Vol. 31, No. 9
JOURNAL OF CLINICAL MICROBIOLOGY, Sept. 1993, p. 2281-2285
0095-1137/93/092281-05$02.00/0 Copyright X 1993, American Society for Microbiology
Phenotypical and Genotypical Characterization of Epidemic Clumping Factor-Negative, Oxacillin-Resistant Staphylococcus aureus ANDREAS SCHWARZKOPF,1* HELGE KARCH,1 HERBERT SCHMIDT,' WOLFGANG LENZ,2 AND JURGEN HEESEMANN'
Institut fuir Hygiene und Mikrobiologie der Universitat Wiurzburg, Josef-Schneider-Strasse 2, D H97080 Wurzburg, 1 and Nationales Referenzlabor fiir die Staphylokokken-Lysotypie, Institut fur Medizinische Mikrobiologie und Immunologie der Universitat Bonn, Venusberg, D H53105 Bonn 1,2 Gennany Received 8 March 1993/Returned for modification 30 April 1993/Accepted 22 May 1993
A total of 50 oxacillin-resistant Staphylococcus aureus (ORSA) strains that were clumping factor negative (CFN) and protein A negative by latex agglutination were collected from patients in six different hospitals at different locations in Germany during 199l and 1992. Antibiograms, bacteriophage typing, and plasmid analysis were performed. The antibiograms showed that, besides oxacillin, all CFN ORSA strains were resistant to gentamicin, clindamycin, erythromycin, ciprofloxacin, and fosfomycin. All these isolates were nontypeable with an international set of phages, and an additional experimental phage set indicated that the strains were phage type 16, 192. Moreover, all isolates possessed a single plasmid of 30 kb, and restriction analysis of those plasmids revealed identical patterns. For genotyping, these 50 isolates were also analyzed by pulsed-field gel electrophoresis (PFGE) and polymerase chain reaction (PCR) of the coagulase and protein A genes and then by restriction enzyme digestion and analysis of restriction fragment length polymorphisms (RFLPs). With 49 strains, electrophoresis of SmaI-digested chromosomal DNA revealed identical PFGE patterns regarding the number and size of the DNA fragments, which could be differentiated from those of clumping factor-positive ORSA strains. Typing for the coagulase gene by PCR revealed PCR products of identical sizes. The AluI restriction digestion patterns of the PCR products were identical. PCR with primers derived from the region of that part of the protein A gene that encodes the immunoglobulin G-binding domains showed a PCR product that was about 170 bp smaller than that of the protein A gene from strains that were positive in the protein A latex agglutination test. Since it is precisely this size that is required in order to encode one immunoglobulin G-binding region, we assume that this is not present in the CFN ORSA strains. The phenotypical and genotypical features identify these very unusual CFN ORSA strains as being of clonal origin. Oxacillin-resistant Staphylococcus aureus (ORSA) strains becoming increasingly problematic in hospitals throughout the world (21). Serious infections caused by ORSA strains include wound infections, pneumonia, and septicemia. Patients with the highest risk are the elderly, patients with bums, those in intensive care units, and patients with surgical wounds or venous access sites (3, 4). The nares of staff members are occasionally colonized by these strains and contribute to the spread of staphylococci (2, 3, 16). In intensive care units, an increasing number of ORSA strains that are also resistant to erythromycin, aminoglycosides, and clindamycin are found (4). Identical susceptibility patterns among ORSA strains may initially indicate nosocomial transmission. In the last few years there has been a clear-cut trend toward genotyping based on chromosomal analysis by pulsed-field gel electrophoresis (PFGE) (9, 17, 20) and variable genetic elements; one example of molecular typing of variable genes within S. aureus is the work of Goh et al. (7), which was based on coagulase gene polymorphisms. The reasons behind this trend have to do with the fact that the genetic basis of the phenotypic variability is usually unknown. Control relies upon rapid identification of these organisms as well as immediate effective infection control programs. A rapid laboratory method commonly used to identify S.
