Health Care for All Persons with Down Syndrome March 21, 2014
George T Capone, M.D. Kennedy Krieger Institute, Baltimore Maryland
Health Care for All Persons with Down Syndrome Persons with Down syndrome are living longer • • • •
Recognition of specific health conditions, treatment and prevention Health promotion to physicians, families & individuals Increased availability & access to health care Improved opportunities for participation in clinical research
Improvements in health care have been “uneven” • Limited by access to medical knowledge, resources or implementation of best practices • Challenge of providing care to complex individuals • Much to be done!
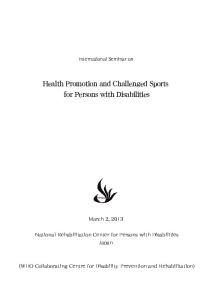
Estimate of Down Syndrome Population Prevalence in the United States in 2008 The Journal of Pediatrics, (2013) Volume 163, Issue 4, 1163-1168; A Presson , G Partyka , K. M. Jensen, et al.
60y
Age at Death
53y 47y
Figure 2 Mean, median, and 25th and 75th percentiles for age at death in persons with Down syndrome, 19002007. The mean and median age at death for persons with Down syndrome have increased significantly over the past 40 years.
Need for Regular & Sustained Health Care Increased prevalence of specific medical conditions • Birth anomalies and medical conditions in newborn • Acquired medical conditions in children & adolescents • Acquired & age-related medical conditions in adults
Possible Barriers Down syndrome/ID - unfamiliar to primary care providers Presentation - unusual, atypical, complicated picture Complexity - multiple, co-occurring conditions, overshadowing
Regular & Sustained Health Care Does regular screening and early treatment improve individual health outcomes and quality of life
Yes To what degree? Depends on condition and functional outcome being measured • • •
Vision & Hearing impairment Heart & Gastrointestinal defects Leukemia, Thyroid disease
Health Care Around the World Down Syndrome International (DSi) Lists organizational contacts in 121 countries Down Syndrome International http://www.ds-int.org/medical NLM PubMed Search: Articles for medical providers on Health Care for people with Down syndrome •
English, Spanish, Portuguese, German, French, Dutch, Finnish, Norwegian, Chinese, Japanese..
Health Care Professionals: Down Syndrome Medical Interest Groups • DS Clinics, Special Interest Groups and Research Networks • Annual Conferences: United States, United Kingdom • WDSC: Dublin (2009), Cape Town (2012), Chennai (2015), Glasgow (2018)
Health Care for Down syndrome AAP Health Supervision Guidelines (2011)
http://pediatrics.aappublications.org/content/128/ 2/393.long English & Spanish Versions
NIH Down Syndrome Consortium
http://downsyndrome.nih.gov/Pages/default.aspx Resources
NLM Medline Plus
http://www.nlm.nih.gov/medlineplus/downsyndro me.html Search Down Syndrome
AAP Health Supervision for Children with Down Syndrome Pediatrics (2011) Volume 128, Issue 2, 393-406 Bull, M. and the AAP Committee on Genetics
AAP Guidelines for DS available since 1994, revised in 2001, 2011 Based on expert opinion as supported by published evidence Organized by chronologic age Provides guidance to Primary Care Providers across various settings (U.S.)
Emphasis: Screening & diagnosis for common medical conditions Increased vigilance & monitoring in asymptomatic individuals Anticipatory guidance specific to DS/ID Access to best information and community resources Action items: Assess, Evaluate, Verify, Obtain, Measure, Administer & Refer Anticipatory Guidance: Review, Educate, Discuss & Counsel
Newborn Period (Birth-30 days) Actionable items based on physical findings and increased prevalence. No single infant has all these conditions Anatomical: Cardiac defect, GI obstruction, Upper respiratory (apnea, stridor) Vision impairment (cataracts) Functional: GI-Feeding-Elimination (swallow, reflux, obstruction), Hearing (loss), Thyroid hormone (low), Blood count (elevated WBCs, RBCs) Required Evaluations: Careful examination, Cardiac ECHO*, Thyroid hormone, Blood count, Hearing, Vision As Needed Evaluations: Abdominal imaging, apnea monitoring, swallow study, specialty consultation as required
Newborn Cardiac Screening Archives of Diseases in Childhood 95:95-98 (2010) Dennis, J Archer, N, Ellis, J and Marder, L.
CHD 40-50%, AV Canal 15-20% Surgical intervention during early infancy is mandatory
Withholding surgical intervention results in preventable morbidity and mortality Every newborn with DS should be evaluated for Cardiac defect in the first 12 weeks of life Abnormal CARDIAC ECHO Team management & action plan developed for each child by 4-6 weeks
Infant & Young Child (1mo-5yr) Actionable items based on physical findings and increased prevalence. No single child has all these conditions Surgical-Medical Followup: Cardiac repair (septum and valves), GI, Feeding, Upper Respiratory, Vision, Hearing, Blood, Thyroid Sustained Vigilance: Heart and GI function, Feeding problems, Gluten sensitivity, Obstructive apnea, Aspiration, GE Reflux, Hearing loss, Middle ear fluid, Visual function, Anemia, Thyroid disorders, Cervical myelopathy, Behavior Ongoing Evaluations: ENT, Hearing, Thyroid, Iron (Ferritin), Growth rate, Dental, Development-Behavior, Infantile seizures, Sleep - Vaccinations, Routine care As Needed Evaluations: Feeding, Swallowing, Sleep, Endoscopy, EEG, Cervical Xray
Medical Guidance for Adults
?
Based on physical findings and increased prevalence *consensus needed* Medical Followup: according to previous history Sustained Vigilance: Younger Adult: Sleep Apnea, Obesity, Mitral/Aortic Valve leak, Moodanxiety disorder, Functional decline, Osteoporosis, Gait changes, Cervical Spondylosis, Hypotension Older Adult: (>45yr) Seizures, Motor and Intellectual Impairment (AD-type) Ongoing Evaluations: Weight (BMI), Nutrition, Fitness-exercise, Thyroid, Vitamin D, Cholesterol, Vision, Hearing, Dental, Females: Routine GYN care
Health Care Challenges Ahead Health Care Providers • Implementation of guidelines requires time & expertise • Access to specialty consultation & resources • Guidance for Adults and individuals with complex conditions Family & Advocacy Organizations • How to educate families to anticipate medical needs • Need to translate & codify the recommendations • Work collaboratively with Primary Care Providers Nations of the World • Practice guidelines specific to each country-region, culture • Practical consideration of existing health resources • Commitment to improve access to resources
Health Care is a Shared Responsibility Families, Advocates Primary Care Providers & Specialists Policy Makers & Governments NGO’s All Parties must Commit to investing in healthcare for people with DS Strengthens the person, family ...Strengthens the community, workforce, nation ...and reaffirms what is best about our shared humanity
Thank you! Gracias Obrigado Merci 谢谢 Спасибі Grazie Tack Go raibh maith
ਤੁਹਾਡਧੰ ਨਵਾਦ þakka þér kiitos
ขอบคุณ
спасибо dziękuję Dank u Dankie ありがとう