Journal of Neuropathology and Experimental Neurology Copyright q 2001 by the American Association of Neuropathologists
Vol. 60, No. 11 November, 2001 pp. 1021 1031
Refsum Disease, Peroxisomes and Phytanic Acid Oxidation: A Review RONALD J. A. WANDERS, PHD, GERBERT A. JANSEN, PHD,
AND
OLA H. SKJELDAL, MD
Abstract. Refsum disease was first recognized as a distinct disease entity by Sigvald Refsum in the 1940s. The discovery of markedly elevated levels of the branched-chain fatty acid phytanic acid in certain patients marked Refsum disease as a disorder of lipid metabolism. Although it was immediately recognized that the accumulation of phytanic acid is due to its deficient breakdown in Refsum disease patients, the true enzymatic defect remained mysterious until recently. A major breakthrough in this respect was the resolution of the mechanism of phytanic acid a-oxidation in humans. In this review we describe the many aspects of Refsum disease from the clinical signs and symptoms to the enzyme and molecular defect plus the recent identification of genetic heterogeneity in Refsum disease. Key Words:
Fatty acids; Genetic diseases; Peroxisomes; Refsum disease.
Clinical Symptoms and Signs
Refsum disease was first delineated as a distinct disease entity by Sigvald Refsum in 1946 (1) who originally called the disease Heredopathia Atactica Polyneuritiformis. According to Refsum the cardinal manifestations of the disease included retinitis pigmentosa, cerebellar ataxia, and chronic polyneuropathy, although the cerebellar ataxia starts late and is therefore not observed in all patients. A major breakthrough with respect to the underlying defect in Refsum disease came in the early 1960s when Klenk and Kahlke (2) reported the accumulation of an unusual 20-carbon, branched-chain fatty acid identified as 3,7,11,15-tetramethylhexadecanoic acid, better known as phytanic acid. These findings identified Refsum disease as an inborn error of lipid metabolism. Studies in the 1960s showed that the accumulation of phytanic acid is due to a defect in the breakdown of phytanic acid via a process called a-oxidation. Despite intense efforts, the mechanism of phytanic acid a-oxidation and the enzymes involved remained elusive until recently. Resolution of the structure of the phytanic acid a-oxidation pathway allowed the identification of the enzymatic defect in Refsum disease and its molecular basis, and also formed the basis for the discovery of genetic heterogeneity in Refsum diseases. In this review we describe the current state of knowledge about the adult form of Refsum disease (ARD), with particular emphasis on the most recent developments.
Patients in whom ARD is destined to develop appear to be perfectly normal as infants and do not show any obvious defects in growth and development. Onset has occasionally been detected in early childhood but not until the fifth decade in others. Most patients have clear-cut manifestations before 20 yr of age. In a study by Skjeldal et al (3) of 17 patients, 25% and 53% of the patients had their first clinical manifestations before 10 and 20 yr of age, respectively. Remarkably, Herbert and Clayton (4) reported on a patient with true Refsum disease who presented at a very young age (7 months) with developmental delay and hypotonia. The clinical picture of adult Refsum disease is often that of a slowly developing, progressive peripheral neuropathy manifested by severe motor weakness and muscular wasting, especially of the lower extremities. The ophthalmological and cerebellar abnormalities as well as the polyneuropathy observed in adult Refsum patients are briefly described below (see Wanders et al (5) for more extensive review).
From the Academic Medical Centre, University of Amsterdam, Departments of Pediatrics and Clinical Chemistry (RJAW, GAJ), Emma Children’s Hospital, Amsterdam, The Netherlands; and Riskhospitalet, Department of Pediatrics (OHS), Neuropediatric Section, Oslo, Norway. Correspondence to: Prof. Dr. Ronald J. A. Wanders, Academic Medical Centre, University Hospital Amsterdam, Room F0-224, P. O. Box 22700, 1100 DE Amsterdam, The Netherlands. The authors’ work has been financially supported by a grant from The Netherlands Organisation for Scientific Research (NWO project no. 901-03-159).
Ophthalmology Retinitis pigmentosa with constricted visual fields and night blindness are characteristic features of Refsum disease. In fact, retinitis pigmentosa seems to be present in all bona fide Refsum patients. Indeed, in a series of 17 patients described by one of us (3), retinitis pigmentosa was observed in all 17 patients. Usually the retinal degeneration is a very early sign and in many cases patients have complained of night blindness before the appearance of additional clinical symptoms (3, 6). A disturbed visual capacity, together with anosmia, are therefore the first clinical manifestations of the disease in most patients and should lead to prompt analysis of plasma phytanic acid in order to start therapy. Electroretinography (ERG) may show reduction or complete absence of rod and cone responses. Over the years, a concentric visual field constriction develops gradually, and finally only tubular vision remains.
