SPD Sensory Processing Disorder: Facts, Assumptions and Myths
Jacci Siebert BSc (OT) Hons Specialist Children’s OT Advanced SI Practitioner & SI mentor
Sens.ations, Leicester, 7th March 2012
SPD is a barrier to engagement in OCCUPATION – OT - art and science of helping people do the day-today activities that are important to them despite impairment, disability, or handicap. – ‘Occupation’ in occupational therapy… refers to all the activities that occupy people’s time and give meaning to their lives.” (Neistadt & Blesedell Crepeau, 1998). – Occupational deprivation - opportunity to engage in occupations.
– Occupational justice principles – all people helped to live a life filled with meaningful and health-promoting occupation.
SPD facts • SPD is a complex disorder of the brain that affects developing children and adults. • Parent surveys, clinical assessments, and laboratory protocols exist to identify children with SPD. • At least 1 in 20 people in the general population may be affected by SPD. • In children who are gifted and those with ADHD, Autism, and fragile X syndrome, the prevalence of SPD is much higher than in the general population. • Studies have found a significant difference between the physiology of children with SPD and children who are typically developing. • Studies have found a significant difference between the physiology of children with SPD and children with ADHD. • SPD has unique sensory symptoms that are not explained by other known disorders. • Heredity may be one cause of the disorder. • Laboratory studies suggest that the sympathetic and parasympathetic nervous systems are not functioning typically in children with SPD. • Preliminary research data support decades of anecdotal evidence that OT is an effective intervention for treating the symptoms of SPD. from Sensational Kids: Hope and Help for Children With Sensory Processing Disorder (SPD ) p. 249-250 by Lucy Jane Miller, PhD, OTR
What is SPD? • Previously referred to as DSI or Sensory Integration Dysfunction. • First described and studied in the 1960s by A. Jean Ayres, an occupational therapist, educational psychologist and neuroscience researcher. • Causes: hereditary? prematurity? A.Jean Ayres 1920-1988
The term “Sensory Integration” can refer to: • Ayres’ theory of normal development
• A process of evaluating Sensory Processing Disorders (SPD) so we can better understand the behaviour we see in individuals. • A specific approach to intervention Ayres Sensory Integration®
7 SENSES
‘Far’ senses ‘Near’ Senses o Sight (Visual) o Sound (Auditory) o Smell (Olfactory)
• Taste (Gustatory) • Touch (Tactile) • Vestibular (movement and balance sense)-provides information about where the head and body are in space and in relation to the earth's surface.
• Proprioception (joint/muscle sense)-provides information about where body parts are and what they are doing .
Tactile + Proprioception = Somatosensory perception (body awareness)
Vestibular + Proprioception = Movement sense and postural control
Autonomic Nervous System
Typical ‘Brain’
Sound, Sight, Taste Touch, Smell, Body Position sense, Movement Sense
Response (timed and adapted to the environment)
The brain makes sense of the sensory input we gain from the environment and designs & implements an appropriate response.
Five interrelated components that help to explain how Sensory Integration occurs: • • • • •
Sensory Registration Orientation Interpretation Organization of a response Execution of a response
What are the results of Sensory Integration? • Self Regulation The nervous system’s ability to attain, maintain, and change levels of arousal or alertness.
• Motor Planning The process of deciding what your body has to do and then doing it (praxis).
