Review article
c
...........................................................................................................................................................
The management of clinical risk in telemedicine applications Adam Darkins Riverside Community Health Care NHS Trust, London, UK
Summary Any telemedicine application should be viewed in terms of its health-care context, the clinical process it is enabling, and whether it is appropriate to apply telemedicine to that process. Telemedicine should be used as a tool to enable the transfer of clinical information which, by being transferred, will reduce clinical risks. Because managing clinical services involves knowing where clinical decisions are being made, it is important to ensure that telemedicine activity is recorded as part of the routine clinical and investigative data sets that will be kept for clinical audit and health-service costing purposes. There may be areas of health-care delivery where the telemedicine solution becomes the treatment of choice. In this event, not to provide telemedicine may be unethical and may expose a service to high clinical risk. If a service is based on the use of telemedicine, it is important to ensure that the technical specifications are adequate, that the system is sufficiently reliable, and that there are adequate back-up provisions in the case of system failure.
Introduction
................................................................................. It is a reflection of the way that telemedicine applications are moving into the mainstream of health-care delivery that clinical risk management is now an important determinant of the future development of telemedicine generally. Health-care developments normally evolve from a research setting and in their early stages act as an adjunct to existing care. Developments such as telemedicine usually receive insurance cover from the academic institutions that sponsor them. When such developments are ready for incorporation into mainstream operational services, they must be demonstrably reliable, robust and safe, thereby ensuring that the revenue streams from public and/or private health purchasers can be generated to sustain them. This paper reviews the clinical risk-management aspects of telemedicine that will determine its widespread adoption, and suggests issues that clinicians and managers should consider in setting up telemedicine services. Telemedicine can be defined simply as ‘medicine carried out at a distance’1. This pragmatic definition Accepted 15 September 1996 Correspondence: Dr A Darkins, Medical Director, Riverside Community Health Care NHS Trust, Parsons Green Health Centre, 5–7 Parsons Green, London SW6 4UL, UK (Fax: +44 181 846 7654)
Journal of Telemedicine and Telecare 1996; 2: 179–184
offers practitioners, managers, and others with an interest in telemedicine a useful working basis upon which to consider any clinical risks that are associated with new or existing applications. It follows from this definition that telemedicine represents a process that facilitates health-care activity taking place, and therefore does not act as an end in itself. Meaningful assessment of what clinical risks are associated with a telemedicine application should therefore always begin by answering the following question: what clinical process, or processes, is telemedicine enabling, or seeking to enable? A subsidiary question that follows from this is: is it appropriate to apply telemedicine to facilitate the clinical process or processes?
Clinical guidance point Any telemedicine application should be viewed in terms of its health-care context, the clinical process it is enabling, and whether it is appropriate to apply telemedicine to that process.
Telemedicine and the clinical process
................................................................................. When it is viewed in these terms, telemedicine is patently not a new concept. It is well accepted in routine health-care practice for clinician–clinician and
A Darkins Managing clinical risk in telemedicine
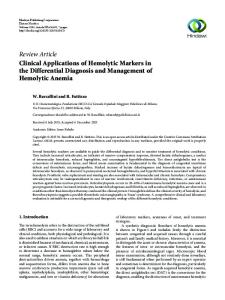
clinician–patient contact to take place via the telephone, as has been the case throughout this century2. This is a formof telemedicine, although many clinicians who unhesitatingly use a telephone to mediate an exchange of clinical data with a colleague, or patient, would not necessarily recognize it as such. Yet health-care workers often express reservations about telemedicine, suggesting that it exposes clinicians and patients to ‘risk’. Are fears that there are attendant clinical risks justified in the case of telemedicine? A useful starting point is to consider the millions of telephone consultations worldwide each year that enable practitioners to exchange clinical information and ratify clinical decisions. A hypothetical case illustrating the risks that may accompany a ‘routine’ telephone consultation is suggested by the following example: A young woman with multiple injuries, including a suspected serious head injury, is taken by ambulance to the accident and emergency department of a hospital without neurosurgical facilities on site. The clinical dilemma for the doctors attending the patient is whether she needs urgent transfer to a neurosurgical facility for her head injury. This decision is not straightforward because transferring the patient many miles in an ambulance may mean that she will deteriorate from another, as yet unrecognized, injury, apart from her known head injury, or from the head injury itself. In transit she will not have access to the investigative and/or resuscitation back-up immediately available in an acute hospital. Given that there are therefore risks associated with both transfer and non-transfer, a telephone consultation allows the clinical history, the physical examination, and the results from any investigation to be relayed to staff at the neurosurgical facility. From this assortment of verbal data a decision can be made about whether or not transfer of the patient should be undertaken. This hypothetical example is in fact ‘accepted practice’. Is it appropriate to upgrade from telephone to video consultation and teleradiology, or will upgrading the technology in this way increase the clinical risk? Video consulting will allow the neurosurgical clinicians, who have expertise in assessing head-injured patients, to assess the level of the patient’s coma remotely. Teleradiology means that skull radiographs and computerized tomography (CT) scans can be viewed by the neurosurgical expert (Fig 1). Consequently, the quality of decision support to the referring clinician will be increased. In this hypothetical case these data are required to make a judgement about whether a blood clot is compressing the patient’s brain, and whether immediate surgery to release the pressure from this clot
180
Fig 1 Extradural haematoma. A verbal description of a computerized tomography scan given by telephone is likely to be much riskier clinically than the transmission of the scan itself by teleradiology. (Courtesy Dr C McKinstry, Royal Victoria Hospital, Belfast, UK.)
