Pacific University
CommonKnowledge School of Physician Assistant Studies
Theses, Dissertations and Capstone Projects
Summer 8-8-2015
Hydroxychloroquine in the Treatment of Osteoarthritis Briana Hougum
Follow this and additional works at: http://commons.pacificu.edu/pa Part of the Medicine and Health Sciences Commons Recommended Citation Hougum, Briana, "Hydroxychloroquine in the Treatment of Osteoarthritis" (2015). School of Physician Assistant Studies. Paper 540.
This Capstone Project is brought to you for free and open access by the Theses, Dissertations and Capstone Projects at CommonKnowledge. It has been accepted for inclusion in School of Physician Assistant Studies by an authorized administrator of CommonKnowledge. For more information, please contact
[email protected].
Hydroxychloroquine in the Treatment of Osteoarthritis Abstract
Background: Osteoarthritis (OA) accounts for one of the most common causes of loss of work and disability in America. Traditional treatments are aimed at symptomatic relief and maintaining functional capacity, but have not been shown to modify disease progression. Evidence for inflammatory and immune components in the development of OA lend support to expanding treatment options to potentially slow the disease and delay the need for invasive surgical intervention. Hydroxychloroquine (HCQ) is known for its use as an antimalarial and as a DMARD for rheumatoid arthritis, but has also been considered an option for treatment resistant OA. Several studies have looked at the medication’s potential for symptomatic relief, and have touched on the possibility of slowing disease progression in OA, but resources cite the drug as “uncertain benefit” in the realm of OA treatment. In patients with osteoarthritis, can hydroxychloroquine provide symptomatic improvement? Method: An exhaustive search using MEDLINE-Ovid, Web of Science, and CINAHL was performed using keywords: osteoarthritis and hydroxychloroquine. These were screened with eligibility criteria. The resulting studies were then appraised and assessed for quality with GRADE. Current NIH clinical trials were found to include two active studies relating to the use of HCQ in OA, with one for hand OA, and the other combining HCQ and a statin for knee OA. Results: Three studies were included in this systematic review, meeting the inclusion and exclusion criteria. One RCT looked at 44 patients with knee OA and showed overall improvement in pain, stiffness, and function with the treatment of HCQ. A retrospective observational study demonstrated that 6 of 8 patients with erosive hand OA, on the same dose of HCQ, responded to the treatment with global improvement, decreased synovitis, and decreased stiffness. Another RCT showed that patients with erosive hand OA had improvement in joint tenderness, and also saw decreased physiological markers of inflammation and immune destruction after treatment with HCQ. Conclusion: Hydroxychloroquine has been shown to provide symptomatic improvement in patients with OA, both in hand and knee OA, and is a reasonable treatment option for patients resistant to traditional first line analgesics. To a smaller extent, the drug effect has been assessed on a physiological basis with laboratory markers, and shown positive results in this respect. Further research into the disease modifying potential and larger clinical trials are needed in order to further validate this treatment and determine the OA subsets and patient populations that it would most benefit. Keywords: Hydroxychloroquine, osteoarthritis Degree Type
Capstone Project Degree Name
Master of Science in Physician Assistant Studies First Advisor
Annjanette Sommers, MS, PA-C
This capstone project is available at CommonKnowledge: http://commons.pacificu.edu/pa/540
Keywords
osteoarthritis, hydroxychloroquine Subject Categories
Medicine and Health Sciences Rights
Terms of use for work posted in CommonKnowledge.
This capstone project is available at CommonKnowledge: http://commons.pacificu.edu/pa/540
Copyright and terms of use If you have downloaded this document directly from the web or from CommonKnowledge, see the “Rights” section on the previous page for the terms of use. If you have received this document through an interlibrary loan/document delivery service, the following terms of use apply: Copyright in this work is held by the author(s). You may download or print any portion of this document for personal use only, or for any use that is allowed by fair use (Title 17, §107 U.S.C.). Except for personal or fair use, you or your borrowing library may not reproduce, remix, republish, post, transmit, or distribute this document, or any portion thereof, without the permission of the copyright owner. [Note: If this document is licensed under a Creative Commons license (see “Rights” on the previous page) which allows broader usage rights, your use is governed by the terms of that license.] Inquiries regarding further use of these materials should be addressed to: CommonKnowledge Rights, Pacific University Library, 2043 College Way, Forest Grove, OR 97116, (503) 352-7209. Email inquiries may be directed to:.