SPD ‘Brain’
Sensory Info
Sensory seeker Sensory disregarder Sensory avoider Sensory sensitivity
Problems interpreting, modulating and discriminating sensory inputs: •Sensory defensiveness •Poor sensory awareness May or may not contribute to sensory distortions (receptor/brainstem/cortical problem): •Auditory distortions (hyperacuisis, tinnitus, misophonia) •Vertigo •Visual distortions (prosopagnosia, hallucinations) •Synaesthesia
Identifying Sensory Processing Disorder • 5-15 percent of general population (Miller, 2006) • Sensory processing impacts on occupation • SI trained therapist (typically OT) assesses client’s: – – – – –
Sensory Discrimination Sensory Modulation Posture, co-ordination, balance, motor skills Praxis Visual spatial organisation
What does SPD look like? • Symptoms and Red Flags – individuals experience sensations differently – more or less intensely, don’t get sensory messages right. ‘Sensory problems are chronic and disrupt everyday life’ (Miller, 2006). • Confusion about symptoms commonly result in other diagnoses being given (Oppositional Defiant Disorder, Failure to Thrive, Infantile Annorexia) (Miller, 2006) • Co-morbidity of SPD – ADHD, ASD • The road to an SPD diagnosis begins with a physician in order to rule out other neurological conditions.
What is the impact of SPD on function? • • • • •
Emotional regulation Social participation Play Learning Coping skills
Sensory Processing Problems • Sensory Registration Deficits Registration deficits limit the amount of sensation that the individual detects, thereby limiting relevant information from their perception. Registration is the initial point of perception from the sensory organs.
• Sensory Modulation Modulation deficits affect the way the individual perceives the intensity of the stimuli, thereby altering the ability to cope with, tolerate, or orient to the information, especially in the presence of stress, unexpected sensations, or in high stimulus environments.
• Sensory Discrimination Discrimination deficits lead to inadequate or distorted perceptions due to slow or inaccurate information processing about the details of the sensory input such as shape, size, location, quantity and quality.
Miller et al (2007) proposed Nosology for SPD Sensory Processing Disorder (SPD)
Sensory Modulation Disorder (SMD)
Sensory-Based Motor Disorder (SBMD) -Dyspraxia -Postural Disorder
-SOR -SUR -SS
SOR = sensory overresponsivity SUR = sensory underresponsivity SS = sensory seeking
Sensory Discrimination Disorder (SDD) -Visual -Auditory -Tactile -Vestibular -Proprioception -Taste/smell
Diagram from Pre-school Sensory Scan for Educators by Carol Stock Kranowitz
Sensory Integration Disorder
Sensory Modulation Disorder
Sensory Overresponsivity (Sensory Avoider)
Sensory Underresponsivity (Sensory Disregarder)
Sensory Discrimination Disorder (Sensory Jumbler)
Sensory Seeking (Sensory Craver)
Sensory based Motor Disorder
Postural Disorder (Sensory Slumper)
Dyspraxia (Sensory Fumbler)
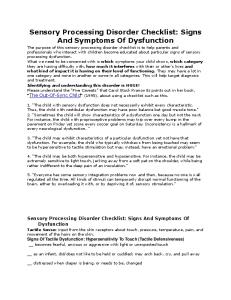
Sensory Profile by Winnie Dunn PhD, OTR , FAOTA • This is a standardised caregiver questionnaire which seeks to identify the nature of the child’s sensory processing
Neurological Threshold Continuum
Behavioural Response Continuum
HIGH (habituation)
Poor Registration
Sensory Seeking
Uninterested, Apathetic Dull affect Withdrawn “Overly tired” Self-absorbed
Active Continuously engaging Fidgety Excitable
Acting in ACCORDANCE with Threshold
Acting to COUNTERACT Threshold
difficulties. • Mainly looks at sensory modulation
Distractible Hyperactive
LOW (sensitization)
Sensitivity to Stimuli
Resistant to change Reliant on rigid rituals
Sensation Avoiding
Neurological Threshold Continuum
Behavioural Response Continuum
HIGH (habituation)
Bystander
LOW (sensitization)
Acting in ACCORDANCE with Threshold
Acting to COUNTERACT Threshold
Seeker
Easy-going and not easily ruffled, have to be called several times to get their attention, miss signposts, may leave dirt on their face or hands, find scratches and bruises and don’t know how they got them, don’t notice clutter until someone points it out.
Enjoy going to firework displays, make noises such as humming and whistling, order or cook spicy food, tend to touch people when talking to them, walk around barefoot, change daily routines to keep them interesting.
