A new generation of artificial ligaments in reconstruction of the anterior cruciate ligament TWO-YEAR FOLLOW-UP OF A RANDOMISED TRIAL T. Nau, P. Lavoie, N. Duval From the Hˆopital Notre Dame, Montréal, Canada
e have undertaken a randomised clinical trial comparing two methods of reconstruction of the anterior cruciate ligament in patients with chronic instability. We used an ipsilateral bone-patellartendon-bone autograft in 27 patients and the Ligament Advancement Reinforcement System (LARS) artificial ligament in 26. Assessment before and at two, six, 12 and 24 months after surgery, included the history, physical examination, a modified International Knee Documentation Committee (IKDC) score, the Tegner score, the Knee Injury and Osteoarthritis Outcome Score (KOOS) and instrumented laxity testing. There were no cases of reactive synovitis or of infection of the knee, and there was no difference regarding the failure rate between the two groups. The IKDC showed no significant differences between the two groups at any stage of the follow-up. The KOOS evaluation showed consistently better results in all subscales for the LARS group during the first year of follow-up. After 24 months these differences were no longer evident. Instrument-tested laxity was greater in the LARS group at all stages of follow-up, but the differences were not significant at 24 months. Our findings suggest that at follow-up at 24 months the LARS ligament seems to be a satisfactory treatment option, especially when an early return to high levels of activity is demanded.
W
J Bone Joint Surg [Br] 2002;84-B:356-60. Received 1 May 2001; Accepted after revision 3 August 2001
T. Nau, MD P. Lavoie, MD N. Duval, MD Laboratoire de Recherche en Imagerie et Orthopédie, Centre de Recherche du CHUM, Hˆopital Notre-Dame, Bureau Y1615, 1560 Rue Sherbrooke Est, Montréal, Canada H2L 4M1. Correspondence should be sent to Dr T. Nau at the Trauma Centre, University of Vienna Medical School, Waehringer Guertel 18-20, 1090 Vienna, Austria. ©2002 British Editorial Society of Bone and Joint Surgery 0301-620X/02/312400 $2.00 356
A number of different methods have been suggested for the treatment of the unstable, anterior-cruciate-ligament-deficient knee. The bone-patellar-tendon-bone (BPTB) autograft is commonly used for reconstruction of the anterior 1-3 cruciate ligament (ACL) and gives good results. The complications are mainly related to the harvesting of the graft and include fractures of the patella, rupture of the patellar tendon, the infrapatellar contracture syndrome and 4-7 patella baja. Reports of complications have increased and the use of artificial ligaments which avoids those complications may offer an alternative form of treatment. The use of synthetic material for ligament replacement was proposed in the 1980s. Poor results and high rates of failure were reported and the concept became less popular. Improved surgical techniques and new designs providing a more anatomical form of reconstruction may offer better results. The LARS artificial ligament (Ligament Advanced Reinforcement System; Surgical Implants and Devices, Arc-sur-Tille, France) has recently been reported to be a 8-10 suitable material. In 1996, encouraged by good early results we initiated a prospective, randomised controlled trial comparing two 10 techniques of reconstruction of the ACL. Our aim was to evaluate and compare the BPTB autograft and the LARS ligament in terms of clinical outcome and patient satisfaction.
Patients and Methods Between December 1996 and August 1998 we selected patients with closed growth plates who were older than 15 years of age and who had chronic symptomatic rupture of the ACL. A chronic rupture was defined as a delay between rupture and consultation with the senior author (ND) of more than six months. Patients with a history of previous surgery on the ACL, infection or septic arthritis in either knee and those with additional ligamentous instability in the affected knee were excluded. We obtained approval from the local Ethics Committee and informed written consent from all the patients. Randomisation to either a BPTB autograft or the LARS ligament was by opening a sealed envelope by an independent person on the day of surgery. There were 27 patients in the BPTP group and 26 in the THE JOURNAL OF BONE AND JOINT SURGERY
A NEW GENERATION OF ARTIFICIAL LIGAMENTS IN RECONSTRUCTION OF THE ANTERIOR CRUCIATE LIGAMENT
Table I. Details of the patients who underwent reconstruction of the ACL with either an ipsilateral BPTB autograft or the LARS artificial ligament Number of patients Mean (± SD) age in years Mean (± SD) injury age in years Gender Female Male
BPTB
LARS
27 30.87 ± 8.66 4.92 ±+ 6.03
26 31.03 ± 8.98 4.72 + 5.56
12 15
5 21
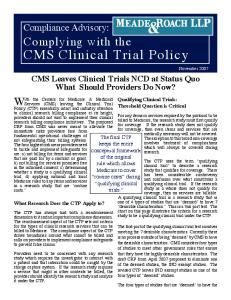
Fig. 1 The LARS ACL. The free fibres of the intra-articular portion are orientated clockwise or counterclockwise for right or left knees, to mimic the natural ligament.