is the clumping factor and protein A detection performed with latex particles coated with fibrinogen or immunoglobulin G (IgG). Unusual strains of ORSA which were nonreactive in the two latex agglutination assays have recently been reported in North America (20), the British Isles (13), and Germany (18). After isolating clumping factornegative (CFN) ORSA from a hospital outbreak (18), we learned of five other hospitals in Germany which had also recovered such unusual outbreak-associated CFN ORSA strains. Here we describe the characterization of 50 isolates by phenotypical and genotypical typing procedures. We provide evidence that the CFN ORSA strains gathered from different hospitals at different locations in Germany are clearly of clonal descent. aureus
are
*
MATERIALS AND METHODS
Bacterial strains. All CFN ORSA strains were isolated between November 1991 and June 1992 from various clinical materials (wound swabs [n-31 isolates], tracheal secretions [n-12], blood cultures [n-4], urine [n-2], postmortem swab from ethmoidal cells [n-1]). The isolates that we examined originated from six different hospitals (hospitals A to F) from different locations scattered throughout Germany. Six clumping factor-positive (CFP) ORSA strains and six Staphylococcus epidermidis isolates were used as control strains in the genotyping experiments. We are not aware of contacts
Corresponding author. 2281
2282
SCHWARZKOPF ET AL.
between patients and medical staff from hospital A and the other clinics. Biotyping and antibiotic susceptibility testing. The clumping factor was tested with Staphyslide (Bio Merieux, Charbonnieres-lesbains, France), and protein A was tested with Staphaurex D (Wellcome Diagnostics, Dartford, Great Britain). Biochemical identification was carried out with the API system (Bio Merieux). Plasma coagulase activity was tested with fresh rabbit plasma (overnight colony suspended in 0.5 ml of 1:10-diluted plasma incubated at 37°C for 2 h). DNase was determined by an agar plate test (Difco Laboratories, Detroit, Mich.). Antibiotic susceptibilities were determined by the agar disk diffusion test (German standard specification); oxacillin resistance was determined on agar plates containing 6 mg of oxacillin per liter and 4% NaCl incubated at 30°C for 48 h. Phage typing. An international basic set of 23 phages (group I, 29, 52, 52A, 79, and 80; group II, 3A, 3C, 55, and 71; group III, 6, 42E, 47, 53, 54, 75, 77, 83A, 84, and 85; group V, 94 and 96; and miscellaneous, 81 and 95) was deployed by standard methods. Because routine test dilutions x 100 did not provide a lysotype, additional phages (Dll, 16, 92, 187, 192) were used. Phages that produced a strong reaction, as defined in international rules (8), gave the lysotype. Plasmid preparation and analysis. Plasmid DNA was prepared as described by Birnboim (1), with slight modifications. Briefly, 1.5 ml of an overnight culture was pelleted by centrifugation. The cells were resuspended in 0.1 ml of STE buffer (50 mM disodium EDTA, 50 mM Tris-HCl, 8% saccharose), and 0.5 mg of lysostaphin (Sigma Chemical Co., St. Louis, Mo.) per ml was added. The cells were lysed (at 37°C for 8 min), and the suspension was mixed with 0.3 ml of solution II (0.2 N NaOH, 1% [wt/vol] sodium dodecyl sulfate; Serva, Heidelberg, Germany) and was kept on ice for 5 min. Subsequently, 0.225 ml of solution III (60 ml of 5 M potassium acetate, 11.5 ml of glacial acetic acid, 28.5 ml of distilled water) was added; the suspension was placed on ice for another 5 min. After 10 min of centrifugation, DNA was extracted with phenol-chloroform (1:1) and centrifuged, and the DNA in the supernatant was precipitated with 96% ethanol. The DNA was then washed with 70% ethanol and dried in an exsiccator. The resulting pellet was resuspended in 0.05 ml of distilled water and was digested with 1 ,ul of RNase (100 ,ug/ml) at 37°C for 15 min. Restriction analysis was performed with EcoRI as recommended by the manufacturers. Electrophoresis was carried out in a 0.6% agarose gel that was stained with ethidium bromide. PFGE. PFGE was done by a procedure slightly modified from that of Goering and Duensing (6). Logarithmically grown cells were harvested from 10-ml bouillon cultures (brain heart infusion with 1% glycine), and the pellet was then washed twice with TEN buffer (0.1 M Tris [pH 7.5], 0.1 M EDTA, 0.15 M NaCl). Subsequently, the bacteria were resuspended in EC buffer (6 mM Tris-HCl [pH 7.6], 1 M NaCl, 0.1 M EDTA [pH 7.5], 1% sodium lauroyl sarcosine, 0.2% deoxycholate). This solution was mixed with 2% GTG-agarose (Biometra, Gottingen, Germany) and cast in blocks, which were incubated overnight at 37°C in 0.5 ml of EC buffer containing 30 to 45 U of lysostaphin per ml and 10 mg of lysozyme (Sigma) per ml. On the next day, the EC buffer was replaced with 0.5 ml of ESP buffer (0.5 M EDTA [pH 9.3], 1% sodium dodecyl sulfate, 1 mg of proteinase K [Merck, Darmstadt, Germany] per ml), and the blocks were incubated at 55°C for 48 h. They were incubated with the TE buffer (10 mM Tris-HCI, 5 mM EDTA [pH 7.5]), which was
