Clinical Science (1999) 97, 579–584 (Printed in Great Britain)
Baseline heart rate variability in healthy centenarians: differences compared with aged subjects (� 75 years old) Giuseppe PAOLISSO, Daniela MANZELLA, Michelangela BARBIERI, Maria Rosaria RIZZO, Antonio GAMBARDELLA and Michele VARRICCHIO Department of Geriatric Medicine and Metabolic Diseases, Servizio di Astanteria Medica, Piazza Miraglia 2, I-80138 Napoli, Italy
A
B
S
T
R
A
C
T
Healthy centenarians have better anthropometric, endocrine, metabolic and immunological parameters than aged subjects (� 75 years old). Heart rate variability (HRV) has been demonstrated to be a good index of the cardiac autonomic nervous system. It is not known whether there are any differences in cardiac autonomic nervous system activity between aged subjects and healthy centenarians. It is possible that differences in cardiac autonomic nervous system activity could represent one of a cluster of factors explaining the extreme survival of centenarians. Thus we aimed to answer the following question : is there any difference in baseline HRV parameters between aged subjects and healthy centenarians ? Therefore power spectral analysis of HRV at baseline was investigated in 25 aged subjects (age � 75 years) and 30 healthy centenarians (age � 100 years). Anthropometric measurements were made in all subjects, fasting blood samples were drawn for metabolite determinations, and HRV was determined. Independent of age, gender, body mass index and fasting plasma noradrenaline and free 3,3h,5-tri-iodothyronine concentrations, healthy centenarians had lower basal values for total power (1318p546 compared with 1918p818 ms2 ; P 0.01) and the low-frequency component (33p21 compared with 50p11 normalized units ; P 0.03) and a higher value for the highfrequency component (77p15 compared with 61p18 normalized units ; P 0.05) than aged subjects. Consequently, the low-frequency/high-frequency ratio (0.43p0.07 compared with 0.91p0.05 ; P 0.02) was also lower in the healthy centenarians than in the aged subjects. Our study demonstrates that the basal low-frequency/high-frequency ratio, an indirect index of cardiac sympathovagal balance, is lower in healthy centenarians than in aged subjects.
INTRODUCTION Power spectral analysis of heart rate variability (HRV) provides a non-invasive method of estimating cardiac sympathetic and parasympathetic activity [1], and it can detect autonomic nervous dysfunction even in the preclinical stage [2]. Several studies have reported that HRV decreases with age, suggesting an age-dependent decline
in autonomic nervous system (ANS) activity in subjects aged between 60 and 85 years [2,3]. To the best of our knowledge, no study has evaluated HRV in healthy centenarians. This latter group of subjects has been shown to have anthropometric characteristics [4], endocrine and metabolic profiles [5–8] and immunological parameters [9] different from those of aged subjects (� 75 years old). Thus one cannot exclude the possibility that healthy
Key words : aged subjects, healthy centenarians, heart rate variability, plasma noradrenaline. Abbreviations : ANS, autonomic nervous system ; BMI, body mass index ; f T , free 3,3h,5-tri-iodothyronine ; HF, high-frequency ; $ HRV, heart rate variability ; LF, low-frequency ; VLF, very-low-frequency. Correspondence : Dr Giuseppe Paolisso (e-mail gpaoliss!tin.it).
# 1999 The Biochemical Society and the Medical Research Society
579
580
G. Paolisso and others
centenarians may show HRV characteristics, and thus cardiac ANS activity, different from those of aged subjects. In the light of such experimental evidence, the present study aimed at investigating potential differences between aged subjects and healthy centenarians in baseline power spectral analysis of HRV. Thus power spectral analysis of HRV was investigated in 25 aged subjects and 30 healthy centenarians.