LARS group with no significant differences with regard to age, gender and time from injury to surgery (Table I). The incidence of additional pathology was similar in both groups, with chondral changes present in 14 patients (52%) of the BPTB group and in 13 (50%) of the LARS group. Meniscal tears were seen in 22 patients (81%) of the BPTP and in 18 (69%) of the LARS group. Based on the experience with the Ligastic implant, a new design using Terresuisse-polyethylene terephtalate has been introduced which consists of two different parts. The intraosseous part is made of longitudinal fibres bound together by a transverse knitted structure. The intra-articular part comprises only longitudinal parallel fibres which are preVOL. 84-B, NO. 3, APRIL 2002
357
twisted at 90° (Fig. 1). This architecture is based on biomechanical studies which showed improved perform8,11 The intra-articuance compared with the earlier designs. lar multifilament part of the prosthesis is implanted in a twisted fashion to imitate the natural cruciate ligament. This avoids shearing forces between the fibres and interfibres during combined tension, torsion, and flexion. The polyethylene terephtalate fibres allow ingrowth of tissue in the intra-articular part. Ingrown soft tissue between the ligament fibres acts as a viscoelastic element and protects the ligament against friction at the opening of the bony canal as well as between the artificial fibres themselves. Operative technique. Routine arthroscopy was carried out on all patients and any minor meniscal injuries were treated. In those patients allotted to a BPTB autograft, a standard arthroscopically-assisted intra-articular ACL reconstruction was carried out using the middle one-third of the patellar tendon taken as an autograft as described by 12 Clancy. The LARS-ACL reconstructions were undertaken following the surgical principles which have previously 8,9,11 been described. We used the LARS 60 or 80 gauge fibres, depending on the weight of the patients. The diameter of the drill hole was 6 mm for the tibial and femoral tunnels in all patients. The artificial implant was fixed by interference-fit titanium screws with diameters of 7 and 8 mm at each site. The thread of the screws has blunt edges so that it will compress, but not cut, the material while locking the ligament securely. Rehabilitation. The postoperative rehabilitation protocol was identical for both groups. Patients followed a vigorous rehabilitation regime with weight-bearing as tolerated. They were discharged on the day after surgery and attended outpatient physiotherapy three times a week for three months. Evaluation. Preoperative assessments included measure13 ment of the Tegner score, clinical examination, instrumented laxity testing and MRI. The status of the injured knee was assessed using a modified International Knee 14 Documentation Committee (IKDC) scoring system, and assessment of patient satisfaction by the Knee Injury and 15 Osteoarthritis Outcome Score (KOOS). Standard followup evaluation at two, six, 12 and 24 months after surgery included a clinical examination, instrumented laxity testing (beginning after six months), and the evaluation of IKDC, Tegner score, and KOOS. Instrumented laxity testing (Telos, Marburg, Germany) was carried out at 20° of flexion with a maximal force mode of 250 N as the upper 16 limit. The uninjured limb was tested as a control. The surgeon was not involved in the follow-up, except in the case of any complication. The clinical assessment was undertaken by another physician (PL) and the KOOS was evaluated by a research assistant. Statistical analysis. All measurements are expressed as the mean and standard deviation, and non-continuous data as the median with ranges given. For statistical comparisons we used the chi-squared test for all categorical data, the
358
T. NAU, P. LAVOIE, N. DUVAL
Mann-Whitney U test to calculate the non-parametric data obtained from the KOOS questionnaires and Student’s ttest for unpaired groups for parametric data. A probability level of p < 0.05 was considered to be statistically significant.