J. CLIN. MICROBIOL.
changed twice within 4 h, and were stored until use. The blocks were digested with SmaI (20 U in 0.150 ml of NE buffer 4; New England BioLabs, Beverly, Mass.) at 25°C for 24 h. Slices of the digested blocks were loaded onto the wells of a 1% agarose gel. Lambda concatemers (lambda ladder; New England BioLabs) were used as size markers. PFGE was performed on the CHEF-DR II system (Bio-Rad, Munich, Germany) with initial pulse times of 5 s and a pulse time of 50 s at the end of the 26-h run at a constant voltage of 200 V. Gels were stained with ethidium bromide and viewed under UV light. PCR amplification for detection of protein A and coagulase genes. Bacterial cell lysis was performed as described by Goh et al. (7), with minor modifications. Briefly, each isolate was subcultured overnight in 5 ml of Trypticase soy broth. The cells were centrifuged (1,000 x g) and washed in 50 mM Tris-HCl buffer (pH 7.5) containing 50 mM disodium EDTA (TE). The cell pellet was suspended in 500 p,l of TE containing 15 U of lysostaphin (Sigma) per ml and was incubated at 37°C for 1 h. To this was added 1 ml of lysing buffer (composed of 0.45% Triton X-100, 0.45% Tween 20, and 0.6 p,g of proteinase K [Sigma] per ml in polymerase chain reaction [PCR] buffer [Amersham Laboratories, Buckinghamshire, United Kingdom]). The samples were incubated for an additional 1 h at 56°C and were finally extracted with phenol-chloroform (1:1). PCR was used for the detection of the S. aureus protein A gene (spa). Primers spa-1 (5'-CAA AGA TCA ACA AAG CGC C-3') and spa-2 (5'-CGA AGG ATC GTC TIT AAG GC-3') were designed for amplifying a 622-bp fragment of the spa gene, which encodes a domain essential for binding IgG. PCR was performed by adding 5 ,ul of each lysate described above to the mixture containing 50 pmol of each primer, 5 ,ul of 10-fold polymerase synthesis buffer, 200 p,M (each) deoxynucleoside triphosphate, and 2.5 U of Taq polymerase (Amersham Laboratories) in a total volume of 50 ,ul of deionized water. The samples were subjected to 30 PCR cycles, each of which consisted of 40 s at 94°C, 90 s at 54°C, and 90 s at 72°C. The nucleotide sequences of primers COAG2 and COAG3 were the same as those described by Goh et al. (7). The conditions for amplifying the coagulase gene were modified slightly, in that the cells were lysed as described above. Five milliliters of cell lysate was subjected to 30 PCR cycles. Restriction analysis of the PCR products. Restriction analysis of the spa PCR products was performed with Hinfl (Pharmacia LKB). AluI (New England BioLabs) was used for restriction analysis of the coagulase PCR products.
RESULTS Biotyping of CFN ORSA. When subjected to agglutination tests, all epidemic ORSA strains proved to be negative for both the clumping factor and protein A. The reaction for DNase was positive. Rabbit plasma was coagulated by these isolates within 2 h. Biochemical analysis of the isolates with the API system resulted in the definitive identification (99.9%) of S. aureus. Antibiotic susceptibility testing. All CFN S. aureus strains were resistant to oxacillin (and, therefore, to all other -lactam antibiotics and imipenem), gentamicin, clindamycin, erythromycin, ciprofloxacin, and fosfomycin. Susceptibilities to tetracycline, vancomycin, rifampin, and fusidic acid and, with a single exception, to co-trimoxazole were found. Phage typing. None of 50 CFN ORSA strains could be
-~ ~1,6
CHARACTERIZATION OF OXACILLIN-RESISTANT S. AUREUS
VOL. 31, 1993 M 1 2
3 4
5 6 7 8 9 10 11 12
M l
kb
38 -
582
533,5
389,5
-
388
339,5 291
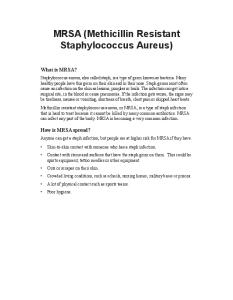
194 FIG. 1. PFGE analysis of the ORSA strains. Lanes 1 to 11, CFN outbreak strains from hospital A; lane 12, the SmaI pattern of a CFP ORSA strain from the same hospital.