Distracted by sounds, startle easily, are bothered by fast changing images on TV, have precise ideas about clothing textures, repeatedly pick the same food in restaurants, prefer clean design in the home, select only a few chosen rides at amusement parks.
Leave the room when a crowd starts to gather, like their surroundings clean and tidy, keep curtains or blinds drawn or partially drawn, make narrow food choices, don’t like getting their hands mucky, select solitary leisure activities
Sensor Cited from “Living Sensationally” by Winnie Dunn
Avoider
The Aim of OT with children with SPD • Reframe the observable behaviour using sensory glasses – child is often then seen in a more positive light. • Provide a ‘toolbox’ of sensory related strategies for home and school. • Teach reasoning strategies to parents, carers or teachers so that tasks, environments, relationships can be modified for better functioning. • Direct therapy programme designed to improve quality of child’s life in 3 occupations central to childhood: school, play, self care.
Treatment methods • Occupational therapy (and physiotherapy) using various approaches : sensory-motor, psychosocial, neurodevelopmental, cognitive and motor learning approaches. • Occupational therapy using sensory stimulation and Sensory Diets: Henry OT – toolbox Alert programme Therapressure (Willbarger’s) Therapeutic Listening Programme Weighted or pressure vests Therapy balls as seat alternative • Occupational therapy using a Sensory Integration Approach (OT:SI): Ayres Sensory Integration® intervention or ASI
Sensory Integration Treatment Principles
Creation of a therapeutic environment Address underlying deficits in neural and sensory processing See movement, think sensory Provide planned and controlled sensory inputs designed to child’s specific needs Elicit an adaptive response to environmental demand Grade activities from simple to complex Use a child centred approach Use non-directive purposeful activities Balance of facilitation and inhibition Encourage active participation Capitalise on the child’s inner drive and self direction. To learn how to learn Therapy must be fun
Ayres SI Fidelity Tool (Parham et al, 2007)
Structural elements Professional background Clinical experience Room set up Type of equipment
Process elements Provide sensory opportunities Provide just-right challenge Collaborate on activity choice Guide self organisation Support optimal arousal Create play context Maximise child’s success Ensure physical safety Arrange room to engage child Foster therapeutic alliance
Author
Recent OT-SI Effectiveness Design SubjectsStudies Age Intervention Outcome range (years)
Smith 2005
ABAB OT-SI vs tabletop activities
7 PDD or 8-19 “Mental retardation”
5 sessions per week of 30 minutes
Significant reduction in self stimulatory behaviour
Miller 2007
OT-SI vs activity protocol vs no treatment
24 SMD (15 ADHD, 1 Anxiety)
3-11
20 x 1 hour sessions over 10 weeks
Significant gains in individualised GAS, Attention, Cognitive/social and reduced electrodermal responsivity ampitude
Pfeiffer 2011
OT-SI vs 37 ASD fine-motor
6-12
18 x 45 min sessions over 6 weeks
Significant positive changes in GAS (sensory processing, motor skills and social functioning)
Efficacy of ASI Intervention (May Benson and Koomar 2010, Pfeiffer et al 2011) Evidence suggests that SI may result in positive outcome in the areas of: – – – – – – – –
Sensorimotor skills Motor planning Socialization Attention Behavioral regulation Reading and reading related skills Individualized goals Autistic behaviors
Therapy Space
Mary Sheridan Centre, Lambeth (2004)
Russet House School, Enfield (2005)
Early diagnosis prevents long term issues developing • Plasticity remains throughout the lifespan, so its never too late, but a more optimal outcome is gained with early diagnosis and intervention. • Who benefits from screening for SPD? - Fussy babies with feeding and sleeping issues - Infants with atypical developmental milestones - All 0-5 year olds with suspected ASD and ADHD. - Majority of children with ASD - Majority of children with ADHD - Children & adults with motor learning and coordination difficulties, balance and muscle fatigue issues, fine motor and handwriting difficulties.