is required. In addition to the diagnostic support, a video link enables remote surgery to be supervised if it has to be undertaken as an urgent life-saving procedure because transfer to a neurosurgical facility will take too long. In the hypothetical example above the use of telemedicine is not only appropriate but also reduces the risk to the patient. When the remote clinical assessment of patients using telemedicine is appropriate, it may serve to reduce the clinical risk, in comparison with traditional, non-telemedicine situations. Although the hypothetical case is an extreme example, it illustrates the principles that apply to telemedicine in general.
Clinical guidance point The appropriate use of telemedicine should be as a tool to enable the transfer of clinical information which, by being transferred, will reduce the clinical risks.
Telemedicine as ‘accepted practice’
................................................................................. An important component of any defence raised by hospitals and clinicians against litigation for Journal of Telemedicine and Telecare Volume 2 Number 4 1996
A Darkins Managing clinical risk in telemedicine
malpractice is whether or not the practice being questioned accorded with what a responsible body of medical opinion would consider ‘accepted practice’3. Clinical risk management is a proactive process designed to reduce the threat of litigation. It is therefore important that health-care providers implementing telemedicine services adopt clinical standards for telemedicine that are agreed by practitioners. Realtime videoconferencing is the technology that enables teleconsulting, and our current development of teleradiology applications is now possible because of reductions in hardware costs, and the availability of cheap, reliable digital data transmission networks. The capture and transmission of these digital data at affordable costs are fundamental factors that are driving telemedicine services into ‘accepted practice’. Early telemedicine systems were reliant upon standard videoconferencing equipment to capture realtime video. Increasingly telemedicine systems are now using desktop PCs with videocards and camera attachments, in place of boardroom-style videoconferencing equipment. An advantage of this switch in technology is that details of the clinical consultation can be exchanged, stored and then kept as a permanent record. Accurate record keeping of telemedicine activity is an important part of managing the clinical risk associated with it. However, a potential drawback of the increasing sophistication of PCs is that as videoconferencing facilities become ubiquitous, teleconsultations may develop ad hoc, in the manner of an extension of the current use of the telephone, in which event there will be risks. These risks are associated with the delegation of decision making that telemedicine allows without the ability to make a full clinical examination. This is why protocols are important to ensure that telemedicine is used safely. It is the current marketing strategy of some equipment providers that they will sell the ‘boxes’ rather than develop the processes that support the safe development of telemedicine. Equipment suppliers should at the very least be aware of the standards for equipment such as resolution of cameras and of monitors, data transfer speeds, and so on that are necessary to meet the demands of the clinical situation that their product is supporting.
Professional ‘acceptance’ of telemedicine
................................................................................. As with any innovation, there is often initial resistance on the part of some clinicians to embrace telemedicine in their routine clinical practice. This resistance is associated with a perception that a teleconsultation is somehow aesthetically not as good as a face-to-face consultation. The face-to-face consultation is undoubtedly the ‘gold standard’ where a patient and a clinician who has the appropriate clinical skills to deal with a problem are able to meet easily. However, the logistics of placing the patient with the appropriate clinician can be difficult to arrange because of geographical distance, time, cost or lack of relevant expertise locally. In such instances telemedicine offers the potential for a general practitioner who is managing a patient to access specialist skills, or for a specialist clinician to access advice from another specialist clinician. Circumstances are foreseeable where teleconsultation becomes the treatment of choice; if telemedicine is not used in such circumstances, a health-care provider could be exposed to the risk litigation. Once telemedicine applications are devised and piloted this process of substitution may occur very quickly, particularly when the inevitable growth in the availability of videoconferencing facilities takes place.