typed with an international basic set of 23 phages. By using additional phages, the ORSA strains were shown to belong to lysotype 16, 192. PFGE analysis. Genomic analysis of SmaI-digested chromosomal DNA separated by PFGE was deployed in order to show the interrelationships between the CFN ORSA strains. The genome type was defined as any fragment pattern varying from another with regard to the number and sizes of the particular fragment bands concerned. First, we analyzed the outbreak strains from hospital A. Their patterns are depicted in Fig. 1, lanes 1 to 11. They were identical with regard to their numbers and sizes. Lane 12 in Fig. 1 shows the pattern of a representative CFP ORSA strain stemming from the same hospital. This isolate revealed a different PFGE pattern, as did five other CFP ORSA strains (data not shown). In the next stage we compared the CFN ORSA strains from hospital A with the CFN ORSA strains from hospitals B, C, D, E, and F. Figure 2, lanes 1 to 6, shows the directly comparable PFGE patterns. With the exception of the pattern shown in Fig. 2, lane 6, which stemmed from the only strain that had a slightly modified antibiogram (cotrimoxazole resistant), identical patterns were observed. Because the differences here were minimal, we suggest that such a strain be classified as a genomic subtype. Plasmid analysis. All 50 of the CFN ORSA stains were tested for the presence of plasmids. This revealed that they uniformly harbored a single plasmid of 30 kb in size. Restriction analysis was carried out on these plasmids. As an example, four representative CFN ORSA strains digested with EcoRI are depicted in Fig. 3, lanes 5 to 8, and strains digested with BamHI are shown in Fig. 3, lanes 10 to 13. It is apparent that the numbers and sizes of the restriction fragments were identical for each strain, but were different from those for the CFP ORSA strain shown in lane 9 of Fig. 3. Amplification and restriction analysis of the coagulase gene of CFN ORSA. A novel typing method for S. aureus that is based on PCR amplification of the variable region of the coagulase gene and then AluI restriction enzyme digestion (7) was used in the present study. All 50 CFN ORSA strains from the various hospitals showed a single PCR product of approximately 650 bp. Six isolates of coagulase-positive ORSA strains revealed different patterns and patterns that were different from those of the CFN strains. These patterns differed by the numbers and sizes of the individual PCR
2
3
4
7. .
kb
145,5 -
97
--
48,5
-
5
6
2283
I
FIG. 2. Directly comparable PFGE patterns of CFN ORSA strains from different hospitals. Lanes 1 to 6, strains from hospitals A, B, C, D, E, and F, respectively; lane M, lambda concatemers ranging from 48.5 kb (bottom) to 582 kb (top) used as DNA size markers.
products. One example is shown in Fig. 4, lane 1, in which two PCR products of 800 and 410 bp are shown. AluI restriction enzyme digestion of the PCR products generated fragments of identical sizes for the CFN strains (Fig. 4, lanes 7 to 10) that were different from the sizes of the fragments of the CFP strains; an example is shown in Fig. 4, lane 6. PCR detection and characterization of the spa gene in CFN ORSA strains. Primers were derived from that part of the spa gene that encodes IgG-binding domains and were used for amplification. PCR performed with six control strains which were protein A positive by latex agglutination revealed the
1 2
3
4 5
6
7
8 9
10 11 12 13 14
kb
12,2
_-2,0
i
_ _ _ ~~~~~~~~~~~~0,52 FIG. 3. Plasmid analysis of ORSA strains. Lane 1, size marker (GIBCO Bethesda Research Laboratories, Berlin, Germany); lane 2, undigested plasmid from CFP ORSA; lane 3, undigested plasmid from outbreak strain; lane 4, plasmid in lane 2 digested with EcoRI; lanes 5 to 8, plasmids from four outbreak strains digested with EcoRI; lane 9, plasmid of the ORSA strain in lane 2 digested with BglII; lanes 10 to 13, plasmids from outbreak strains digested with BglII; lane 14, size markers (1-kb ladder; GIBCO Bethesda Research Laboratories).