[email protected]
This capstone project is available at CommonKnowledge: http://commons.pacificu.edu/pa/540
NOTICE TO READERS This work is not a peer-reviewed publication. The Master’s Candidate author of this work has made every effort to provide accurate information and to rely on authoritative sources in the completion of this work. However, neither the author nor the faculty advisor(s) warrants the completeness, accuracy or usefulness of the information provided in this work. This work should not be considered authoritative or comprehensive in and of itself and the author and advisor(s) disclaim all responsibility for the results obtained from use of the information contained in this work. Knowledge and practice change constantly, and readers are advised to confirm the information found in this work with other more current and/or comprehensive sources. The student author attests that this work is completely his/her original authorship and that no material in this work has been plagiarized, fabricated or incorrectly attributed.
Hydroxychloroquine in the Treatment of Osteoarthritis
Briana Hougum
A Clinical Graduate Project Submitted to the Faculty of the School of Physician Assistant Studies Pacific University Hillsboro, OR For the Masters of Science Degree, August 8, 2015
Faculty Advisor: David Keene, PA-C Clinical Graduate Project Coordinator: Annjanette Sommers, PA PA-C, C, MS
1
|| Biography || Briana Hougum is from Northern California and received her Bachelor of Science degree from University of California, Los Angeles (UCLA), in 2012, with a major in Integrative Biology and Physiological Sciences. Her clinical background is working in physical therapy, and she hopes to use this experience to incorporate patient instruction and assistance with exercise into the area she ends up practicing in as a physician assistant. She is interested in pursuing a career in either internal medicine or orthopedic surgery.
2
|| Abstract || Background: Osteoarthritis (OA) accounts for one of the most common causes of loss of work and disability in America. Traditional treatments are aimed at symptomatic relief and maintaining functional capacity, but have not been shown to modify disease progression. Evidence for inflammatory and immune components in the development of OA lend support to expanding treatment options to potentially slow the disease and delay the need for invasive surgical intervention. Hydroxychloroquine (HCQ) is known for its use as an antimalarial and as a DMARD for rheumatoid arthritis, but has also been considered an option for treatment resistant OA. Several studies have looked at the medication’s potential for symptomatic relief, and have touched on the possibility of slowing disease progression in OA, but resources cite the drug as “uncertain benefit” in the realm of OA treatment. In patients with osteoarthritis, can hydroxychloroquine provide symptomatic improvement? Method: An exhaustive search using MEDLINE-Ovid, Web of Science, and CINAHL was performed using keywords: osteoarthritis and hydroxychloroquine. These were screened with eligibility criteria. The resulting studies were then appraised and assessed for quality with GRADE. Current NIH clinical trials were found to include two active studies relating to the use of HCQ in OA, with one for hand OA, and the other combining HCQ and a statin for knee OA. Results: Three studies were included in this systematic review, meeting the inclusion and exclusion criteria. One RCT looked at 44 patients with knee OA and showed overall improvement in pain, stiffness, and function with the treatment of HCQ. A retrospective observational study demonstrated that 6 of 8 patients with erosive hand OA, on the same dose of HCQ, responded to the treatment with global improvement, decreased synovitis, and decreased stiffness. Another RCT showed that patients with erosive hand OA had improvement in joint tenderness, and also saw decreased physiological markers of inflammation and immune destruction after treatment with HCQ. Conclusion: Hydroxychloroquine has been shown to provide symptomatic improvement in patients with OA, both in hand and knee OA, and is a reasonable treatment option for patients resistant to traditional first line analgesics. To a smaller extent, the drug effect has been assessed on a physiological basis with laboratory markers, and shown positive results in this respect. Further research into the disease modifying potential and larger clinical trials are needed in order to further validate this treatment and determine the OA subsets and patient populations that it would most benefit. Keywords: Hydroxychloroquine, osteoarthritis
3
|| Table of Contents || Biography.…..….…………….………………………………………………………………...….2 Abstract.….……..…………..…………………………………………………………..................3 Table of Contents …...……………..………………………………………………………….......4 List of Tables …...…….…………….…………………………………………………….............5 List of Abbreviations.……....…………….…………………………………………….................5 Background……………………………….………………………………………………….........6 Methods……………..………………………..……………………………………………...…….8 Results.….………………..……………………………..………………………………...…….…8 Discussion………………………..……....…………………………………………………..…..13 Conclusion…………………………………………………………………………………..…...15 References...……………...……………………………………………………………................16 Table 1……....…….……………………………………………………………………..…........19 Figure 1.……………………………………………………………………..……………….......19
