, patients with breast cancer who have 3 positive LN findings, tumors greater than 2 cm, and/or gross ENTE have increasingly received RT after mastectomy during the past decade.3 The reported incidence of ENTE (defined as cancer perforating the LN capsule into the perinodal tissue) among patients with breast cancer patients and axillary LN metastases ranges from 20% to 60%.16–22 Some studies20,23–26 have found that the presence of ENTE increases the possibility of locoregional recurrence and systemic metastases and decreases disease-free survival (DFS) and overall survival (OS) rates. Because of these studies, it is postulated that in patients with ENTE, postmastectomy RT and more aggressive chemotherapy protocols should be offered to prevent locoregional recurrence.19 In this study, we retrospectively reviewed clinical and pathologic factors for patients at MD Anderson Cancer Center with pT1 to pT2 (,5 cm) tumors and 1 to 3 positive LN results, treated by mastectomy, with or without postmastectomy radiotherapy, between 1978 and 2007. Our purpose was to determine whether the number of positive axillary LN findings or the presence of ENTE predicted survival outcome in patients with breast cancer. We also sought to determine whether postmastectomy RT provided a survival benefit in patients with ENTE, hypothesizing that it did not provide significant benefit. MATERIALS AND METHODS The radiation oncology breast cancer database at MD Anderson Cancer Center was searched for patients fulfilling the pathologic criteria (pT1 to pT2 tumors and 1 to 3 positive LN results, treated by mastectomy, with or without postmastectomy radiotherapy), between the years 1978 and 2007, under an institutional review board–approved research protocol. The initial search revealed 1027 patients. Patients with bilateral synchronous primary pT1 to pT2 tumors or those with a primary tumor diagnosis of only ductal carcinoma in situ without invasion were then excluded. From the Arch Pathol Lab Med—Vol 139, October 2015
initial search, 456 patients (44.4%) had complete pathologic reports available for review. The medical records of those 456 patients diagnosed with breast cancer between 1978 and 2007 in our institution were then retrospectively analyzed, with clinical and pathologic reports available for all cases. Clinical and pathologic factors, including the histologic type of invasive cancer, the number of positive LN findings, the total number of LNs (sentinel or otherwise), and the presence or absence of ENTE, RT, and clinical outcomes, were identified for the 456 patients. Extranodal tumor extension was defined as cancer perforating the LN capsule into perinodal tissue (Figure 1). Tumor that was within, but which did not perforate, the LN capsule was considered negative for ENTE. We confirmed the diagnosis reported in the patients’ pathology reports by reviewing patients’ archived LN slides when available for review; 198 of the 456 patients (43.4%) included in this study had slides available for review. The original diagnosis was not changed in any of the 198 cases. We used the reported diagnoses for the remaining 258 patients (56.6%) for whom archived LN slides were not available. Data analysis was performed using Stata/MP 12.0 statistical software (StataCorp LP, College Station, Texas). Fisher exact test was used to assess measures of association in frequency tables. The survival function was performed with Kaplan-Meier estimates. The log-rank test was used to assess the equality of the survivor function across groups. The equality of medians for continuous variables was assessed with the nonparametric median test. A P value of .05 or less was considered statistically significant. Statistical tests were based on 2-sided significance levels. Survival time was calculated from the diagnosis date to the first occurrence of the considered event (either death or recurrence). Overall survival was defined as the time between diagnosis and death from any cause. Disease-free survival (DFS) was defined as the time between diagnosis date and the first recurrence of disease (locoregional or distant). The Cox proportional hazard model was used for multivariate analyses to assess the effect of patient, tumor, and other predictor factors of significance on the end points. The estimated hazard is reported. The Wald test was used to assess the role of covariates in the model (Stata Statistical Software).