2284
SCHWARZKOPF ET AL.
kb
1,01
M 1
2
3
4
J. CLIN. MICROBIOL.
5
6
7
8
9 10
-
0,51 __ 0,2980,154 -s
FIG. 4. PCR amplification and restriction enzyme digestion of the coagulase gene products from CFN ORSA strains from four different hospitals. Lane 1, PCR product from a CFP ORSA strain; lanes 2 to 5, PCR products from CFN ORSA strains; AluI restriction is shown for the CFP-ORSA strain in lane 6 and for the CFN-ORSA in lanes 7 to 10; lane M, size markers (1-kb ladder; GIBCO Bethesda Research Laboratories).
622-bp fragment (Fig. 5, lane 1), as expected from published nucleotide sequence data (19). Restriction with Hinfl identified three fragments of 141, 174, and 307 bp which fell in line with the nucleotide sequence (19). Six S. epidermidis strains gave no PCR product, further indicating that the PCR deployed in the present study is specific for the spa gene. When PCR was performed with all 50 CFN ORSA strains, identical PCR products of approximately 450 bp in length were found; examples are shown in Fig. 5, lanes 2 to 5. Restriction analysis of these PCR products revealed identical restriction fragment length polymorphism profiles; an example of this is shown in Fig. 5, lanes 7 to 10. Three fragments were found on acrylamide gels (data not shown). Two fragments of 140 and 170 bp shown in Fig. 5, lanes 7 to 10, seemed to be identical in size to the corresponding fragments of the protein A-positive control strains shown in Fig. 5, lane 6. In the agarose gel shown in Fig. 5, the third fragment of 130 bp could not be separated from the 140-bp fragment. Because in all CFN ORSA strains the PCR products were 170 bp smaller in size and it is precisely a fragment of this size that is required to encode one IgG-binding region,
kb
M l
2
3 4 5 6 7 8 910
101
0.51-9 0,298-_
0.1 45-
FIG. 5. PCR detection of the spa gene in CFN ORSA isolates from different hospitals. Lane 1, PCR products obtained from either a protein A latex agglutination test-positive strain or a CFP ORSA strain; lanes 2 to 5, PCR products from CFN ORSA strains; Hinfl restriction for the CFP ORSA strain is shown in lane 6; Hinfl restriction for the CFN ORSA strains is shown in lanes 7 to 10.
we assume that this fragment is not present in the CFN ORSA strains.
DISCUSSION Reliable identification of ORSA strains is of paramount importance for specific antibiotic treatment of patients suffering from infections caused by these pathogens. Likewise, to prevent cross-infections among patients and medical staff, laboratory diagnosis of ORSA is vital for hygienic control programs (3, 4). The ORSA strains reported here could not be identified by conventional laboratory analysis by latex agglutination tests for detection of clumping factor or protein A. All strains showed yellow-pigmented colonies, and it was this that prompted us to perform further characterization. A positive DNase reaction, tube coagulase activity, and biochemistry resulted in definitive identification of S. aureus. From the results of phenotyping and genotyping, we present evidence here that not only the CFN ORSA isolates from a recent outbreak but also CFN ORSA isolates involved in outbreaks in five other hospitals were identical to each other; there was only one exception to those findings in that a particular strain differed slightly in its antibiogram (cotrimoxazole resistant), and likewise, its PFGE pattern varied slightly. Molecular typing of ORSA strains is of great potential value for basic and epidemiological studies of S. aureus infections. In addition to PFGE of chromosomal DNA, which proved to be cumbersome and time-consuming, and therefore less practical for use in routine investigations, there is a strong tendency toward molecular typing of S. aureus by using variations in the chromosomal DNA structures (6, 12, 14). An interesting element in this connection is the coagulase gene, which comprises a region containing several 81-bp tandem repeats (10, 11); the number of these repeats differs among S. aureus strains. The value of this gene for molecular typing lies in whether the repeats differ in the presence or absence of AluI restriction sites. Goh et al. (7) recently analyzed 24 