4
List of Tables Table 1: Characteristics of Reviewed Studies and GRADE profile
List of Abbreviations DIP DMARD GRADE HCQ OA NIH NNT NSAIDs PIP RA RR sIL-2R SLE
distal interphalangeal disease modifying anti-rheumatic drug grading of recommendations, assessment, development, and evaluations hydroxychloroquine osteoarthritis National Institute of Health number needed to treat non-steroidal anti-inflammatories proximal interphalangeal rheumatoid arthritis risk reduction soluble interleukin-2 receptors systemic lupus erythematosus
5
Hydroxychloroquine in the Treatment of Osteoarthritis
BACKGROUND Osteoarthritis (OA) is a debilitating condition that accounts for one of the most common causes of disability among adults.1 This disease leads to lost productivity via chronic disability and affects nearly ¼ of adults over age 18, and 68% of adults over age 65.2 In addition to the impact on occupational work, OA stops many patients from doing their favorite athletic activities, from sports to simply walking, and even non-athletic everyday activities if it affects hands and fingers. Symptomatic control to reduce joint pain and preserve function early on is an important role of healthcare providers. The theories behind the etiology of OA have changed over the years, which is part of the reason new treatment options should be more extensively explored. Classically OA was thought to be “non-inflammatory” arthritis, with rheumatoid being the “inflammatory” form, however, there is much evidence to support that OA is not simply mechanical wear and tear. The pathophysiology showing inflammatory and immune processes behind the chondrocyte apoptosis3 leading to the cartilage destruction, “bone-on-bone” narrowed joint space, bone edema, and osteophytes seen in OA, lends support to using medications that provide disease modification in addition to analgesia. Acetaminophen (APAP) and NSAIDs are the most wellstudied, and first-line interventions in treating OA, but there is very little evidence for slowing of disease progression.4 Some NSAIDs, such as diclofenac, have actually been proven to have detrimental effects on the disease.5 In addition, many patients fail conservative treatment with APAP and NSAIDs, leaving providers with nonsurgical options including pain management on opioids or injections with either corticosteroids or viscosupplements. Depending on the patient,
6
these may or may not buy them time until the only option is surgery, which usually involves partial or total joint replacement. When considering the pathophysiology behind OA, there are less studied interventions that may provide further symptomatic relief, as well as have potential for modifying the disease process. Among these is hydroxychloroquine (HCQ), a medication well-studied as a DMARD for rheumatoid disease and considered to be one of the least toxic of the anti-rheumatics. HCQ not only has anti-inflammatory properties, which are thought to be via inhibition of prostaglandin production through interference with lysosomal actions; it also has immunomodulatory function. This function is thought to be through suppressing interleukin-1’s harmful effect on chondrocyte degradation. Nitric oxide is thought to be another culprit in accelerating cartilage degradation, and HCQ has been shown to act on chondrocytes to suppress this destructive process. 6 The subset of erosive type OA has more evidence to support an immune influence, however, there has been increasingly more evidence to show that the disease process of classic OA in large joints is also affected by immune-related chondrocyte destruction. Hydroxychloroquine itself was originally approved as an antimalarial drug, and is currently also used for RA and SLE. Since it is an oral medication that comes in generic form, it is cost effective and more easily available than many other immune-modulating drugs and some of the more costly NSAIDs such as celecoxib. Side effect profile is also smaller than many other anti-rheumatic drugs, with the main concern being potential for chloroquine toxicity in the eye. To monitor for this rare side effect, a baseline retina exam is recommended, with a repeat in 5 years for patients on long-term use of the medication.7 Using HCQ in the treatment of OA is currently offlabel, however, there are several completed studies and trials in progress to look at
7