Clinical guidance point There may be areas of health-care delivery where the telemedicine solution becomes the treatment of choice. In this event, not to provide telemedicine may be unethical and may expose a service to high levels of clinical risk.
Telemedicine and ‘technical safety’
.................................................................................
Because managing clinical services involves knowing where clinical decisions are being made, it is important to ensure that telemedicine activity is recorded as part of the routine clinical and investigative data sets that will be kept for clinical audit and health-service costing purposes.
As a consequence of a growth in the use of telemedicine and it becoming a vital component of clinical services, the robustness and reliability of the equipment assumes an important dimension in the clinical risk equation. Telemedicine applications are attractive to health-care providers as a way of saving costs. Health services must meet the continual need to become more efficient in dealing with ever-growing demands resulting from the increased expectation of patients and demographic changes. If these savings and increased efficiencies are to be realized, then telemedicine must not duplicate existing services, but should substitute for existing ways of delivering health care. The technical failure of equipment, whether hardware, software or the underlying telecommunication network, may interrupt vital
Journal of Telemedicine and Telecare Volume 2 Number 4 1996
181
Clinical guidance point
A Darkins Managing clinical risk in telemedicine
clinical processes and consequently put patients at risk of injury or death. Minimizing these risks involves setting agreed standards for the technical infrastructure upon which telemedicine applications are based. Technical and clinical back-up mechanisms need to be created to support care in areas where risk of failure is assessed as unacceptably high.
Clinical guidance point If a service is based on the use of telemedicine, it is important to ensure that the technical specifications are adequate, that the system is sufficiently reliable, and that there are adequate back-up provisions in the case of system failure.
Introducing telemedicine into routine service: managing the process or muddling through? .................................................................................
Currently telemedicine is at a stage in its evolution that offers two approaches to its future growth and dissemination. The first is that telemedicine is introduced by individual clinicians who are enthusiasts and that it becomes a ubiquitous process like the use of the telephone. The second is that it is a managed process. Although enthusiastic clinicians are vital, an unmanaged approach to the introduction of telemedicine may leave unresolved vital concerns about clinical risk and reimbursement for services provided. The prudent health-care organization will therefore consider telemedicine as a managed process and not an exercise in serendipity. If the widespread dissemination of telemedicine services is to be managed in health-care institutions, what are the issues?
Questions for directors, managers and clinicians What does this review of telemedicine mean practically for the busy clinician, clinical risk manager, medical director or general manager at work in a health-care organization? Below are some questions that they might consider.
Informal telemedicine activity Currently the clinicians in an organization who may range from chiropodists to cardiac surgeons will be teleconsulting by telephone. Few, if any, will have received training in conducting a remote consultation. These clinicians will assume that the process works well unless they have been involved in a clinical complaint,
182
clinical incident, or litigation that involved a telephone consultation as part of the clinical process. Many health-care organizations are concentrating upon the telephone manner of their staff as a priority in their ‘customer care strategy’ for patient-focused services. This effort usually targets reception staff as an important part of quality initiatives associated with complaints handling and clinical risk management. Is the organization aware of the quantity and quality of informal telemedicine activity that it undertakes? Should the organization conduct an audit/risk analysis of this aspect of care, looking at, for example, telephone contacts between family doctors and junior hospital doctors?
Formal telemedicine activity Does the organization participate in formal telemedicine activity? If the answer to this is yes, has this been subject to a formal clinical risk analysis, and has suitable indemnity cover been arranged? Does the organization have a strategy for the development of telemedicine services? Is the organization developing clinical guidelines, clinical protocols and clinical care pathways? If the answer to this is yes, is telemedicine activity incorporated into these processes? Is there training for clinicians in their use and is such training regularly audited?
Clinicians in telemedicine Are clinicians in the organization aware of the differences between a face-to-face consultation, a telemedicine consultation and a telephone consultation? Are clinicians clear about what each of these means in terms of their clinical responsibility for the patient? Are clinicians satisfied with protocols for telemedicine consultations, and satisfied that these ensure that consultations take place with clinicians who have adequate training for the particular areas of referral made to them? Are there adequate systems in place for notes to be made and records kept of telemedicine consultations? Have they a clinical need, and permission from the patient, to record a consultation on video, if appropriate? Is the picture quality sufficient for the telemedicine consultations that take place? Is the telemedicine part of the service a vital component, one that ensures the integrity of a pathway of clinical care? If the answer to this is yes, are there adequate back-up procedures in place if the primary telemedicine system fails? If the answer to this is yes, have these procedures been tested? Journal of Telemedicine and Telecare Volume 2 Number 4 1996
A Darkins Managing clinical risk in telemedicine
Departments of information technology and telemedicine Is the information technology department aware of telemedicine activity that is taking place? Do telemedicine services use a secure and reliable network? What is the failure rate for the technology that is being used? Are there operative log-on procedures, protected by secure passwords, to ensure the security of consultations and prevent impersonation?