What happens when intervention is not available? • SMD
- secondary mental health complications, depression, borderline personality disorder, bipolar mood disorder, obsessive compulsive disorder. - possible drug and alcohol addiction. - antisocial behaviour. - relationships in family are stressed.
• SBMD
- poor self esteem, poor achievement despite clear strengths, social rejection.
Reasoning Strategies • A SECRET (Miller, 2006) A – Attention S – Sensation E – Emotion C – Culture R – Relationship E – Environment T – Task Cited from “Sensational Kids: Hope and Help for Children with Sensory Processing Disorder (SPD)” by Lucy Jane Miller, Ph.D., OTR
Support available • Books The Out-of-Sync child by Carol Stock Kranowitz Sensational Kids by Lucy Jane Miller Baby Sense by Megan Faure & Ann Richardson • Websites www.sensoryintegration.org.uk www.spdfoundation.net www.thespiralfoundation.org • Local services: screening & referral to OT via, GP, HV, SENCo, Paediatrician, Midwife.
• Independent Occupational Therapists www.cotss-ip.org.uk
Thank you for Listening
Contact details:
[email protected]
References •
•
•
•
• •
• •
Arbesman, M. & Lieberman, D. (2010) Methodology for the systematic reviews of occupational therapy for children and adolescents with difficulty processing and integration sensory information. American Journal of Occupational Therapy, 64 (3), 368374. Bagatell, N., Mirigliani, G., Patterson, C., Reyes, Y. & Test, L. (2010) Effectiveness of therapy ball chairs with autism spectrum disorders. American Journal of Occupational Therapy, 64 (6), 895-903. Ben-Sasson, A., Hen, L. Fluss, R. Cermak, S.A. Engel-Yeger, B. & Gal, E. (2009) A meta-analysis of sensory modulation symptoms in individuals with autistic spectrum disorder. Journal of Autism and Developmental Disorders, 39(1), 1-11 Ben-Sasson, A., Cermak, S.A., Orsmond, G.I. & Tager-Flusberg, H. (2007) Extreme sensory modulation behaviours in toddlers with autism spectrum disorders. American Journal of Occupational Therapy, 61 (5), 584-592. Brown, N.B. & Dunn, W. (2010) Relationship between context and sensory processing in children with autism. American Journal of Occupational Therapy, 64 (3) 474-483. Bundy, A.C., Shia, S., Qi, L. & Miller, L.J. (2007) How does sensory processing dysfunction affect play? American Journal of Occupational Therapy, 61(2), 201-208. Bundy, A.C., Murray, E. and Lane, S. (2002) Sensory Integration: Theory and Practice. 2nd edition. Philadelphia: FA Davies Co. Case-Smith, J. & Bryan, T. (1999) The effects of occupational therapy with sensory integration emphasis on preschool-age children with autism. American Journal of Occupational Therapy, 53(5), 489-497.
• •
• •
•
•
•
•
Gere, D.R., Capps, S.C., Mitchell, D.W. & Grubbs, E. (2009) Sensory sensitivities of gifted children. American Journal of Occupational Therapy, 63(3), 288-295. Lane, S.J. & Schaaf, R.C. (2010) Examining the neuroscience evidence for sensorydriven neuroplasticity: Implications for sensory-based occupational therapy for children and adolescents. American Journal of Occupational Therapy, 64 (3), 375-390. Lawlor, M.C. (2003) The significance of being occupied: The social construction of childhood occupations. American Journal of Occupational Therapy, 57(4), 424-434 Mailloux, Z., Mulligan, S., Smith Roley, S., Blanche, E., Cermak, S., Coleman, G.G., Bodison, S. & Lane, C.J. (2011) Verification and clarification of patterns of sensory integrative dysfunction. American Journal of Occupational Therapy, 65 (2), 143-151. May-Benson, T.A. & Koomar, J.A. (2010) Systematic review of the research evidence examining the effectiveness of interventions using a sensory integrative approach for children. American Journal of Occupational Therapy, 64 (3), 403-414. May-Benson, T.A., Koomar, J.A. & Teasdale, A. (2009) Incidence of pre, peri-, and postnatal birth and developmental problems of children with sensory processing disorder and children with autism spectrum disorder. Frontiers in Integrative Neuroscience, 3 (31), 112. Miller, L.J., Coll, J.R. & Schoen, S.A. (2007) A randomized controlled pilot study of the effectiveness of occupational therapy for children with sensory modulation disorder. American Journal of Occupational Therapy, 61 (2), 228-238. Miller, L.J., Anzalone, M.E., Lane, S.J., Cermak, S.A. & Osten, E.J. (2007) Concept evolution in sensory integration: a proposed nosology for diagnosis. American Journal of Occupational Therapy, 61 (2), 135-140.