the utility of this medication in treating both the symptoms and disease progression of OA. Can hydroxychloroquine provide symptomatic improvement in patients with osteoarthritis? METHODS An exhaustive literature search using MEDLINE-Ovid, Web Science, and CINAHL was conducted. The following search terms were used: “hydroxychloroquine” and “osteoarthritis.” The bibliographies from several relevant background articles were used and inclusion/exclusion criteria were applied. Included were studies conducted on patients with osteoarthritis, evaluating hydroxychloroquine in comparison to placebo or standard analgesics (including NSAIDs, APAP), and measuring symptomatic improvement. Other inclusion criteria required human studies and studies published in the English language. Studies were excluded if researchers didn’t supply data regarding patient response to therapy. Additionally, conferences or poster reports that did not report study details were excluded. In a search via NIH for current clinical trials using HCQ for OA, results included one recently completed for hand osteoarthritis,8 and a trial that is currently recruiting for combo hydroxychloroquine/atorvastatin treatment for knee OA.9 RESULTS The initial search yielded 62 articles for review. After eliminating duplicates and screening these results for relevant articles using eligibility criteria, there were a total of 3 articles. These articles were two randomized controlled trials10,11 and one retrospective observational study.12 (See Table 1) Another retrospective observational study was considered, but fell under exclusion criteria, since they did not define how they were measuring symptomatic improvement of OA in the patients.13 Jokar et al
8
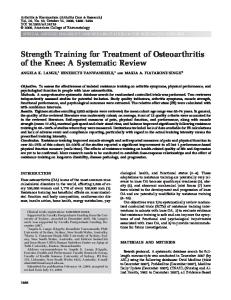
This was the most recent study10 of the three, performed in 2013, and was a randomized, double-blinded, placebo controlled trial. The authors wanted to look at the effect of hydroxychloroquine on symptoms of knee osteoarthritis, along with interest in the drug slowing progression of OA via its immunomodulatory properties and anti-inflammatory nature. The primary outcome evaluated was symptomatic improvement of OA. This was done via the WOMAC index, which looked at pain, stiffness, and functional limitation with scoring systems for each category.10 The study enrolled individuals from outpatient clinics who fit criteria designated by American College of Rheumatology for knee OA. Exclusion criteria were presence of secondary OA or other known inflammatory diseases, knee arthroscopy or corticosteroid injection within the past 6 months, hypersensitivity to antimalarials, or eye disease. After meeting criteria, 51 patients were randomized to either HCQ 200mg or placebo twice daily, and all participants were blinded to assignment. Patients were able to use NSAIDS and painkillers that they had already been taking, but were asked to keep record and to refrain from taking anything other than the study treatment 48 hours before their evaluations.10 WOMAC scores were recorded at the beginning of the study and at time points over a period of 6 months. Loss to follow-up and discontinuation of treatment reduced the study by 7 patients, leaving a total of 44 patients who were analyzed in the group to which they had been initially allocated. Results showed improvement for the treatment group in all three prongs of the WOMAC score system, and in using the total WOMAC score of the groups from baseline to day 180, there was a significant difference between the improvement seen in the treatment group compared to the placebo group. The average score went from 124.71 down to 81.14 at day 180 for the group receiving HCQ, while the placebo group score went from a baseline of 119.70
9
down to 116.48 in the same time period. The authors also noted that the record of pain medications used by patients concurrently during the trial showed a smaller number used in the HCQ treatment group, at 0.74 pills/day, compared to the placebo group, who reported using 0.96 pills/day.10 When interpreting this data, there was not a cutpoint made for the WOMAC score that designated individual patients as a “responder” to treatment. Because there is no binary “response to the therapy” that would allow an event rate to be calculated with the RR and NNT,14 the Cohen d index15 may be used to look at the difference in effect size, showing the magnitude of effect the treatment had on patients in comparison to the placebo. In looking at the changes in WOMAC score from pre to post treatment, the effect magnitude of the HCQ was “large”, as seen in Table 1. The authors did not calculate this effect magnitude, but did show the WOMAC scores plotted on a graph (Figure 1) demonstrating the treatment group’s significant change in mean score over time, and the placebo group’s minimal change from baseline to day 180. In both of these representations of data, the results show that there is evidence for symptomatic improvement in patients with OA treated with HCQ. The authors do recognize the need for larger clinical trials, and that they cannot make any claims about the disease-modifying potential of HCQ, since this study only tracked changes in symptoms. With hopes of future confirmation that this treatment may slow disease progression, the authors conclude that, at this time, HCQ can be considered useful in OA based on the success in symptom reduction seen in this study.10 Bryant et al This was a retrospective observational trial12 looking at similar patients that had received the same treatment of hydroxychloroquine over a period of time. The authors wanted to know whether HCQ provided the primary outcome of symptomatic relief for patients with erosive