RESULTS The mean age of patients was 50 years (range, 23–78 years). Of the 456 patients included in the study, 368 (80.7%) had invasive ductal carcinomas, 31 (6.8%) had invasive mixed carcinomas with ductal and lobular features, 43 (9.4%) had invasive lobular carcinomas, 5 (1.1%) had papillary carcinomas, 3 (0.7%) had micropapillary carcinomas, 2 (0.4%) had medullary carcinomas, 2 (0.4%) had tubular carcinomas, and 1 (0.2%) had a mucinous carcinoma; in 1 patient (0.2%) the type of primary tumor was unknown. The primary tumors were located in the left breast in 234 patients (51.3%) and in the right breast in 222 patients (48.6%). Of the 456 patients, 257 (56.4%), 141 (30.9%), and 58 (12.7%) had 1, 2, or 3 positive LN results, respectively. Extranodal tumor extension was present in 99 patients (21.7%) and was absent in the remaining 357 cases (78.3%). Seventy-six patients (16.7%) received RT. For the patients treated with radiation during the period of this study, a median dose of 50 Gy in 25 fractions was delivered to the chest wall with a prescribed dose of 50 Gy also delivered to the ipsilateral upper 3, intracostal, internal mammary LN region and the ipsilateral supraclavicular and axillary apex. The supraclavicular field was extended laterally to cover the anatomic location of Rotter (interpectoral) LNs and, therefore, the dissected level I/II axilla could receive from 20 to 50 Gy, depending on the depth and patient anatomy. For all patients, the OS rate at 5 and 10 years was 93% and 89%, while the DFS rate at 5 and 10 years were 85% and Extranodal Tumor Extension—Drinka et al 1289
Figure 2. Disease-free survival (DFS) rate for all patients (5- and 10-year DFS rates, 85% and 82%, respectively). Abbreviation: LN, lymph node. Figure 3. Disease-free survival (DFS) by radiation therapy (RT) status. Patients who received RT trended toward having worse DFS compared with patients who did not receive RT, but these groups did not have significantly different DFS (79.26% [no RT] versus 70.13% [RT]; P ¼ .08). Abbreviation: LN, lymph node. Figure 4. Disease-free survival (DFS) by number of total lymph nodes (LNs) positive for cancer cells. The number of positive axillary LNs was statistically significant for patient outcome. In patients with 3 positive LN findings, there was a decrease in DFS versus patients with 1 or 2 positive LN results (10-year DFS: 1 positive LN result, 86.05%; 2 positive LN results, 82.16%; 3 positive LN results, 63.30%; P ¼ .04). Figure 5. Disease-free survival (DFS) by presence or absence of extranodal tumor extension (ENTE). The DFS of patients with ENTE was significantly shorter than it was for those patients without ENTE (10-year DFS: 85.46% [no ENTE] versus 70.15% [ENTE]; P ¼ .001). Abbreviation: LN, lymph node.
82%, respectively (Figure 2). A total of 32 patients (7.0%) had a local recurrence (axillary, infraclavicular, supraclavicular, inframammary, manubrium, chest wall, or sternum). Ten of the 99 patients (10.1%) with ENTE had a local recurrence. Most patients with a local recurrence (28 of 32; 87.5%) did not receive RT, whereas 4 patients (12.5%) did receive radiation. Of those 4 patients, 2 (50.0%) had local recurrences that were outside the field of radiation, 1 (25.0%) had a chest wall recurrence, and 1 (25.0%) had an infraclavicular recurrence. We attempted looking into local recurrence among patients with 1, 2, or 3 positive LN results and RT, but the numbers were too small to provide a meaningful statistical evaluation and to draw any conclusions. Although patients who received RT trended toward having worse DFS than did patients who did not receive RT, 1290 Arch Pathol Lab Med—Vol 139, October 2015
these groups did not have significantly different DFS (79.26% [no RT] versus 70.13% [RT]; P ¼ .08) [Figure 3] or OS (86.23% [no RT] versus 79.05% [RT]; P ¼ .41). Kaplan-Meier DFS curves regarding the number of positive LNs and the presence or absence of ENTE are shown in Figures 4 and 5. The number of positive LN results was statistically significant for patient outcome. In patients with 3 positive LN findings, there was a decrease in OS and DFS versus patients with 1 or 2 positive LN results (10-year OS: 1 positive LN result, 90.11%; 2 positive LN results; 83.00%, 3 positive LN results, 69.96%; P , .001; and 10-year DFS: 1 positive LN result, 86.05%; 2 positive LN results, 82.16%; 3 positive LN results, 63.30%; P ¼ .04, respectively). Extranodal Tumor Extension—Drinka et al