1021
Downloaded from http://jnen.oxfordjournals.org/ by guest on January 23, 2017
INTRODUCTION
1022
WANDERS ET AL
Polyneuropathy The polyneuropathy observed in Refsum patients is of the mixed motor and sensory type, is symmetrical, and initially affects the distal parts of the lower limbs with muscular atrophy, muscle weakness, and sensory disturbances. The polyneuropathy is chronic and progressive although its onset may be preceded by visual and auditory disturbances for several years. In the early stages the polyneuropathy may occur episodically. Over the years, muscular weakness can become widespread and disabling, involving not only the limbs but also the truncal musculature. Peripheral sensory disturbances are also a general feature of Refsum patients (10). In most cases the deep sensation is impaired, particularly the vibration and positionmotion qualities in the distal parts of the legs. Neurological examination reveals loss of deep reflexes, mostly with ankle jerks. Generally, the plantar responses are flexor or absent. A reduced sensory nerve conduction velocity is usually found with sometimes very marked reductions. The pattern of conduction velocity slowing is not uniform as expected in patients with a demyelinative neuropathy (11). This is in accordance with the varying degrees of segmental demyelination as observed in nerve biopsies (10). A similar conclusion was reached by Kuntzer et al (12) who reported on the follow up of a patient over a 21-yr period. Cerebellar Abnormalities According to Refsum (1), cerebellar abnormalities are a central characteristic of Refsum patients. Subsequent studies, however, have shown that cerebellar symptoms are a much less common feature of the disease. In part, J Neuropathol Exp Neurol, Vol 60, November, 2001
this may be due to the fact that cerebellar anomalies usually present relatively late compared to the retinopathy and neuropathy. Unsteadiness of gait has been reported in Refsum patients, which has led to the misdiagnosis of Friedreich ataxia in some cases. Additional Clinical Features In addition to the features described above, Refsum patients may show additional abnormalities: 1) Anosmia is one of the early manifestations of the disease (10, 13) and warrants suspicion of Refsum disease, especially in conjunction with retinitis pigmentosa. 2) Hearing is usually also impaired, which is explained by the fact that both the olfactory and auditory nerves are affected. The loss of hearing is of the cochlear type with vestibule function usually unimpaired (14). 3) Cardiac abnormalities have been reported in patients, including cardiomyopathy with an enlargement of the heart, conduction disturbances, and electrocardiographic changes. Sudden death among Refsum patients has been reported repeatedly and has been ascribed to primary cardiac failure (15–17). 4) Skeletal malformations have been found, including bilateral shortening or elongation of the metatarsal bones, particularly the third and fourth metatarsals. Other malformations reported are syndactyly, shortened and widened digits or metacarpals, and hammer toes. These abnormalities have been described in about half of the patients (3). 5) Skin abnormalities may be predominant but can also be completely absent in patients. Cutaneous manifestations may range from a slightly dry skin, especially of the trunk, to florid ichthyosis (18–20). Phytanic Acid is Derived from Dietary Sources Only Studies on the distribution of phytanic acid among the various lipid fractions in plasma from Refsum patients have shown that very little phytanic acid is in the free unesterified form. Instead, most is present in triglycerides, and less in the form of phospholipids and cholesterol esters (21–23). Based on its polyisoprenoid-like structure, it was originally thought that phytanic acid might be synthesized endogenously in a way similar to the synthesis of other isoprenoids from acetate via the mevalonate pathway. However, in vivo studies both in humans and in experimental animals failed to show formation of phytanic acid from radiolabeled acetate or mevalonate, indicating that phytanic acid is derived from dietary sources only. Studies have shown that phytol and especially phytanic acid itself are the most important sources of phytanic acid in the human diet. These compounds are especially abundant in dairy products and ruminant fats. Ruminants ingest large quantities of chlorophyll, which undergoes effective degradation by resident bacteria present in the rumen. The phytol molecule released in this way can be converted into phytanic acid that can then be incorporated
Downloaded from http://jnen.oxfordjournals.org/ by guest on January 23, 2017
The retinal degeneration seems to be due to the excessive deposition of phytanic acid in ocular tissue (7). Pathological examinations have shown an almost complete loss of photoreceptors, thinning of the inner nuclear layer, and reduction in the number of ganglion cells of the retina (8). Often the typical ‘‘bony spicule type’’ of pigmentary retinal degeneration is lacking (‘‘retinitis pigmentosa sine pigmento’’), and the pigmentation appears as fine granules or has a ‘‘salt and pepper’’ type of appearance. According to some authors, 4%–5% of retinitis pigmentosa patients may have Refsum disease (9). In addition to retinitis pigmentosa, visual failure in Refsum patients may also be aggravated by optic atrophy, cataract, and vitreous opacities. Interestingly, although not mentioned by Refsum in his original patients, cataract is a frequent finding in Refsum patients found in half (3) to one third of the patients (10). Furthermore, nystagmus—usually of moderate degree—has also been recorded in about 25% of patients. Myosis and poor reaction of the pupils to light may also contribute to the poor vision in patients.