Results IKDC evaluation. No significant differences were found between the groups with respect to any of the IKDC categories before operation. At the follow-up at six months, the patients in the LARS group showed a tendency (p = 0.051) towards better subjective assessment. Other areas of the IKDC evaluations showed no significant differences at that stage. At later stages of follow-up no significant differences were found between the two groups (Table II). Instrumented laxity testing. The anterior laxity values showed no significant differences between the two groups before operation. During the postoperative observation
Table II. The IKDC results for both groups before and at two, six, 12 and 24 months after operation IKDC score
Preop
Postop 2 6
12
24
Subjective (median) BPTB LARS
C C
C B
B B
B B
A A
Stability (median) BPTB LARS
C C
A B
B B
B B
B B
Range of movement (median) BPTB LARS
A A
B B
A A
A A
A A
Symptoms (median) BPTB LARS
D D
D D
C C
C C
A B
period, anterior laxity was significantly greater in the LARS group (p = 0.01) at the follow-up at six months. After 12 and 24 months, the laxity values were even greater in the LARS group, but the differences were not significant
100
100
50
50
0
0 Pre-op
2
6
12
24
Pre-op
2
6
12
24
Months after operation
Months after operation Fig. 2a
Fig. 2b
p=0.04 100
100
50
50
0
0 Pre-op
2
6
12
24
2
p=0.04
6
12
24
Months after operation
Months after operation Fig. 2c
100
Pre-op
p=0.04
Fig. 2d
p=0.03
p=0.02
6
12
50
0
Pre-op
2
Months after operation Fig. 2e
24
The mean KOOS scores for a) pain b) symptoms c) activities of daily living d) sports and recreation and e) quality of life for both groups before and at two, six, 12 and 24 months after operation (䡵 = LARS, 䡺 = BTB).
THE JOURNAL OF BONE AND JOINT SURGERY
A NEW GENERATION OF ARTIFICIAL LIGAMENTS IN RECONSTRUCTION OF THE ANTERIOR CRUCIATE LIGAMENT
(p = 0.31 and p = 0.18, respectively). At the most recent follow-up, the mean laxity testing was 2.38 ± 1.80 mm in the BPTB group and 4.86 ± 3.80 mm in the LARS group. KOOS evaluation and Tegner score. Before operation, there were no significant differences between the treatment groups in any of the subscales of KOOS. At follow-up at two months there were slightly better results in the LARS group with respect to the sports-and-recreation score (p = 0.058). At any stage of follow-up during the first year after operation, the LARS group showed better results for each of the KOOS subscales. Significant differences were found for the sports-and-recreation score (p = 0.04) and for the quality-of-life score (p = 0.03) at six months. At the follow-up at 12 months the activity-of-daily-living score (p = 0.04), the sports-and-recreation score (p = 0.04), and the quality-of-life score (p = 0.02) showed significant differences between the two groups. At follow-up at 24 months no significant differences were found in any of the subscales of KOOS (Fig. 2). Before operation and at any stage of follow-up, the median Tegner score showed no difference, except for the follow-up at two months when the median Tegner score was 4 in the LARS group and 3 in the BPTB group, showing a tendency towards a higher grade, although less than significant for the LARS group. Complications. There were no complications perioperatively in either treatment group. One BPTB patient developed an infected haematoma at the site of harvesting of the ipsilateral graft, requiring surgical debridement and antibiotics. Two patients were lost to follow-up, one in each group. Each was assumed to be a failure of reconstruction. One BPTB patient was suspected of being a failure at follow-up at 24 months, having marked laxity in both the clinical examination and instrumented laxity testing. One LARS patient had a further operation after laxity was recognised six months after operation. Arthroscopy showed an intact intra-articular ligament, but a loose femoral fixation. Through a 5 cm incision on the lateral aspect of the distal femur the old interference screw was removed and the intact ligament was retensioned and secured using an interference screw the diameter of which was 1 mm larger than that of the previous screw.