Figure 6. Disease free survival (DFS) by number of positive lymph node (LN) found and radiation therapy (RT) status. The DFS durations of patients who received RT and had 1, 2, or 3 positive LN findings did not differ significantly from those of patients who did not receive RT (DFS all, P ¼.13; 1 positive LN result, no RT/RT, P ¼ .48; 2 positive LN results, no RT/RT, P ¼ .35; 3 positive LN results, no RT/RT; P ¼ .47). Figure 7. Overall survival (OS) by number of lymph nodes (LN) with cancer cells and the presence or absence of extranodal tumor extension (ENTE). Patients with 1 positive lymph node found and ENTE had a worse OS (10-year OS, 91.30 [1 positive LN/no ENTE] versus 82.69 [ENTE]; P ¼ .03). Patients with 2 or 3 positive LN results and ENTE did not show worse overall survival than those without ENTE (10-year OS: 86.45% [2 positive LNs/no ENTE] versus 73.75% [ENTE], P ¼ .09; 61.30% [3 positive LN results/no ENTE] versus 76.97% [ENTE], P ¼ .25). Figure 8. Disease-free survival (DFS) by number of lymph nodes (LNs) positive for cancer cells and the presence or absence of extranodal tumor extension (ENTE). Patients with a finding of 1 positive LN and ENTE trended toward a worse DFS (10-year DFS: 88.30% [1 positive LN found/no ENTE] versus 72.96% [ENTE]; P ¼.06) than their counterparts without ENTE. Although patients with 2 positive LNs found and ENTE did show worse DFS than those without ENTE, those with 3 positive LNs found did not (10-year DFS: 87.01% [2 positive LN results/no ENTE versus 69.62% [ENTE], P ¼ .01; 59.16% [3 positive LNs found/no ENTE] versus 67.17% [ENTE], P ¼ .87). Figure 9. Disease-free survival (DFS) by presence or absence of extranodal tumor extension (ENTE) and radiation therapy (RT) status. For patients with ENTE, receiving RT did not reach significance in terms of DFS (10-year DFS: 74.17% [ENTE no-RT] versus 52.06% [ENTE RT], P ¼ .13).
Of all the patients who received RT, most (35 of 76; 46.0%) had 2 positive LN findings. There were 26 patients (34.2%) with 1 positive LN finding who received RT, and 15 patients (19.7%) had 3 LNs positive for cancer cells who received RT. The 10-year DFS durations for patients who received RT and had 1, 2, or 3 positive LN findings did not differ significantly from those of patients who did not receive RT and had 1 (P ¼ .48), 2 (P ¼ .35), or 3 (P ¼ .47) LNs positive for cancer cells (Figure 6). The DFS (Figure 5) and OS of patients with ENTE were significantly shorter than those of patients without ENTE (10-year OS, 87.24% [no ENTE] versus 78.24% [ENTE]; P ¼ Arch Pathol Lab Med—Vol 139, October 2015
.004; and 10-year DFS, 85.46% [no ENTE] versus 70.15% [ENTE]; P ¼ .001, respectively). Of patients with ENTE (n ¼ 99), 36 (36.4%) had 1 positive LN finding, 39 (39.4%) had 2 positive LN results, and 24 patients (24.2%) had 3 LNs positive for cancer cells. Overall survival and DFS of patients by number of LNs positive for cancer and the presence or absence of ENTE are illustrated in Figures 7 and 8. Of all of the patients (n ¼ 99) with ENTE, 27 (27.3.5%) received RT and 72 (72.7%) did not. For patients with ENTE, receiving RT did not reach significance in DFS (74.17% [no RT] versus 52.06% [RT]; P ¼ .13) or OS (78.89% [no RT] versus 76.86% [RT]; P ¼ .59) (Figure 9). Extranodal Tumor Extension—Drinka et al 1291
Table 1.
Univariate Analysis
Results
Hazards Ratio
P Value
95% Confidence Interval
Overall survival Treatment after versus before 2000 3 versus 1 positive lymph node findings ENTE versus no ENTE Radiation therapy versus no radiation therapy
0.29 2.71 1.88 1.27
,.001 ,.001 .005 .41
0.17–0.50 1.59–4.64 1.21–2.90 0.72–2.26
Disease-free survival Treatment after versus before 2000 3 versus 1 positive lymph node findings ENTE versus no ENTE Radiation therapy versus no radiation therapy
0.30 2.01 2.01 1.59
,.001 .01 .002 .08
0.19–0.48 1.16–3.50 1.30–3.11 0.94–2.68
Abbreviation: ENTE, extranodal tumor extension.