methicillin-resistant S. aureus isolates recovered from patients and staff members during an investigation of an outbreak. Of these epidemiologically related strains, 23 had identical coagulase restriction fragment length polymorphism profiles, but these profiles were different from those of epidemiologically unrelated S. aureus strains. Although we confirmed the essential value of coagulase genotyping when we investigated epidemiologically unrelated CFP ORSA stains, we were unable to distinguish the CFN ORSA strains from different hospitals. This probably means that they are identical even in this highly variable gene. An unexpected finding of the present study was the positive PCR result for the protein A gene in the strains, despite their negative phenotype for the protein A gene. The spa genes encode a protein that consists of two sets of remarkable amino acid repeats (19). The first set comprises 12 octapeptide repeats constituting the cell wall-attaching domain. The second set is made up of five repeats of 58 amino acid residues, and these repeats correspond to the IgG-binding domains (19). A new protein A gene has recently been described in S. aureus V8, which lacks one of the five IgG-binding domains (15). To characterize the immunoglobulin-binding region of the protein A gene from the CFN ORSA strains, we constructed primers to detect both of the protein A genes mentioned above. This strategy proved successful. The PCR products of the latex agglutination-positive strains were of the expected size, being in
CHARACTERIZATION OF OXACILLIN-RESISTANT S. AUREUS
VOL. 31, 1993
agreement with the size of a protein A gene that contains five IgG domains. All CFN ORSA strains provided a PCR product with a size consistent with that of a region comprising four IgG-binding domains. Since restriction analysis results were not in accordance with those published for the spa nucleotide sequence of strain V8 (5), it is evident that sequence analysis must be performed to characterize definitively the spa genes from the CFN ORSA strains. Recently, CFN ORSA has been described in Great Britain (13) and North America (20). The isolates described by Neville et al. (13) differed from the strains described here by the lack of DNase activity. Wanger et al. (20) reported on CFN ORSA strains isolated from infants in a newborn intensive care unit. In contrast to the strains reported on here, those isolates were susceptible to ciprofloxacin. Plasmid analysis of their strains revealed a single plasmid of approximately 100 kb. We had similar findings with the single plasmid in our isolates, but it was only 30 kb in size. What is particularly striking here is that the PFGE patterns shown by Wanger et al. (20) resemble ours, which might, we suggest, indicate global propagation. This would be in line with the concept recently announced by Kreiswirth et al. (12), who described the clonal origin of methicillin resistance in S. aureus. They showed that the mecA gene that encodes penicillin-binding protein 2a was acquired only once by S. aureus. The fact that transmission of infection with ORSA strains is so rapid and global suggests that a meeting of minds regarding standardization of fingerprinting would be indispensable to clarifying and simplifying work in this field worldwide. Finally, it should be pointed out that the attention paid to unusual ORSA strains such as those described here is well justified. Although no protein A and clumping factor, which are generally thought to be putative virulence factors, were detectable by latex agglutination, the strains must have the capacity to still be virulent. They spread with a great rapidity inside and outside hospitals as we have not yet observed. Their virulence is manifest by many patients who become seriously ill, two of whom even died in one outbreak. REFERENCES 1. Birnboim, H. C. 1983. A rapid alkaline extraction method for the isolation of plasmid DNA. Methods Enzymol. 100:243-255. 2. Bouvet, A., J. M. Fournier, A. Audurier, C. Branger, A. Orsoni, and C. Girard. 1990. Epidemiological markers for epidemic strain and carrier isolates in an outbreak of nosocomial oxacillin-resistant Staphylococcus aureus. J. Clin. Microbiol. 