Legal representatives/clinical indemnity providers Are they aware that the organization is undertaking, or thinking of undertaking, telemedicine? What aspects of telemedicine do they provide cover for, and what areas do they not cover? Are there any standards that they would wish to see in place for telemedicine services provided?
The way forward
.................................................................................
Effective protocol That there is a need to question the standards of care, protocols and the suitability of applications for telemedicine reflects a current uncertainty about the place of telemedicine in clinical care. It is also illustrative of the fact that new health-care interventions are subject to much greater scrutiny than in the past. Although there is a move towards evidence-based medicine, applying telemedicine to established areas of practice raises the problem that many of these are not themselves based upon sound evidence of effectiveness4. In developing telemedicine services it therefore makes sense from both a quality-of-care and an economic perspective, as well as a sound clinical risk management strategy, to base these services on effectiveness-based protocols that provide clear standards to audit.
the ultimate wellbeing of their patients, irrespective of the systems they use to deliver care. It is therefore important that health-care organizations involve clinicians and risk managers in exploring the implications of telemedicine activities as they establish new services. Legal review of the implications of telemedicine3 suggests that there are no new issues of principle outside the current duty of care if health-care services are transferred to telemedicine from face-to-face consultation.
Technology and telemedicine The barriers to the safe expansion of telemedicine services are non-technical. The basic technology is robust, reducing in price, and increasing in performance. The barriers to telemedicine are ‘people issues’. They are organizational, and there is little point in introducing technology into health care if it does not fit the clinical situation to which it is being applied. Telemedicine offers potentially lucrative avenues for the international export of medical expertise, as never before. Health-care organizations adopting, buying, or selling telemedicine services must ensure there is reciprocity of recognition of professional qualifications for clinical staff within and between countries. While this review has concentrated upon the clinical rather than the hardware aspects of telemedicine, it is important to ensure the compatibility of equipment. Computers as well as people must be able to talk to each other. A final process to consider is the place of third parties, such as the network carriers. The network chosen is of great importance in terms of the security and reliability of the telemedicine transaction. An open system such as the Internet should be considered a high-risk option in this context because it is not secure. Paradoxically, however, many of the data upon which the effectiveness of telemedicine will be judged in future may well be transmitted over the Internet.
Medicolegal considerations
Conclusions
Although telemedicine is as yet largely unproven, so also are many health-care interventions5. Telemedicine must further establish itself by developing the appropriate protocols for its widespread use. The medicolegal implications of telemedicine are currently unclear, and are currently based upon conjecture because there is no clear body of legal judgement upon which to determine precedent3. Clinicians, and the health-care organizations in which they work, have a duty of care to the patients they look after, and have a responsibility, therefore, for
Telemedicine is an exciting and dynamic technique that is likely to play a major role in the way in which health care is delivered in the future. It offers the promise of putting the patient at the very centre of health-care delivery. Although there are risks associated with its widespread introduction these should be viewed in their proper perspective and managed in the context of a riskmanagement approach, not evoked as a spectre to haunt and inhibit the growth and reputation of telemedicine.
Journal of Telemedicine and Telecare Volume 2 Number 4 1996
.................................................................................
183
A Darkins Managing clinical risk in telemedicine
Acknowledgement: This article is based, with permission, on one published previously in Health Care Risk Report.
References 1 Editorial. Telemedicine: fad or future? Lancet 1995;345:73–4 2 Hallam L. You’ve got a lot to answer for, Mr Bell: a review
184
of the telephone in primary care. Family Practitioner 1989;6: 45–57 3 Brahams D. The medicolegal implications of teleconsulting in the UK. Journal of Telemedicine and Telecare 1995;1:196–201 4 Hoare J. Tidal Wave: New Technology, Medicine and the NHS. London: King’s Fund Centre, 1992 5 Department of Health. Assessing the Effectiveness of Health Technology. Principles, Practice, Proposals. Report of the Advisory Group of Health Technology Assessment. London: Department of Health, 1993
Journal of Telemedicine and Telecare Volume 2 Number 4 1996