REFSUM DISEASE
1023
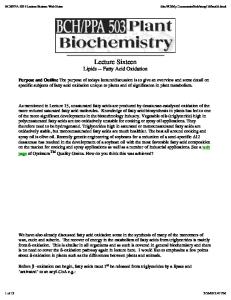
Fig. 1. Structure of phytanic acid, a 3-methyl-branched-chain fatty acid and its degradation by a-oxidation to pristanic acid plus CO2. Pristanic acid is a 2-methyl-branched-chain fatty acid that undergoes b-oxidation.
Deficient Oxidation of Phytanic Acid in Refsum Disease The discovery by Klenk and Kahlke (2) of the accumulation of phytanic acid in Refsum patients was soon followed by studies to identify the underlying defect. Studies done by Stoffel and Kahlke (24) and Steinberg et al (25, 26) using radioactively labeled phytol and phytanic acid administered to patients revealed that Refsum patients were unable to degrade phytanic acid. It was immediately recognized that phytanic acid could not undergo straightforward b-oxidation due to the presence of a methyl-group at the 3-position, which prohibits this breakdown pathway. Although several possible mechanisms of oxidation were suggested, it became clear that the most likely mechanism would be a-oxidation, in which the terminal carboxyl-group of phytanic acid is removed to produce CO2 and a new fatty acid, pristanic acid (2,6,10,14-tetramethylpentadecanoic acid), which is 1 carbon atom shorter and has the methyl-group at the 2position (Fig. 1). 2-Methyl fatty acids can undergo normal b-oxidation in contrast to 3-methyl fatty acids. Studies by Mize et al (27), in which phytol and phytanic acid were administered to mice, led to the identification of pristanic acid as the decarboxylation product of phytanic acid indicating that phytanic acid indeed undergoes aoxidation. In addition to pristanic acid, other products were found, including 4,8,12-trimethyltridecanoic acid and 4,8-dimethylnonanoic acid, which are the expected products of b-oxidation of pristanic acid. These findings set the stage for subsequent studies aimed to resolve the mechanism of a-oxidation and the enzymes involved. Detailed studies by Steinberg et al (28) and others suggested that the oxidation of phytanic acid does not involve its coenzyme A ester, which is usually the case for fatty acids, but that free phytanic acid is the true substrate
for a-oxidation. Furthermore, evidence was brought forward suggesting that 2-hydroxyphytanic acid is an intermediate in the a-oxidation pathway and that mitochondria are the site of phytanic acid a-oxidation, classifying Refsum disease as a mitochondrial disorder (28, 29). As we know now, these conclusions are incorrect as will be described below. Phytanic Acid a-Oxidation: Resolution of the Structure of the Pathway, Characterization of the Enzymes Involved, and Identification of Peroxisomes, not Mitochondria, as the Sole Site of Phytanic Acid a-Oxidation Several experimental observations in the late 1980s/ early 1990s led to the notion that the proposed mechanism of a-oxidation and its subcellular localization as proposed by Steinberg et al could not be correct. The first clue came when Poulos et al (30, 31) reported that fibroblasts from Zellweger patients in which peroxisomes are lacking are unable to a-oxidize phytanic acid, suggesting that a-oxidation is a peroxisomal process. Furthermore, we and others found that the rates of phytanic acid oxidation in intact cells were much higher as compared to homogenates, indicating that conclusions drawn from experiments with homogenates needed revision. Two major observations have revolutionized our way of thinking about a-oxidation. First, Watkins et al (32) presented convincing evidence suggesting that phytanoylCoA and not phytanic acid is the true substrate for aoxidation. Second, following up on these findings, Mihalik et al (33) discovered a new enzyme, phytanoyl-CoA hydroxylase (PHYH), which converts phytanoyl-CoA into 2-hydroxyphytanoyl-CoA. This enzyme turned out to require 2-oxoglutarate, Fe21 and ascorbate in order to be catalytically active. Furthermore, it was demonstrated that the enzyme is localized in peroxisomes (33–35), in line with the notion first put forward by Poulos et al (30) that phytanic acid a-oxidation is localized in peroxisomes, at least in part. Studies in recent years have also resolved the remainder of the pathway. It turns out that 2-hydroxyphytanoylCoA is cleaved by the enzyme 2-hydroxyphytanoyl-CoA J Neuropathol Exp Neurol, Vol 60, November, 2001
Downloaded from http://jnen.oxfordjournals.org/ by guest on January 23, 2017
into ruminant fats. Green vegetables contain massive amounts of phytol since each chlorophyll molecule contains 1 molecule of phytol. Nevertheless, green vegetables do not appear to be an important source of phytol/ phytanic acid since humans appear to be unable to release the phytol from the chlorophyll molecule.