Discussion There are many reports of reconstruction of the ACL in the current literature. Most focus on the results of one particular technique. The paucity of prospective, randomised studies comparing different methods of reconstruction is 17,18 evident. Although short-term and intermediate observation periods for different types of reconstruction have been said to be too short to allow conclusions to be drawn in a prospective, randomised study, important differences can 17,18 be observed even within this short time. We have shown differences between the groups. In all five subscales of the KOOS, the patients with LARS reconVOL. 84-B, NO. 3, APRIL 2002
359
struction had better results during the first year after operation with significant differences in some categories. Also the patients’ subjective assessment of the IKDC showed a tendency to better results at follow-up at six months. Some authors have mentioned the importance of patient satisfac10,15,19 tion. Subjective outcome does not correlate with objective parameters such as instrumented laxity testing or 10,19 10 clinical examination. Lavoie et al have reported that documenting only the mechanical stability of the knee is inadequate in follow-up studies and a questionnaire assess19 ing patient satisfaction should be added. Hyder et al studied the correlation between instrumented laxity testing and functional outcome after reconstruction of the ACL. They did not find a significant correlation between the clinical outcome and objective arthrometric measurements. Some authors have mentioned the relationship between 20-22 proprioception and the subjective feeling of stability. 22 Fremerey et al reported that most of the proprioceptive recovery occurred between three and six months after reconstruction using the BPTB autograft, but not completely in the mid-range position. They concluded that an earlier return to full activity could be dangerous because of the proprioceptive deficit still present at this time. Although it was not the aim of our study to investigate proprioception, the LARS group had better results in terms of early return to sports and recreational activities. Compared with the BPTB group, the mean measured laxity was greater in the LARS group, and this difference was significant at six months. Except for one failure in each group, all patients had a firm endpoint to the Lachmann test at all stages of follow-up. Also, the stability assessment of the IKDC showed no differences between the two groups, suggesting that the passive stabilising function was intact, regardless of the reconstruction method. Artificial reconstruction of the ACL with the use of 23-29 Autovarious materials was recommended in the 1980s. genous grafts are thought to be weaker than artificial substances at implantation and undergo a period of morphological change with further weakening. On the other hand, artificial implants carry a risk of structural failure and reactive synovitis as a result of wear particles. Despite the possible advantages of a synthetic graft, such as minimal morbidity from the operation allowing an early return to unrestricted sports activity, the use of artificial ligaments in surgery on the ACL has not achieved universal popularity. 28 DiGiovine and Shields have described the common clinical history of an artificial ligament. This included excellent results during biomechanical testing followed by enthusiastic preliminary clinical results, then a period of overimplantation, complications and recognised clinical failures, and finally abandonment of the ligament and return to conventional autologous reconstruction techniques. The new generation of artificial ligaments, represented in our study by the LARS ligament, has already shown sat9-11 9 isfying results in retrospective studies. Dericks reported encouraging results in 220 cases of reconstruction of the
360
T. NAU, P. LAVOIE, N. DUVAL
ACL with a mean follow-up of 2.5 years. He mentioned that older artificial ligaments were extremely brittle and ruptured easily. The lack of resistance to abrasion had caused synovitis, predisposing to infection. The special design of the LARS ligament with open fibres in its intraarticular part is said to be more resistant to torsional fatigue and to wear and tear. In our series, we did not find any signs of clinically evident synovitis. That caused by wear particles has been reported to be a serious problem asso26,29 ciated with artificial ligaments. We conclude that reconstruction of the ACL using the LARS ligament in chronic ACL-deficient patients gives high patient satisfaction during the first 24 months after operation. The results thus far suggest that full return to activity may be achieved earlier compared with that following reconstruction using the BPTB autograft. This may offer the possibility of a shorter period of rehabilitation especially in the field of sports medicine. Long-term results from follow-up of this randomised controlled trial are essential, however, if the encouraging early results using the LARS ligament are to be maintained, thus reducing the current prejudice against the use of artificial ligaments in surgery on the knee. We thank Valerie Roy, MB and Anick Lambert, MSc, for their assistance in the administration of data. Although none of the authors have received or will receive benefits for personal or professional use from a commercial party related directly or indirectly to the subject of this article, benefits have been or will be received but are directed solely to a research fund, foundation, educational institution, or other non-profit institution with which one or more of the authors is associated.
References 1. Peterson RK, Shelton WR, Bomboy AL. Allograft versus autograft patellar tendon anterior cruciate ligament reconstruction: a 5-year follow-up. Arthroscopy 2001;17:9-13. 2. Eberhardt C, Kurth AH, Hailer N, Jager A. Revision ACL reconstruction using autogenous patellar tendon graft. Knee Surg Sports Traumatol Arthrosc 2000;8:290-5. 3. Deehan DJ, Salmon LJ, Webb VJ, Davies A, Pinczewski LA. Endoscopic reconstruction of the anterior cruciate ligament with an ipsilateral patellar tendon autograft: a prospective longitudinal fiveyear study. J Bone Joint Surg [Br] 2000;82-B:984-91. 4. Bonamo JJ, Krinick RM, Sporn AA. Rupture of the patellar ligament after use of its central third for anterior cruciate reconstruction: a report of two cases. J Bone Joint Surg [Am] 1984;66-A:12947. 5. Christen B, Jakob RP. Fractures associated with patellar ligament grafts in cruciate ligament surgery. J Bone Joint Surg [Br] 1992;74-B:617-9. 6. Hughston JC. Complications of anterior cruciate ligament surgery. Orthop Clin North Am 1985;16:237-40. 7. McCarroll JR. Fracture of the patella during a golf swing following reconstruction of the anterior cruciate ligament: a case report. Am J Sports Med 1983;11:26-7. 8. Cazenave A, Laboureau JP. Reconstruction of the anterior cruciate ligament: determination of the pre- and peroperative femoral isometric point. Rev Chir Orthop Reparatrice Appar Mot 1990;76:288-92.