10
subset of osteoarthritis. The authors started with 31 records of patients who met criteria for diagnosis of erosive OA, and pared down the group with inclusion criteria to a group of patients with complete records, similar baseline characteristics, and same dosage of HCQ (200mg bid) over a period of at least 7 months. This resulted in 8 patients who had radiographic changes showing OA in their PIP and DIP joints, and who also had complete documentation to review for treatment effect.12 Symptomatic improvement was measured by a three-pronged “overall response,” which included evaluation of morning stiffness, synovitis, and patient global assessment. In order to be considered a responder to treatment, the patient had to have decreased morning stiffness (50% less in duration), resolution of synovitis in at least one joint or reduction of synovitis in at least two joints, and improvement of patient global assessment by a point or more. The baseline ESR was recorded for all patients, with an average of 20, but a post-treatment value was not taken.12 Results measured data from the scoring system pre-treatment with HCQ and at 7 mos to determine if patients could be classified as a responder to the therapy. In 6 of the 8 patients the treatment was considered effective, and they had achieved response meeting the MID (minimum important difference) in the evaluation system measuring symptomatic improvement. The other two patients also experienced decreased synovitis, but their response did not meet the MID at 7 months. This anchor-based evaluation determined a 75% response, but without a placebo control, the RR or NNT again could not be calculated. This doesn’t translate easily to an effect change on the Cohen index, but with the majority of patients meeting the MID, this can be considered a “moderate” effect magnitude. The authors concluded that they had confirmed that HCQ “has utility in erosive OA,” and recognized that prospective randomized trials are important for further validation.12
11
Punzi et al This was a randomized placebo-controlled trial,11 and was the only study that looked at both symptomatic improvement, as well as physiological markers pre and post treatment with HCQ. The patient population in their study had erosive OA and had not responded well to traditional analgesics including NSAIDs. Inclusion criteria specified that patients had similar radiographic evidence of erosive OA of their PIP and DIP joints, and all individuals were screened with exclusion criteria for presence of any other rheumatic diseases.11 In the study, 15 patients were randomly allocated to receive either HCQ (200mg) or traditional analgesics and NSAIDs for 12 months. Measurements were taken at baseline, 6 mos, and 12mos, and included a Ritchie index for joint tenderness, and physiological markers including ESR and sIL-2R.11 Results showed improvement in all three measurements for the treatment group, which was to a greater extent than the placebo group. There was no MID determination for treatment responder, so the Cohen index was used to look at effect size and magnitude. The Ritchie index values decreased from 6.60 to 3.31 in the HCQ group, and from 5.31 to 4.54 in the non-HCQ group. This was a “large” effect magnitude when looking at improvement in the treatment group compared to the control, as seen in Table 1. Physiological inflammatory marker ESR was reduced from 23.01 to 16.17 in patients treated with HCQ, and from 23.62 to 20.34 in the control patients. The marker for sIL-2R also had a significant change from 119.67 to 69.23 in the HCQ group, compared to the placebo group where the lab value went from 106.78 to 96.42. These two markers representing secondary outcome of disease modulation translate to an effect size that is of medium-large magnitude on the Cohen index, as seen in Table 1.11
12
The authors concluded that HCQ was efficacious in causing a positive clinical response. They note that it is possible that articular changes may be modified by hydroxychloroquine, and though further validation is needed, there is a beneficial role for the medication in erosive subsets of OA.11 DISCUSSION In synthesizing the results from these three small studies, the consensus was that hydroxychloroquine does have utility in providing symptomatic improvement in patients with osteoarthritis, more specifically OA involving the knee and the subset of erosive OA involving finger joints. There is some evidence for the immunomodulatory capability of HCQ, but its utility in the alteration of disease progression needs additional research, ideally with both labs for physiological markers and radiographic monitoring. The treatment at dosage of 200mg bid was tolerated well, with the only reported ADRs across all three studies being rash in two patients and vertigo in one patient.10 There remains a risk of rare choloroquine-induced damage to the eye, which would need appropriate monitoring via the baseline ophthalmologic exam and additional exam at the 5 year mark in prolonged use.7 As an affordable, easy to take medication, HCQ should be kept in mind as an offlabel treatment to use in clinical practice for patients who do not respond well to APAP or NSAIDs, and do not wish to move to more invasive interventions such as injections or surgery. In addition to being a treatment resistant analgesic option, the shift towards altering disease progression is an important area of study. Further considerations include novel injectable treatments not yet covered by insurance, including platelet-rich plasma (PRP) and stem cell therapy (MSC). While acetaminophen and NSAIDs are a good place to start for initial