•
•
•
• •
•
•
Parham, L.D., Smith Roley, S., May-Benson, T.A., Koomar, J., Brett-Green, B., Burke, J.P., Cohn, E.S., Mailloux, Z., Miller, L.J. & Schaaf, R.C. (2011) Development of a fidelity measure for research on the effectiveness of the Ayres sensory integration® intervention. American Journal of Occupational Therapy, 65 (2), 133-142. Pfeiffer, B.A., Koenig, K., Kinnealey, M., Sheppard, M. & Henderson, L. (2011) Effectiveness of sensory integration interventions in children with autism spectrum disorders: A pilot study. American Journal of Occupational Therapy, 65 (1), 76-85. Schaaf, R.C., & Nightlinger, K.M. (2007) Occupational therapy using a sensory integrative approach: A case study of effectiveness. American Journal of Occupational Therapy, 61 (2), 239-246. Schaaf, R.C. & Smith Roley, S.(2006) Sensory Integration: Applying clinical reasoning to practice with diverse populations. Austin, Texas. Pro-ed, Inc. Schilling, D.L., Washington, K., Billingsley, F.F. & Deitz, J. (2003) Classroom seating for children with attention deficit hyperactivity disorder: Therapy balls versus chairs. American Journal of Occupational Therapy, 57 (5), 534-541. Smith, S.A., Press, B., Koenig, K.P. & Kinnealey, M. (2005) Effects of sensory integration intervention of self-stimulating and self-injurious behaviour. American Journal of Occupational Therapy, 59 (4), 418-25. Stephenson, E.A. & Chesson, R.A. (2008) 'Always the guiding hand’: parents' accounts of the long-term implications of developmental coordination disorder for their children & families. Child: Care, Health and Development, 34 (3), 335-343.
SPD red flags for: • Infants and toddlers ____ Problems eating or sleeping ____ Refuses to go to anyone but me ____ Irritable when being dressed; uncomfortable in clothes ____ Rarely plays with toys ____ Resists cuddling, arches away when held ____ Cannot calm self ____ Floppy or stiff body, motor delays from www.spdfoundation.net
SPD red flags for: • Pre-schoolers ____ Over-sensitive to touch, noises, smells, other people ____ Difficulty making friends ____ Difficulty dressing, eating, sleeping, and/or toilet training ____ Clumsy; poor motor skills; weak ____ In constant motion; in everyone else's face and space ____ Frequent or long temper tantrums from www.spdfoundation.net
SPD red flags for: • Grade schoolers ___ Over-sensitive to touch, noise, smells, other people ___ Easily distracted, fidgety, craves movement; aggressive ___ Easily overwhelmed ___ Difficulty with handwriting or motor activities ___ Difficulty making friends ___ Unaware of pain and/or other people from www.spdfoundation.net
SPD red flags for: • Adolescents and adults ___ Over-sensitive to touch, noise, smells, and other people ___ Poor self-esteem; afraid of failing at new tasks ___ Lethargic and slow ___ Always on the go; impulsive; distractible ___ Leaves tasks uncompleted ___ Clumsy, slow, poor motor skills or handwriting ___ Difficulty staying focused ___ Difficulty staying focused at work and in meetings from www.spdfoundation.net