1024
WANDERS ET AL
Fig. 2. Enzymology of the phytanic acid a-oxidation pathway. Phytanic acid first undergoes activation to phytanoyl-CoA followed by hydroxylation of phytanoyl-CoA to 2-hydroxyphytanoyl-CoA as catalyzed by the enzyme phytanoyl-CoA hydroxylase. Subsequently, 2-hydroxyphytanoyl-CoA is cleaved into pristanal and formyl-CoA followed by dehydrogenation to pristanic acid. After activation to pristanoyl-CoA, b-oxidation takes place.
lyase into formyl-CoA (the CoA-ester of CO2) and pristanal (36, 37). The enzyme involved is localized in peroxisomes as concluded from subcellular fractionation studies (38). Studies by Foulon et al (39) have shown that the protein is equipped with a PTS1-signal directing it to peroxisomes. The pristanal formed in the lyase reaction is oxidized to pristanic acid via an aldehyde dehydrogenase (Fig. 2). It was initially reported that this aldehyde dehydrogenase would be localized in the endoplasmic reticulum but recent evidence suggests that peroxisomes contain endogenous pristanal dehydrogenase activity (40). The nature of this enzyme remains to be determined. Finally, in order to allow pristanic acid to undergo b-oxidation, pristanic acid needs to be activated to its CoA-ester. It turns J Neuropathol Exp Neurol, Vol 60, November, 2001
out that peroxisomes contain 2 distinct synthetases capable of pristanoyl-CoA formation. The first enzyme is long-chain acyl-CoA synthetase (LACS), localized at the outer aspect of the peroxisomal membrane (41). Recently, Steinberg et al (42) identified another acyl-CoA synthetase with its catalytic site exposed to the peroxisomal matrix that also reacts with pristanic acid. This enzyme, called VLACS (very long chain acyl-CoA synthetase), may well be the enzyme that converts intraperoxisomal pristanic acid to pristanoyl-CoA. We have postulated (40) that the other synthetase, i.e. LACS, is involved in the activation of pristanic acid derived directly from dietary sources (Fig. 3). Phytanoyl-CoA Hydroxylase Deficiency: The Enzyme Defect in Adult Refsum Disease and Its Molecular Basis The discovery of phytanoyl-CoA hydroxylase by Mihalik et al (33) immediately suggested that the deficient aoxidation of phytanic acid in Refsum disease may result from a deficiency of this enzyme, which indeed turned out to be true (43). We subsequently purified the PHYH protein from rat liver peroxisomes and used this to clone the PHYH cDNA, allowing resolution of the molecular basis of Refsum disease for the first time (44). In 5 Refsum disease patients different mutations were found, including 1) a single nucleotide deletion leading to a frame shift and subsequently a premature stop codon, 2) an inframe deletion of 111 nucleotides resulting in a protein lacking 37 amino acids, and 3) a missense mutation (805A . C) resulting in the substitution of a histidine for an asparagine (Asn 269 His), which leads to an inactive enzyme as shown by expression studies. Using a different
Downloaded from http://jnen.oxfordjournals.org/ by guest on January 23, 2017
Fig. 3. Schematic representation of the subcellular localization of the phytanic acid a-oxidation machinery. We hypothesize that the 2 acyl-CoA synthetases (i.e. LACS and VLCAS) play different roles, with VLACS being involved in the phytanic acid a-oxidation per se, whereas LACS catalyses the activation of dietary pristanic acid (40).
1025
REFSUM DISEASE
Fig. 4.