28: 1338-1341. 3. Brumfitt, W., and J. Hamilton-Miller. 1989. Methicillin-resistant Staphylococcus aureus. N. Engl. J. Med. 320:1188-1196. 4. Eadon, H. J., and R. J. Pinney. 1991. Methicillin-resistant Staphylococcus aureus-an overview. J. Clin. Pharm. Ther. 16:453-462. 5. Finck-Barbancon, V., G. Prevost, I. Mazurier, and Y. Piemont. 1992. A structurally novel staphylococcal protein A from the V8 strain. FEMS Microbiol. Lett. 91:1-8. 6. Goering, R. V., and T. D. Duensing. 1990. Rapid field inversion gel electrophoresis in combination with an rRNA gene probe in the epidemiological evaluation of staphylococci. J. Clin. Micro-
2285
biol. 28:426-429. 7. Goh, S. H., S. K. Byrne, J. L. Zhang, and A. W. Chow. 1992. Molecular typing of Staphylococcus aureus on the basis of coagulase gene polymorphisms. 30:1642-1645. 8. Hadorn, K., W. Lenz, F. H. Kayser, I. Shalit, and C. Krasemann. 1990. Use of a ribosomal RNA gene probe for the epidemiolgoical study of methicillin and ciprofloxacin resistant Staphylococcus aureus. Eur. J. Clin. Microbiol. Infect. Dis. 9:649-653. 9. Ichiyama, S., M. Ohta, K. Shimokata, N. Kato, and J. Takeuchi. 1991. Genomic DNA fingerprinting by pulsed-field gel electrophoresis as an epidemiological marker for study of nosocomial infections caused by methicillin-resistant Staphylococcus aureus. J. Clin. Microbiol. 29:2690-2695. 10. Kaida, S., T. Miyata, Y. Yoshizawa, H. Igarashi, and S. Iwanaga. 1989. Nucleotide and deduced amino acid sequence of staphylocoagulase gene from Staphylococcus aureus strain 213. Nucleic Acids Res. 17:8871. 11. Kaida, S., T. Miyata, Y. Yoshizawa, S. Kawabata, T. Morita, H. Igarashi, and S. Iwanaga. 1987. Nucleotide sequence of the staphylocoagulase gene: its unique COOH-terminal 8 tandem repeats. J. Biochem. 102:1177-1186. 12. Kreiswirth, B., J. Kornblum, R. D. Arbeit, W. Eisner, J. N. Maslow, A. McGeer, D. E. Low, and R. P. NovicL 1993. Evidence for a clonal origin of methicillin resistance in Staphylococcus aureus. Science 259:227-230. 13. Neville, L. O., 0. J. Billington, C. C. Kibbler, and S. H. Gillespie. 1991. Methicillin resistant Staphylococcus aureus without clumping factor, protein A and DNase. Lancet 338:518.
(Letter.) 14. Nicolle, L. E., H. Bialkowska-Hobrzanska, L. Romance, V. S. Harry, and S. Parker. 1992. Clonal diversity of methicillinresistant Staphylococcus aureus in acute-care institution. Infect. Control. Hosp. Epidemiol. 13:33-37. 15. Phonimdaeng, P., M. O'Reilly, P. Nowlan, A. J. Barmley, and T. J. Foster. 1990. The coagulase of Staphylococcus aureus 8325-4. Sequence analysis and virulence of site-specific coagulase-deficient mutants. Mol. Microbiol. 4:393-404. 16. Reboli, A. C., J. F. John, C. G. Platt, and J. R. Cantey. 1990. Methicillin-resistant Staphylococcus aureus outbreak at a Veteran's Affairs medical center; importance of carriage of the organism by hospital personnel. Infect. Control. Hosp. Epidemiol. 11:291-296. 17. Schlichting, C., C. Branger, J. M. Fournier, W. Witte, A. Boutonnier, C. Wolz, P. Goullet, and G. Doring. 1993. Typing of Staphylococcus aureus by pulsed-field gel electrophoresis, zymotyping, capsular typing, and phage typing: resolution of clonal relationships. J. Clin. Microbiol. 31:227-232. 18. Schwarzkopf, A., H. Schmidt-Rotte, H. Schmidt, E. Kunz, H. Karch, and J. Heesemann. 1992. Molecular analysis of nosocomial infection by oxacillin-resistant Staphylococcus aureus lacking protein A and clumping factor. Lancet 340:621. (Letter.) 19. Uhlen, M., B. Guss, B. Nilsson, S. Gatenbeck, L. Philipson, and M. Lindberg. 1984. Complete sequence of the staphylococcal gene encoding protein A. J. Biol. Chem. 259:1695-1702. 20. Wanger, A. R., S. L. Morris, C. Ericsson, K. V. Singh, and M. T. LaRocco. 1992. Latex agglutination-negative methicillinresistant Staphylococcus aureus recovered from neonates: epidemiologic features and comparison of typing methods. J. Clin. Microbiol. 30:2583-2588. 21. Zierdt, C. H., I. K. Hosein, R. Shively, and J. D. MacLowry. 1990. Phage pattern specific oxacillin-resistant Staphylococcus aureus in U.S. hospitals: epidemiological significance. J. Clin. Microbiol. 30:252-254.