METHODS Subjects A total of 25 aged subjects [age 78p0.7 years (meanpS.D.)] and 30 healthy centenarians (age 102p0.8 years), without a family history of diabetes, obesity or hypertension, volunteered for the study. All subjects were normotensive, were not taking any medication, were non-smokers and showed no evidence of metabolic or cardiovascular diseases. Oral glucose tolerance [10] (75 g of glucose) was tested in all volunteers before being enrolled. Subjects with a family history of type II diabetes mellitus, or suffering from obesity [body mass index (BMI) � 30] or hypertension, were excluded from the study. No women were or had been taking hormonereplacement therapy during or before the study. Subjects with a change in body weight of � 2 kg during the preceding year, or with Alzheimer’s disease or secondary dementia, were excluded from the study. Subjects were always studied in the supine position. All tests were performed in the morning after an overnight fast (at least 12 h). After a clear explanation of the potential risks of the study, all volunteers (as well as their relatives for centenarians) provided written informed consent to participate into the study, which was approved by the Ethical Committee of our Institution.
Anthropometric determinations Weight and height were measured using standard techniques. Fat-free mass was measured using a four-terminal bio-impedance analyser (RJL Spectrum Bioelectrical Impedance-BIA 101\SC Akern ; RJL-System, Florence, Italy) as previously reported [4]. Waist and hip circumferences were measured to the nearest 0.5 cm with a plastic tape, and the waist\hip ratio was calculated.
Analytical methods Plasma glucose was determined immediately by the glucose oxidase method (Beckman, Fullerton, CA, U.S.A.). Blood samples for haematocrit measurements were collected in heparinized tubes. After centrifugation (10 000 g ; 5 min), plasma concentrations of leptin (Linco Research, St. Louis, MO, U.S.A. ; coefficient of variation 4.5p0.5 %) and free 3,3h,5-tri-iodothyronine (f T ) (Bio$ data Milan, Italy ; coefficient of variation 3.8p0.6 %) # 1999 The Biochemical Society and the Medical Research Society
were determined by radioimmunoassay. Plasma catecholamine concentrations were determined by HPLC.
Cardiovascular determinations Blood pressure was recorded using a standard mercury sphygmomanometer (diastolic blood pressure, corresponding to Korotkoff’s phase V). All determinations were carried out with the subject at rest after 15 min in the supine position, on three occasions separated by intervals of 5 min ; the mean value of the three measurements was then calculated. Respiratory frequency was also calculated over a period of 2 min before the test. Subjects with a respiratory rate of less than 10 breaths\ min (i.e. 0.15 Hz) were excluded from the study [11] in order to avoid the overlap of oscillations of low and high frequency at spectral analysis. Ambulatory electrocardiographic monitoring was performed with two-channel frequency-modulation tape recorders (Remco Italia Cardioline AD 35 ; recorder model number LP103). After careful skin preparation, the electrodes were placed on the chest in order to obtain the bipolar chest leads CM1 (modified V1) on the first channel and CM4 (modified V4) on the second channel. Holter monitoring started at 08.00 hours for a period of 300 min (60 min for baseline and 240 min after glucose ingestion). Two independent ‘ blind ’ investigators analysed the ambulatory electrocardiographic recording tapes using the program Holter AD35 TOP (Remco Italy Cardioline). Ectopic beats were corrected for linear interpolation with the adjacent complexes. Electrocardiographic tracings with � 1 % premature beats were eliminated from the analysis. Stationary sections of data of appropriate length were selected for analysis. From the surface ECG, the computer program first calculates the interval tachogram and stores them in memory. From tachogram sections of adequate length and stationarity, the computer program automatically calculates simple statistics and the best autoregressive estimate of power spectral density. Autoregressive spectral analysis was undertaken after estimation of model coefficients using the Levinson– Durbin algorithm. The model order selection was performed according to the Akaike information criterion [12]. Spectral components were identified and estimated using the spectral-decomposition algorithm proposed by Johnsen and Andersen [13] and were then assigned, on the basis of their central frequency, to one of the three bands : the very-low-frequency (VLF) band (from 0 to 0.03 Hz), the low-frequency (LF) band (from 0.03 to 0.15 Hz) or the high-frequency (HF) band (from 0.15 to 0.45 Hz). Since the physiological explanation of the VLF component is much less well defined and the existence of a specific physiological process attributable to those heart period changes have been strongly questioned [1], only LF and HF periods were usually considered. LF
Heart rate variability in centenarians
Table 1
Characteristics of study groups
All plasma metabolites were measured in fasted subjects. Results are meanspS.D. Statistically significant differences compared with aged subjects : *P
Age (years) Gender (male/female) Systolic blood pressure (mmHg) Diastolic blood pressure (mmHg) BMI (kg/m2) Fat-free mass (%) Waist/hip ratio Albumin (g/l) Lymphocytes (cells/mm3) Plasma triacylglycerols (mmol/l) Plasma non-esterified fatty acids (mmol/l) Plasma total cholesterol (mmol/l) Plasma noradrenaline (nmol/l) Plasma adrenaline (pmol/l) Plasma leptin (ng/ml) Plasma fT3 (pmol/l)
0.05.