13
symptomatic control, the prospect of being able to slow disease progression is definitely something that is a hopeful prospect for both healthcare providers and patients. In appraising the current evidence, some of the issues in variability across studies were the specification of erosive/inflammatory arthritis, and the differences in focus on hand joints vs. knee joints, however, all patients fell under the category of OA. There was also variability in what scale or measurement (i.e. WOMAC, Ritchie index) was used to determine symptomatic change, but all clearly addressed whether the joint had become less painful with treatment. Other important limitations were the small number of patients in the studies, with the largest study being only 44 people. The populations of two of the studies10,12 included only women, although they were multiracial and covered an age range from 39-77; the other study11 did not specify its population characteristics. There was randomization, but not specified blinding in the Punzi et al study,11 which was sufficient to downgrade its quality level. The Jokar et al study10 did not have any serious limitations. Looking then at the overall GRADE quality16 of the studies, downgrades occurred due to small sample size and unclear blinding. Additionally, there is inherent “low” quality of the retrospective observational study in comparison to RCTs. These limitations meant that there was an overall “low” quality of evidence for the outcome of symptomatic improvement. Given the single study11 with a very small sample size, the quality of evidence was “very low” for the outcome of disease modulation. (See Table 1) Moving forward from the synthesis of current evidence, clinicians can look to what is happening with the use of hydroxychloroquine as treatment in osteoarthritis research today. In the search performed for this review, multiple well-designed study protocol outlines were found, OA TREAT17 and HERO,18 which looked to better explore the use of HCQ in erosive and non-
14
erosive hand OA; however, there was no information on the activity of these studies, other than some leads that suggested recruiting was near completion. One study for small joint OA, FABIO,8 has a completed status on the NIH site, and a HCQ/statin combination drug is currently in progress as a trial for knee OA.9 Aside from these pending findings, a larger RCT for large joint OA is definitely needed to follow the positive results of the Jovac et al study;10 more importantly, studies looking at physiological markers and radiographic changes are needed to establish the connection of HCQ to the disease process of OA. CONCLUSION Hydroxychloroquine can be considered for treatment of osteoarthritis in patients, and is currently used anecdotally for patients who are resistant to initial analgesics such as acetaminophen and NSAIDs. Its disease modifying potential, though proven in RA, has not been well established for OA. Given the current evidence of low quality, symptomatic relief can be seen as a positive primary outcome with HCQ treatment, with minimal evidence for disease modulation. Further clinical studies will validate whether hydroxychloroquine does provide both symptomatic relief and disease modulation, and will better define the population of patients with OA—whether small, large joint, or both—in which HCQ treatment may provide the most benefit.
15
References 1. Centers for Disease Control and Prevention (CDC). Prevalence of doctor-diagnosed arthritis and arthritis-attributable activity limitation--united states, 2010-2012. MMWR Morb Mortal Wkly Rep.2013 Nov 8;62(44):869-73.
2. Elders MJ. The increasing impact of arthritis on public health. J Rheumatol Suppl.2000 Oct;60:6-8.
3. Buckwalter JA, Lotz MK, Stoltz J. Osteoarthritis, inflammation and degradation: A continuum. Vol 70. IOS Press; 2007.
4. Lapane KL, Yang S, Driban JB, et al. Effects of prescription nonsteroidal antiinflammatory drugs on symptoms and disease progression among patients with knee osteoarthritis. Arthritis & Rheumatology. 2015;67(3):724-732.
5. Abramson SB. Do nonsteroidal anti-inflammatory drugs accelerate disease progression in osteoarthritis?. Nature Clinical Practice Rheumatology. 2006;2(6):302-303.
6. Vuolteenaho K, Kujala P, Moilanen T, Moilanen E. Aurothiomalate and hydroxychloroquine inhibit nitric oxide production in chondrocytes and in human osteoarthritic cartilage. Scand J Rheumatol. 2005;34(6):475-479.
7. Browning DJ. Impact of the revised american academy of ophthalmology guidelines regarding hydroxychloroquine screening on actual practice. Am J Ophthalmol. 2013;155(3):418-428.e1.