The results of Cox proportional hazard analysis are illustrated in Tables 1 and 2. On univariate analysis, both the presence of ENTE and having 3 LNs positive for cancer cells (in comparison to 1 LN) were factors negatively related to both OS and DFS. Receiving RT was not a factor related to either DFS or OS on either univariate or multivariate analysis. On multivariate analysis, having 3 positive LN results (in comparison to 1 LN) showed a significant negative relationship to OS but not to DFS. The relationship to OS remained significant when taking into account the period during which the patient was treated. On multivariate analysis, ENTE was only related to DFS if the period during which the patient was treated was not taken into account. The clinical significance of ENTE might be different among patients who received more-contemporary breast cancer care, such as targeted systemic therapies. Furthermore, use of more-advanced RT techniques may affect the outcome of patients. CONCLUSION At our institution, information regarding LN status, including a microscopic measurement of the greatest cross-sectional area of a metastasis in the largest LN positive for cancer cells, the presence or absence of ENTE, as well as a microscopic measurement of the greatest crosssectional area of ENTE is included in every patient report with a positive LN finding. This information is used as one factor when trying to identify patients who may benefit from postmastectomy RT. Extranodal tumor extension has been used as a key histopathologic feature to classify patients with breast cancer as having a high or low risk for local recurrence.27,28 Table 2.
However, whether ENTE is indeed a prognostic factor for patients with breast cancer remains unclear. As far back as 1977, Mambo et al23 found that extranodal disease had an unfavorable effect on the prognosis of patients with breast cancer and fewer than 4 involved axillary nodes but no effect on the prognosis in patients with 4 or more involved axillary nodes. Subsequent studies revealed no such difference in the survival rates of those groups.17,21,29 In 2012, a study by Dobi et al30 reported that ENTE is an independent prognostic parameter in relation to DFS. The study also summarized the findings of 11 separate studies that assessed ENTE as a prognostic factor for local-regional recurrence, DFS, and OS.15,17,19,20,26,30–35 In 5 of the 11 studies (45.5%), there was a significant relationship between ENTE and OS. In 4 (36.4%) of the studies, including the 2 largest studies within the series (Dobi et al30 and Gruber et al31), a relationship between ENTE and DFS duration was present. In 2 (18.2%) of the studies (Hetelekidis et al17 and Pierce et al32), there was no significant correlation between ENTE and local regional recurrence, DFS, or OS. These studies’ inconsistent findings underscore the need to determine definitely the effect of ENTE on the survival of patients with breast cancer. The range of treatment strategies for patients with breast cancer and 1 to 3 LNs positive for cancer cells reflects the lack of a clear consensus regarding the role of ENTE in breast cancer prognosis. An informal survey conducted by the International Breast Cancer Study Group31 in 2002 showed that despite the uncertainty surrounding ENTE, numerous centers offer RT to patients who have 1 to 3 positive LN results in the presence of additional risk factors, such as ENTE. A later survey36 of members of the American Society for Therapeutic Radiology and Oncology and European Society for Radiation and Oncology revealed that
Multivariate Analysis
Results
Hazards Ratio
P Value
95% Confidence Interval
Overall survival Treatment before versus after 2000 3 versus 1 positive lymph node findings, not accounting for treatment period 3 versus 1 positive lymph node findings, accounting for treatment period ENTE versus no ENTE
0.39 2.31 2.38 1.56
.001 .004 .002 .06
0.22–0.70 1.32–4.06 1.39–4.09 0.99–2.46
Disease-free survival Treatment before versus after 2000 ENTE versus no ENTE, not accounting for treatment period ENTE versus no ENTE, accounting for treatment period Radiation therapy versus no radiation therapy