Aged subjects (� 75 years) (n l 25)
Healthy centenarians (� 100 years) (n l 30)
78p0.7 11/14 125p4.4 80p2.1 25.8p0.4 61.7p1.8 0.87p0.02 3.8p0.7 2.418p218 1.2p0.3 395p78 5.1p0.9 2.6p0.2 318p61 13.8p7.9 5.1p0.04
102p0.8 12/18 120p5.3 80p3.2 22.2p0.5* 57.8p0.7* 0.83p0.04* 3.6p1.0 2.215p2.38 1.1p0.5 318p71* 4.8p0.8 2.4p0.2 301p66 10.9p4.1* 4.8p0.5
and HF are reported in normalized units that represent the relative value of each power component in proportion to the total power minus the VLF component [1]. Normalized units tend to minimize the effect on the values of the LF and HF components of changes in total power [1]. The respiratory rate for data analysis was obtained from the central frequency of the HF component [14]. Before recordings were carried out, all patients were asked to rest comfortably in the supine position for at least 30 min. Efforts were made to keep patients unaware of the sampling timing to avoid circumstances that might affect heart rate ; furthermore, all subjects were accustomed to breathing at a constant rate and were advised to avoid talking during the study.
Statistical analyses All results are presented as meanspS.D. Because the distribution of the frequency domain measures of both HRV and plasma leptin concentration were extremely skewed, each value was also logarithmically transformed to improve normality for statistical testing and backtransformed for presentation in the Tables. ANOVA (analysis of variance) was used to assess differences between the two study groups. Simple linear regression analysis was carried out using standard techniques. ANCOVA (analysis of co-variance) was used to adjust basal total power, the LF and HF components and the LF\HF ratio for age, gender, BMI, and plasma noradrenaline (norepinephrine) and fT concentrations. A P $ value of 0.05 was chosen as the level of significance. All calculations were carried out on an IBM PC using the SOLO software package (BMDP, Cork, Ireland).
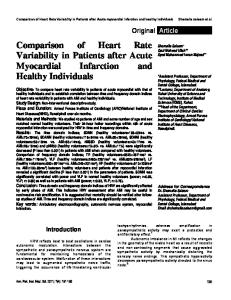
RESULTS The clinical characteristics of the subjects are reported in Table 1. The healthy centenarians were leaner and had a more peripheral body fat distribution than the aged subjects. Fasting plasma urea, creatinine, liver enzymes and total protein concentrations were similar in the two groups, and within the normal range (results not shown). Similarly, fasting plasma adrenaline, noradrenaline and f T concentrations were not different between the two $ groups, while the plasma leptin concentration was lower in the centenarians than in the aged subjects. A typical pattern of baseline spectral analysis in one centenarian and in one aged subject are reported in Figure 1, while the mean values for both groups are shown in Table 2. Healthy centenarians had lower values for total power and the LF component, but higher values for the HF component and for the R–R interval, than the aged subjects. Consequently the LF\HF ratio was lower in the healthy centenarians than in the aged subjects. Independent of age, gender, BMI and fasting plasma noradrenaline and f T concentrations, differences between $ healthy centenarians and aged subjects in basal total power (1318p546 and 1918p818 ms# respectively ; P 0.01), the LF component (33p21 and 50p11 normalized units respectively ; P 0.03), the HF component (77p15 and 61p18 normalized units respectively ; P 0.05) and the LF\HF ratio (0.43p0.07 and 0.91p0.05 respectively ; P 0.02) were apparent. In the aged subjects, the baseline LF\HF ratio was correlated significantly with the BMI (r l 0.48 ; P 0.01), the waist\hip ratio (r l 0.45 ; P 0.02), and the fasting plasma insulin (r l 0.49 ; P 0.01) and nor# 1999 The Biochemical Society and the Medical Research Society
581
582
G. Paolisso and others
Figure 1
Table 2
Spectral pattern from typical registration for one healthy centenarian (A) and one aged subject (B)
Differences in baseline power spectral analysis of HRV parameters between aged subjects and healthy centenarians
All results are meanspS.D. n.u., normalized units ; CHF, central high frequency.