9. Dericks G Jr. Ligament advanced reinforcement system anterior cruciate ligament reconstruction. Op Tech Sports Med 1995;3:187-205. 10. Lavoie P, Fletcher J, Duval N. Patient satisfaction needs as related to knee stability and objective findings after ACL reconstruction using the LARS artificial ligament. Knee 2000;7:157-63. 11. Laboureau JP, Marnat-Perrichet F. Isometric reconstruction of the anterior cruciate ligament: femoral and tibial tunnel placement. In: Yahia L'H, ed. Ligaments and ligamentoplasties. Berlin, etc, SpringerVerlag, 1997:209-25. 12. Clancy WG. Arthroscopic anterior cruciate ligament reconstruction with patellar tendon. Tech Orthop 1988;2:13-23. 13. Tegner Y, Lysholm J. Rating systems in the evaluation of knee ligament injuries. Clin Orthop 1985;198:43-9. 14. Hefti F, Muller W, Jakob RP, Staubli HU. Evaluation of knee ligament injuries with the IKDC form. Knee Surg Sports Traumatol Arthrosc 1993;1:226-34. 15. Roos EM, Roos HP, Lohmander LS, Ekdahl C, Beynnon BD. Knee injury and osteoarthritis outcome score (KOOS): development of a self-administered outcome measure. J Orthop Sports Phys Ther 1998;28:88-96. 16. Jardin C, Chantelot C, Migaud H, et al. Reliability of the KT-1000 arthrometer in measuring anterior laxity of the knee: comparative analysis with Telos of 48 reconstructions of the anterior cruciate ligament and intra- and interobserver reproducibility. Rev Chir Orthop Reparatrice Appar Mot 1999;85:698-707. 17. Engebretsen L, Benum P, Fasting O, Mølster A, Strand T. A prospective, randomized study of three surgical techniques for treatment of acute ruptures of the anterior cruciate ligament. Am J Sports Med 1990;18:585-90. 18. Engstrom B, Wredmark T, Westblad P. Patellar tendon or LeedsKeio graft in the surgical treatment of anterior cruciate ligament ruptures: intermediate results. Clin Orthop 1993;295:190-7. 19. Hyder N, Bollen SR, Sefton G, Swann AC. Correlation between arthrometric evaluation of knees using KT 1000 and Telos stress radiography and functional outcome following ACL reconstruction. The Knee 1997;4:121-7. 20. MacDonald PB, Hedden D, Pacin O, Sutherland K. Proprioception in anterior cruciate ligament-deficient and reconstructed knees. Am J Sports Med 1996;24:774-8. 21. Barrett DS. Proprioception and function after anterior cruciate reconstruction. J Bone Joint Surg [Br] 1991;73-B:833-7. 22. Fremerey RW, Lobbenhoffer P, Zeichen J, et al. Proprioception after rehabilitation and reconstruction in knees with deficiency of the anterior cruciate ligament: a prospective, longitudinal study. J Bone Joint Surg [Br] 2000;82-B:801-6. 23. Bolton CW, Bruchman WC. The GORE-TEX™ expanded polytetrafluoroethylene prosthetic ligament: an in vitro and in vivo evaluation. Clin Orthop 1985;196:202-13. 24. Fujikawa K. Clinical study of anterior cruciate ligament reconstruction with the Leeds-Keio artificial ligament. In: Friedman MJ, Ferkel RD, eds. Prosthetic ligament reconstruction of the knee. Philadelphia, etc: WB Saunders Company, 1988:132-9. 25. Gillquist J. Important factors in the use of the Dacron ligament. Acta Orthop Belg 1987;53:353-5. 26. Gillquist J, Odensten M. Reconstruction of old anterior cruciate ligament tears with a Dacron prosthesis: a prospective study. Am J Sports Med 1993;21:358-66. 27. Park JP, Grana WA, Chitwood JS. A high-strength Dacron augmentation for cruciate ligament reconstruction: a two-year canine study. Clin Orthop 1985;196:175-85. 28. DiGiovine NM, Shields CL. Synthetic ligaments in ACL reconstruction: a review. Am J Knee Surg 1991;4:42-8. 29. Lukianov AV, Richmond JC, Barrett GR, Gillquist J. A multicenter study on the results of anterior cruciate ligament reconstruction using a DACRON ligament prosthesis in ‘salvage’ cases. Am J Sports Med 1989;17:380-6.
THE JOURNAL OF BONE AND JOINT SURGERY