0.31 2.00 1.53 1.69
.001 .002 .07 .05
0.19–0.50 1.29–3.10 0.97–2.40 0.99–2.89
Abbreviation: ENTE, extranodal tumor extension. 1292 Arch Pathol Lab Med—Vol 139, October 2015
Extranodal Tumor Extension—Drinka et al
ENTE was the most influential factor in determining the recommendation for regional nodal RT in patients with breast cancer who had undergone lumpectomy or mastectomy. However, only 63.8% of the American and 53.3% of the European physicians surveyed claimed they would recommend radiation to the axilla in a patient who had undergone mastectomy and had 1 to 3 nodes positive for cancer cells in the presence of ENTE, illustrating the clear lack of consensus regarding treatment.36 At MD Anderson Cancer Center, RT was implemented in patients found to have 1 to 3 positive nodes on the basis of a study by Katz et al15 whose univariate and multivariate analysis showed that significant ENTE (defined as tumor .2 mm beyond the nodal capsule) was a predictor of increased risk of locoregional recurrence (27% risk of isolated and 33% greater risk of total locoregional recurrence). However in the study, focal (,2 mm beyond the nodal capsule) ENTE was also associated with a minimally increased risk of locoregional recurrence (18% risk of isolated and 22% risk of total locoregional recurrence). In addition, the study reported no relationships between ENTE and DFS or OS. In contrast, our current study illustrated both worse OS and DFS when ENTE was present regardless of the amount, as long as we did not differentiate between treatment eras. Extranodal tumor extension was no longer significant on multivariate analysis when the year of treatment was taken into account. The effect of treatment era can be postulated to be one contributing factor to the mixture of findings previously described in the literature. As treatment strategies change, the importance of different variables might also change, resulting in shifting data. Certainly, some of the different studies must encompass different periods and changes in treatment strategies. The present study included patients treated between 1978 and 2007, and the study by Katz et al15 included patients treated between 1975 and 1994, which may account for the difference in findings. Importantly, in our present study, only 27.3% (27 of 99) of the patients with ENTE received RT. If most patients with ENTE did not receive RT, other histologic or medical factors must have more strongly influenced clinical decision making. Although retrospective, the present study is one of the first, to our knowledge, to investigate the effect of RT on the duration of OS and DFS in patients with ENTE. In the proportion of patients with ENTE, receiving RT did not significantly improve OS or DFS. Furthermore, ENTE was no longer significant on multivariate analysis when the year of treatment was taken into account. In our present study, patients with 3 LNs positive for cancer cells had a worse OS than did patients with 1 positive LN on multivariate analysis, even with the period included in the assessment. In patients found to have 1 to 3 positive LNs, receiving RT did not significantly improve OS or DFS. Previous studies have looked into the effect of RT in patients with 1 to 3 positive LN findings. Recently, Cheng et al37 validated a locoregional recurrence risk-scoring system that included 4 factors: patient age, lymphovascular invasion, estrogen receptor negativity, and number of involved LNs. Based on those 4 factors, the researchers grouped patients into low-, intermediate- or high-risk groups. They found that postmastectomy RT was beneficial in patients with 1 to 3 positive LN results who have an intermediate risk for locoregional recurrence. In that group, 5-year locoregional control rate of patients who did not Arch Pathol Lab Med—Vol 139, October 2015