R–R interval (ms) Total power (ms2) LF (ms2) LF (n.u.) HF (ms2) HF (n.u.) LF/HF CHF (Hz)
Aged subjects (� 75 years) (n l 25)
Healthy centenarians (� 100 years) (n l 30)
P
825p15 2050p935 634p118 51p15 698p130 59p20 0.95p0.03 0.21p0.03
951p10 1257p621 510p96 29p20 742p108 71p18 0.41p0.08 0.25p0.02
0.001 0.001 0.020 0.001 0.050 0.030 0.010 0.050
adrenaline (r l 0.57 ; P 0.02) concentrations. No such correlations were found for the healthy centenarians.
DISCUSSION The present study demonstrates that our healthy centenarians had values for the baseline LF component and the LF\HF ratio (an index of cardiac sympathovagal balance) that were significantly lower than those of aged control subjects. Such a difference does not seem to be due only to advancing age. HRV analysis is a useful method to investigate ANS activity at the cardiac level. In fact, in the spectral analysis we mainly recognize two # 1999 The Biochemical Society and the Medical Research Society
peaks : HF and LF. Efferent vagal activity is a major contributor to the HF component, as seen in clinical and experimental observations of autonomic manoeuvres such as electrical vagal stimulation, muscarinic receptor blockade and vagotomy [1]. More debated is the interpretation of the LF component, which is considered to be a marker of sympathetic modulation (especially when expressed in normalized units) or a parameter including both sympathetic and vagal influence [1]. This discrepancy is due to the fact that, in some conditions associated with sympathetic excitation, a decrease in the absolute power of the LF component is observed [1]. Consequently, the LF\HF ratio is considered to be an indirect index of sympathovagal balance [15,16]. Furthermore, it is important to point out that during sympathetic
Heart rate variability in centenarians
stimulation there is an increase in heart rate that is usually accompanied by a marked reduction in total power, whereas the reverse occurs during vagal stimulation. When the spectral components are expressed in absolute units (ms#), the changes in total power influence the LF and HF components in the same direction and prevent the appreciation of the fractional distribution of energy. Due to the reduction in total power, the LF component appears unchanged if considered in absolute units. However, after transformation of the LF and HF components in normalized units, an increase in the LF component or the LF\HF ratio is evident [1]. Healthy centenarians are a very select group of subjects in whom ‘ successful aging ’ is present. The reason for such successful aging is unknown. Lifestyle [17], environmental factors [17], and anthropometric [4], endocrine and metabolic characteristics [5–9] may explain this successful aging. Whether cardiac ANS activity also plays a role has not been investigated previously. Our study shows that the baseline LF\HF ratio and LF component were lower in healthy centenarians than in aged subjects. To the best of our knowledge, this is the first report of HRV in healthy centenarians. Several hypotheses can be suggested for explaining our results. In vitro and in vivo data show that resting heart rate appears to be only slightly changed by aging in healthy adult humans, while the heart rate response to exercise, to βadrenergic stimulation and blockade and to parasympathetic blockade with atropine diminishes with aging [18,19]. Beat-to-beat variability of heart rate also decreases with increasing age [20,21]. In particular, decreases in heart rate responses and beat-to-beat variability have been attributed to age-related alterations in the autonomic regulation of sinus node function [2,3]. Furthermore, HRV as measured by the standard deviation of the R-R intervals at all frequencies of the heart rate power spectra is