16
8. WeiChing Lee MH. Pharmacological treatment in Osteoarthritis (FABIO). https://clinicaltrials.gov/ct2/show/NCT01148043?term=hydroxychloroquine+AND+osteoarthriti s&rank=1. Accessed June 1, 2015.
9. Genovese M. Hydroxychloroquine/atorvastatin in the treatment of Osteoarthritis (OA) of the knee. https://clinicaltrials.gov/ct2/show/NCT01645176?term=osteoarthritis+and+hydroxychloroquine &rank=2. Accessed June 1, 2015.
10. Jokar M, Mirfeizi Z, Keyvanpajouh K. The effect of hydroxychloroquine on symptoms of knee osteoarthritis: A double-blind randomized controlled clinical trial. Iranian Journal of Medical Sciences. 2013;38(3):221-226.
11. Punzi L, Bertazzolo N, Pianon M, Michelotto M, Todesco S. Soluble interleukin 2 receptors and treatment with hydroxychloroquine in erosive osteoarthritis. J Rheumatol. 1996;23(8):14771478.
12. Bryant LR, des Rosier KF, Carpenter MT. Hydroxychloroquine in the treatment of erosive osteoarthritis. J Rheumatol. 1995;22(8):1527-1531.
13. Robertson C, Rice J, Allen N. Treatment of erosive osteoarthritis with hydroxychloroquine. Arthritis Rheum. 1993;36(9):S167-S167.
14. Guyatt G, Rennie D, Meade M, et al. Users' guides to the medical literature: A manual for evidence-based clinical practice. Second Edition ed. McGraw Hill Professional; 2008.
17
15. Cohen J. Statistical power for the social sciences. Hillsdale, NJ: Laurence Erlbaum and Associates. 1988.
16. GRADE Working Group. Grading of recommendations assessment, development and evaluation. http://www.gradeworkinggroup.org/. Updated 2014. Accessed May 23, 2015.
17. Detert J, Klaus P, Listing J, et al. Hydroxychloroquine in patients with inflammatory and erosive osteoarthritis of the hands (OA TREAT): Study protocol for a randomized controlled trial. Trials [Electronic Resource]. 2014;15:412.
18. Kingsbury SR, Tharmanathan P, Adamson J, et al. Hydroxychloroquine effectiveness in reducing symptoms of hand osteoarthritis (HERO): Study protocol for a randomized controlled trial. Trials [Electronic Resource]. 2013;14:64.
18
TABLE 1
Characteristics of Reviewed Studies, GRADE profile: HCQ as treatment for osteoarthritis Quality Assessment
Summary of Findings
Downgrade Criteria
No. of Studies
Design
Limitations
Indirectness
Imprecision
No serious indirectness
Small sample size
Number of Patients
Inconsistency
Study
HCQ
Placebo or no treatment
Jokar et al10
21
23
Bryant et al12
8
0
Punzi et al11
7
8
Punzi et al11
7
8
Publication bias likely
Effect Effect Size (ES), Adjusted ESa
Quality
Importance
Low
Important
Very Low
Important
Effect Magnitudea
Symptomatic improvement
3
2 RCT 1 Retrospect Observational
Blinding not specified (Punzi et al11)
No serious inconsistencies
No bias likely
0.84, 0.98 75% meet MIDb 0.70, 1.07
mediumb
0.70, 0.60c 0.63, 0.87d
med-large med
large
large
Disease modulation (via ESR, sIL-2R)
1
1 RCT
Blinding not specified (Punzi et al11)
No serious indirectness
Small sample size
No serious inconsistencies
No bias likely
GRADE: Grading of Recommendations, Assessments, Development and Evaluation. aCohen
d index and adjustment for difference in size of placebo/treatment groups, pre/post pre/post- treatment evaluation; magnitude determined by Cohen chart15 approach with MID (minimum important difference) defined as im improvement provement of at least one level on patient global assessment score, which determined patient as responder; 75% of group were then considered responders, which was not translated to an effect magnitude, but can be consider considered ed a moderate change. cAssessment off change in ESR and effect size, adjusted effect size dAssessment of change in sIL-2R 2R and effect size, adjusted effect size bAnchor-based based
FIGURE 1
Changes in WOMAC total score from baseline (Jovac et al10)
19