receive RT (90.0%) was significantly less than that of patients who received RT (96.3%; P ¼ .04). However, in patients with 1 to 3 positive LN findings and a low risk for locoregional recurrence, receiving RT did not result in better 5-year locoregional control rates (97.5% and 95.5%, respectively; P ¼ .22). Based on those results, patients with a high risk for axillary node involvement either in the form of more positive LNs or the presence of ENTE could be postulated to have a poorer outcome than would patients with 1 to 3 positive LN results or without ENTE. Importantly, we found that RT did not seem to extend these patients’ overall or DFS durations, which may be for several reasons. Presumably, patients with a worse overall clinical picture are the patients selected to receive RT, and they are presumed to be at risk for worse outcomes initially. Admittedly, we did not assess several risk factors that others have considered useful in identifying patients who may benefit RT, including younger age, larger tumor size, close/positive margins, skin/nipple invasion, and lymphovascular invasion. We also did not take some well-established prognostic factors (eg, estrogen and progesterone receptor status) into account in performing the multivariate analysis. One of these confounding factors may have had a greater negative effect than positive LNs number or ENTE on patient survival. As previously stated, we are now in a new era of breast cancer detection and treatments. Previous reports of much higher rates of local regional recurrence from subset analyses of randomized trials or large data sets for women found with 0 to 3 positive LNs were from patients who were diagnosed and treated several decades ago and, therefore, may not reflect advances in breast cancer management.4,5,9,10,13,14,38–40 Newer studies have shown that rates of locoregional recurrence after mastectomy without RT in patients with 1 to 3 positive LN findings are much less among patients treated within the past decade than they are among patients treated in earlier treatment eras.41 Perhaps the same reasoning can be applied to patients with ENTE. Certainly, clinicopathologic risk factors other than the presence of ENTE or number of positive LNs must be considered when deciding whether to offer adjuvant RT to patients with breast cancer. Nevertheless, the presence of ENTE has historically been noted in the literature as a strong indicator in the decision to offer RT, regardless of whether any retrospective or prospective studies support such a role. Although our study is lacking in scope, its findings suggest that ENTE and the number of positive LNs in the axilla should not be the sole factors considered when deciding whether to offer RT after mastectomy to patients with breast cancer, and the prognostic significance of ENTE in this cohort of patients has diminished over time. References 1. Harris JR, Halpin-Murphy P, McNeese M, Mendenhall NP, Morrow M, Robert NJ. Consensus statement on postmastectomy radiation therapy [review]. Int J Radiat Oncol Biol Phys. 1999;44(5):989–990. 2. Recht A, Edge SB, Solin LJ, et al; American Society of Clinical Oncology. Postmastectomy radiotherapy: clinical practice guidelines of the American Society of Clinical Oncology. J Clin Oncol. 2001;19(5):1539–1569. 3. McBride A, Allen P, Woodward W, et al. Locoregional recurrence risk for patients with T1,2 breast cancer with 1–3 positive lymph nodes treated with mastectomy and systemic treatment [published online ahead of print April 7, 2014]. Int J Radiat Oncol Biol Phys. 2014;89(2):392–398. 4. Ragaz J, Jackson SM, Le N, et al. Adjuvant radiotherapy and chemotherapy in node-positive premenopausal women with breast cancer. N Engl J Med. 1997; 337(14):956–962. 5. Overgaard M, Hansen PS, Overgaard J, et al. Postoperative radiotherapy in high-risk premenopausal women with breast cancer who receive adjuvant
Extranodal Tumor Extension—Drinka et al 1293