found to be decreased by aging when measured in the baseline supine state [22]. Under supine conditions and during normal breathing conditions, the relative balance between LF and HF components does not differ between young and older subjects [23]. On the other hand, the finding that agerelated differences in HRV in the supine state were largely eliminated by the administration of atropine and propranolol suggests that age-related differences in HRV, in contrast with those in heart rate, can be explained solely on the basis of parasympathetic and β-adrenergic influences [18,19]. Thus one can conclude that differences between aged subjects and healthy centenarians might be due to a negative impact of advancing age on ANS activity. Such a hypothesis is consistent with previous data showing that total power, the expression of global variability and hence of global control over sympathovagal interaction, is diminished in subjects aged over 64 years [3], and with our data demonstrating lower values for basal total power and the LF component in healthy
centenarians than in aged subjects. Similar considerations are also useful to explain the behaviour of the LF\HF ratio at baseline. In our study, the baseline HF component was higher in healthy centenarians than in aged subjects. A potential protective effect of a high HF component against cardiac mortality has been suggested recently in a prospective manner by the ATRAMI study [23]. According to Piccirillo et al. [3,24], one can hypothesize that an elevated HF component in healthy centenarians might depend not only on the increased HF power but also on an unbalanced relationship between the LF and HF components. Alternatively, one may also hypothesize that healthy centenarians might be a very select group of subjects whose basal LF\HF ratio reflects a genetically determined lower adrenergic tone compared with aged control subjects. Several observations seem to support such a hypothesis. Firstly, previous studies have shown several differences between aged subjects and healthy subjects [4–9]. Secondly, independent of age, BMI, and plasma noradrenaline and fT concentrations, $ the basal LF\HF ratio was still lower in healthy centenarians than in aged subjects. Lastly, preliminary data on aged individuals with centenarian parents demonstrated that their basal LF\HF ratios were lower than those of age-, gender- and BMI-matched control subjects (G. Paolisso, D. Manzella, M. Barbieri, M. R. Rizzo, A. Gambardella and M. Varricchio, unpublished work). In conclusion, our study demonstrates that baseline values of the LF component and of the LF\HF ratio, an indirect index of cardiac sympathovagal balance, are lower in healthy centenarians than in aged subjects. Further studies should investigate whether such differences are merely due to advancing age, or represent a phenotypic characteristic of a selected genetic background.
REFERENCES 1 Task Force of the European Society of Cardiology and the North American Society of Pacing and Electrophysiology (1996) Heart rate variability. Standards of measurements, physiological interpretation, and clinical use. Circulation 93, 1043–1065 2 Craft, N. and Schwartz, J. B. (1995) Effects of age on intrinsic heart rate, heart rate variability and AV conduction in healthy humans. Am. J. Physiol. 268, H1441–H1452 3 Piccirillo, G., Fimognari, F., Viola, E. and Marigliano, V. (1995) Age-adjusted normal confidence intervals for heart rate variability in healthy subjects during head-up tilt. Int. J. Cardiol. 50, 117–124 4 Paolisso, G., Gambardella, A., Balbi, V., D ’Amore, A. and Varricchio, M. (1995) Body composition, body fat distribution and resting metabolic rate in healthy centenarians. Am. J. Clin. Nutr. 50, 746–750 5 Mariotti, S., Barbesino, G., Caturegli, P., Franceshi, C. and Pinchera, A. (1993) Complex alteration of thyroid function in healthy centenarians. J. Clin. Endocrinol. Metab. 77, 1130–1134 6 Paolisso, G., Ammendola, S., Del Buono, A. et al. (1997) Serum levels of insulin-like growth factor-I and IGFbinding protein in healthy centenarians : relationship with