chemotherapy: Danish Breast Cancer Cooperative Group 82b trial. N Engl J Med. 1997;337(14):949–955. 6. Fowble B, Gray R, Gilchrist K, Goodman RL, Taylor S, Tormey DC. Identification of a subgroup of patients with breast cancer and histologically positive axillary nodes receiving adjuvant chemotherapy who may benefit from postoperative radiotherapy. J Clin Oncol. 1988;6(7):1107–1117. 7. National Cancer Institute. PubMed health: PDQ breast cancer treatment summaries. http://www.ncbi.nlm.nih.gov/pubmedhealth/PMH0032676/. Accessed September 20, 2014. 8. Early Breast Cancer Trialists’ Collaborative Group. Favourable and unfavourable effects on long-term survival of radiotherapy for early breast cancer: an overview of the randomised trials. Lancet. 2000;355(9217):1757– 1770. 9. Wallgren A, Bonetti M, Gelber RD, et al; International Breast Cancer Study Group Trials I through VII. Risk factors for locoregional recurrence among breast cancer patients: results from International Breast Cancer Study Group Trials I through VII. J Clin Oncol. 2003;21(7):1205–1213. 10. Recht A, Gray R, Davidson NE, et al. Locoregional failure 10 years after mastectomy and adjuvant chemotherapy with or without tamoxifen without irradiation: experience of the Eastern Cooperative Oncology Group. J Clin Oncol. 1999;17(6):1689–1700. 11. Katz A, Strom EA, Buchholz TA, Theriault R, Singletary SE, McNeese MD. The influence of pathologic tumor characteristics on locoregional recurrence rates following mastectomy. Int J Radiat Oncol Biol Phys. 2001;50(3):735–742. 12. Truong PT, Olivotto IA, Kader HA, Panades M, Speers CH, Berthelet E. Selecting breast cancer patients with T1–T2 tumors and one to three positive axillary nodes at high postmastectomy locoregional recurrence risk for adjuvant radiotherapy [oral presentation at the Canadian Association of Radiation Oncologists’ annual meeting; September 9–12, 2004, Halifax, NS, Canada]. Int J Radiat Oncol Biol Phys. 2005;61(5):1337–1347. 13. Taghian A, Jeong JH, Mamounas E, et al. Patterns of locoregional failure in patients with operable breast cancer treated by mastectomy and adjuvant chemotherapy with or without tamoxifen and without radiotherapy: results from five National Surgical Adjuvant Breast and Bowel Project randomized clinical trials [published online ahead of print September 27, 2004]. J Clin Oncol. 2004; 22(21):4247–4254. 14. Olivotto IA, Truong PT, Chua B. Postmastectomy radiation therapy: who needs it? [published online ahead of print September 27, 2004]. J Clin Oncol. 2004;22(21):4237–4239. 15. Katz A, Strom EA, Buchholz TA, et al. Locoregional recurrence patterns after mastectomy and doxorubicin-based chemotherapy: implications for postoperative irradiation. J Clin Oncol. 2000;18(15):2817–2827. 16. Palamba HW, Rombouts MC, Ruers TJ, Klinkenbijl JH, Wobbes T. Extranodal extension of axillary metastasis of invasive breast carcinoma as a possible predictor for the total number of positive lymph nodes. Eur J Surg Oncol. 2001;27(8):719–722. 17. Hetelekidis S, Schnitt SJ, Silver B, et al. The significance of extracapsular extension of axillary lymph node metastases in early-stage breast cancer. Int J Radiat Oncol Biol Phys. 2000;46(1):31–34. 18. Fisher ER, Gregorio RM, Redmond C, Kim WS, Fisher B. Pathologic findings from the National Surgical Adjuvant Breast Project (protocol no. 4), III: the significance of extranodal extension of axillary metastases. Am J Clin Pathol. 1976;65(4):439–444. 19. Leonard C, Corkill M, Tompkin J, et al. Are axillary recurrence and overall survival affected by axillary extranodal tumor extension in breast cancer?: implications for radiation therapy. J Clin Oncol. 1995;13(1):47–53. 20. Bucci JA, Kennedy CW, Burn J, Gillett DJ, Carmalt HL, Donnellan MJ, Joseph MG, Pendlebury SC. Implications of extranodal spread in node positive breast cancer: a review of survival and local recurrence. Breast. 2001;10(3):213– 219. 21. Ilknur GB, Hilmi A, Tulay C, et al; Dokuz Eylul ¨ ¨ University Medical Faculty Breast Tumors Study Group. The importance of extracapsular extension of axillary lymph node metastases in breast cancer. Tumori. 2004;90(1):107–111. 22. Turner RR, Chu KU, Qi K, Botnick LE, Hansen NM, Glass EC, Giuliano AE. Pathologic features associated with nonsentinel lymph node metastases in patients with metastatic breast carcinoma in a sentinel lymph node. Cancer. 2000;89(3):574–581. 23. Mambo NC, Gallager HS. Carcinoma of the breast: the prognostic significance of extranodal extension of axillary disease. Cancer. 1977;39(5): 2280–2285.
1294 Arch Pathol Lab Med—Vol 139, October 2015
24. Fisher BJ, Perera FE, Cooke AL, et al. Extracapsular axillary node extension in patients receiving adjuvant systemic therapy: an indication for radiotherapy? Int J Radiat Oncol Biol Phys. 1997;38(3):551–559. 25. Ragaz J, Jackson SM. Significance of axillary lymph node extranodal soft tissue extension and indications for postmastectomy irradiation. Cancer. 2000; 89(1):223–225. 26. Neri A, Marrelli D, Roviello F, et al. Prognostic value of extracapsular extension of axillary lymph node metastases in T1 to T3 breast cancer [published online ahead of print March 3, 2005]. Ann Surg Oncol. 2005;12(3):246–253. 27. Hartveit F, Skjaerven R, Maehle BO. Prognosis in breast cancer patients with tumour cells in the efferent vessels of their axillary nodes. J Pathol. 1983; 139(3):379–382. 28. Goldstein NS, Mani A, Vicini F, Ingold J. Prognostic features in patients with stage T1 breast carcinoma and a 0.5-cm or less lymph node metastasis. Significance of lymph node hilar tissue invasion. Am J Clin Pathol. 1999;111(1): 21–28. 29. Altinyollar H, Berbero˘glu U, Gulben K, Irkin F. The correlation of ¨ extranodal invasion with other prognostic parameters in lymph node positive breast cancer. J Surg Oncol. 2007;95(7):567–571. 30. Dobi E, Bazan F, Dufresne A, et al. Is extracapsular tumour spread a prognostic factor in patients with early breast cancer? [published online ahead of print July 5, 2012]. Int J Clin Oncol. 2013;18(4):607–613. 31. Gruber G, Bonetti M, Nasi ML, et al; International Breast Cancer Study Group. Prognostic value of extracapsular tumor spread for locoregional control in premenopausal patients with node-positive breast cancer treated with classical cyclophosphamide, methotrexate, and fluorouracil: long-term observations from International Breast Cancer Study Group trial VI. J Clin Oncol. 2005;23(28): 7089–7097. 32. Pierce LJ, Oberman HA, Strawderman MH, Lichter AS. Microscopic extracapsular extension in the axilla: is this an indication for axillary radiotherapy? Int J Radiat Oncol Biol Phys. 1995;33(2):253–259. 33. Brenner B, Siris N, Rakowsky E, Fenig E, Sulkes A, Lurie H. Prediction of outcome in locally advanced breast cancer by post-chemotherapy nodal status and baseline serum tumour markers. Br J Cancer. 2002;87(12):1404–1410. 34. Gruber G, Cole BF, Castiglione-Gertsch M, Holmberg SB, et al; International Breast Cancer Study Group. Extracapsular tumor spread and the risk of local, axillary and supraclavicular recurrence in node-positive, premenopausal patients with breast cancer [published online ahead of print April 2, 2008]. Ann Oncol. 2008;19(8):1393–1401. 35. Van den Eynden GG, Vandenberghe MK, van Dam PJ, et al. Increased sentinel lymph node lymphangiogenesis is associated with nonsentinel axillary lymph node involvement in breast cancer patients with a positive sentinel node. Clin Cancer Res. 2007;13(18, pt 1):5391–5397. 36. Ceilley E, Jagsi R, Goldberg S, et al. Radiotherapy for invasive breast cancer in North America and Europe: results of a survey. Int J Radiat Oncol Biol Phys. 2005;61(2):365–373. 37. Cheng SH, Tsai SY, Yu BL, et al. Validating a prognostic scoring system for postmastectomy locoregional recurrence in breast cancer [published online ahead of print November 1, 2012]. Int J Radiat Oncol Biol Phys. 2013;85(4):953– 958. 38. Overgaard M, Nielsen HM, Overgaard J. Is the benefit of postmastectomy irradiation limited to patients with four or more positive nodes, as recommended in international consensus reports?: a subgroup analysis of the DBCG 82 b&c randomized trials [published online ahead of print February 15, 2007]. Radiother Oncol. 2007;82(3):247–253. 39. Ragaz J, Olivotto IA, Spinelli JJ, et al. Locoregional radiation therapy in patients with high-risk breast cancer receiving adjuvant chemotherapy: 20-year results of the British Columbia randomized trial. J Natl Cancer Inst. 2005;97(2): 116–126. 40. Clarke M, Collins R, Darby S, et al; Early Breast Cancer Trialists’ Collaborative Group (EBCTCG). Effects of radiotherapy and of differences in the extent of surgery for early breast cancer on local recurrence and 15-year survival: an overview of the randomised trials [review]. Lancet. 2005;366(9503): 2087–2106. 41. Sharma R, Bedrosian I, Lucci A, et al. Present-day locoregional control in patients with t1 or t2 breast cancer with 0 and 1 to 3 positive lymph nodes after mastectomy without radiotherapy [published online ahead of print May 5, 2010]. Ann Surg Oncol. 2010;17(11):2899–2908.
Extranodal Tumor Extension—Drinka et al