# 1999 The Biochemical Society and the Medical Research Society
583
584
G. Paolisso and others
plasma leptin and lipid concentrations, insulin action and cognitive function. J. Clin. Endocrinol. Metab. 82, 2204–2209 7 Paolisso, G., Gambardella, A., Ammendola, S., Balbi, V., Varricchio, M. and D’Onofrio, F. (1996) Glucose tolerance and insulin action in healthy centenarians. Am. J. Physiol. 270, E890–E896 8 Paolisso, G., Gambardella, A., Ammendola, S. et al. (1997) Preserved antilipolytic insulin action is associated with less atherogenic plasma lipid profile in healthy centenarians. J. Am. Geriatr. Soc. 45, 1504–1509 9 Sansoni, P., Cassarizza, A., Brianti, V. and Franceschi, C. (1993) Lymphocyte subset and natural killer activity in healthy old people and centenarians. Blood 82, 2767–2773 10 WHO Study Group. (1985) Diabetes Mellitus. WHO Tech. Rep. Ser. 727, 9–17 11 Brown, T. E., Beightol, L. A., Koh, J. and Eckberg, D. L. (1993) Important influence of respiration on human RR interval power spectra is largely ignored. J. Appl. Physiol. 75, 2310–2317 12 Kay, S. M. (1977) Modern Spectral Estimation : Theory and Application, pp. 221–237, Prentice Hall, Englewood Cliffs, NJ 13 Johnsen, S. J. and Andersen, N. (1978) On power estimation in maximum entropy spectral analysis. Geophysics 43, 681–690 14 Pinciroli, G., Rossi, R. and Vergani, L. (1985) Detection of electrical axis variation for the extraction of respiratory information. Comp. Cardiol. 11, 499–502 15 Malliani, A., Pagani, M., Lombardi, F. and Cerruti, S. (1991) Cardiovascular neural regulation explored in the frequency domain. Circulation 84, 1482–1492
16 Malliani, A., Lombardi, F. and Pagani, M. (1994) Power spectral analysis of heart rate variability : a tool to explore neural regulatory mechanisms. Br. Heart J. 71, 1–4 17 The Italian Multicenter Study on Centenarians (1995) I centenari in Italia : aspetti epidemiologici e clinico biologici. In Proceedings of 96th Meeting of the Italian Society of Internal Medicine, Pozzi (Rome, Italy), pp. 23–109, Italian Society of Internal Medicine, Rome 18 Ford, G. A., Hoffman, B. B., Vestal, R. E. and Blaschke, T. B. (1992) Age-related changes in adenosine and βadrenoreceptor responsiveness of vascular smooth muscle in man. Br. J. Clin. Pharmacol. 33, 83–87 19 Lakatta, E. G. (1993) Cardiovascular regulatory mechanism in advanced age. Physiol. Rev. 73, 9413–9467 20 Schwartz, J. B., Gibb, W. J. and Tran, T. (1991) Aging effects on heart rate variation. J. Gerontol. Med. Sci. 46, M99–M106 21 Sega, S., Jager, F. and Kiauta, T. (1993) A comparison of cardiovascular reflex tests and spectral analysis of heart rate variability in healthy subjects. Clin. Auton. Res. 3, 175–182 22 Stanley, G., Verotta, D., Craft, N., Siegel, R. A. and Schwartz, J. B. (1996) Age and autonomic effects on interrelationship between lung volume and heart rate. Am. J. Physiol. 270, H1833–H1840 23 La Rovere, M. T., Bigger, J. T., Marcus, F. I., Mortara, A. and Schwartz, P. J. (1998) Baroreflex sensitivity and heartrate variability in prediction of total cardiac mortality after myocardial infarction. Lancet 351, 478–484 24 Piccirillo, G., Fimognari, F. L., Munizzi, M. R., Bucca, C., Cacciafesta, M. and Margliano, V. (1996) Age-dependent influence on heart rate variability in salt-sensitive hypertensive subjects. J. Am. Geriatr. Soc. 44, 530–538 Received 16 March 1999/14 May 1999; accepted 22 July 1999
# 1999 The Biochemical Society and the Medical Research Society