Schematic representation of the phytanoyl-CoA hydroxylase gene and the different mutations found.
Phytanoyl-CoA Hydroxylase is Also Deficient in Peroxisomes Biogenesis Disorders and Rhizomelic Chondrodysplasia Punctata Type 1 Earlier studies had already shown that plasma phytanic acid is not only increased in Refsum disease patients but also in patients affected by a peroxisome biogenesis defect (PBD) (31), including rhizomelic chondrodysplasia punctata Type 1 (47). In all cases phytanoyl-CoA hydroxylase turned out to be deficient (35, 43, 48). The disorders of peroxisome biogenesis include Zellweger syndrome, neonatal adrenoleukodystrophy and infantile Refsum disease, and other phenotypes not easily assignable to each of these categories. In these PBD patients peroxisome formation is defective due to mutations in one of the many genes involved in peroxisome biogenesis (49). As a consequence, peroxisomes are deficient, resulting in generalized loss of peroxisomal functions including phytanic acid a-oxidation (50). Indeed, in the absence of peroxisomes, phytanoyl-CoA hydroxylase is being synthesized but is not active, probably because of its rapid degradation in the cytosol as shown for other peroxisomal enzymes. Rhizomelic chondrodysplasia punctata (RCDP) is another peroxisomal disorder characterized by severe growth failure, proximal shortening of the extremities, contractures, spasticity, mental retardation, and cataracts. Importantly, RCDP is genetically heterogeneous with 3 distinct genetic forms (50). Phytanic acid is only elevated in RCDP Type 1, which is caused by mutations in the PEX7 gene, resulting in a defective PTS2-receptor.
In order to understand the action of the PTS2-receptor, the process of peroxisome formation must be discussed in some detail. The generally accepted idea is that peroxisomes can not be synthesized de novo but originate from pre-existing peroxisomes via fission, after which the daughter peroxisomes take up new peroxisomal proteins from the cytosol. It turns out that most proteins destined for peroxisomes are equipped with a specific peroxisome targeting signal (PTS) contained within the polypeptide chain itself. Two such targeting signals have been identified. The PTS1 signal involves a carboxyterminal tripeptide of the general configuration S (A,C)–K (R,H)–L (M). This motif is found in many peroxisomal proteins, notably matrix proteins. The second PTS (PTS2) is localized near the aminoterminal end of peroxisomal proteins and has the following consensus motif: Xn–RL–X5– HL–Xn where X may be any amino acid. The PTS1 and PTS2 signals in peroxisomal proteins are recognized by 2 distinct receptors, the PTS1- and PTS2-receptor, encoded by the PEX5- and PEX7-genes, respectively. The loaded receptors are then recognized by specific components of the peroxisomal membrane, subsequently followed by translocation of the respective peroxisomal proteins across the peroxisomal membrane and recycling of the receptors back to the cytosol to participate in another round of peroxisomal protein uptake (Fig. 5). PhytanoylCoA hydroxylase is a typical PTS2-protein with the sequence RLQIVLGHL at amino acid positions 9 through 17 of the protein. This clearly explains why phytanoylCoA hydroxylase is also deficient in RCDP Type 1, like the other 2 peroxisomal PTS2-proteins, alkyl-dihydroxyacetonephosphate synthase (alkyl-DHAP synthase) and peroxisomal thiolase. Laboratory Diagnosis of Refsum Disease If a patient is suspected of having Refsum disease, therapy should be initiated as soon as possible if plasma phytanic acid is found to be elevated. Available data suggest that plasma phytanic acid is an excellent marker for the disease with no reports in the literature of false negatives. It should be emphasized that phytanic acid is not J Neuropathol Exp Neurol, Vol 60, November, 2001
Downloaded from http://jnen.oxfordjournals.org/ by guest on January 23, 2017
approach, Mihalik et al (45) also cloned the human PHYH cDNA and also described mutations in Refsum patients. We recently determined the structure of the PHYH gene, which spans 21.5 kb on chromosome 10p of the human genome (46). The gene contains 9 exons and 8 introns and codes for a mRNA of 1.6 kb. The availability of the PHYH gene structure has allowed us to perform molecular studies at the genomic rather than cDNA level. As has been reported (46), many different mutations were found in Refsum patients (Fig. 4).
1026
WANDERS ET AL
Downloaded from http://jnen.oxfordjournals.org/ by guest on January 23, 2017
Fig. 5. Current model of peroxisome biogenesis. Peroxisomal matrix proteins are synthesized on soluble ribosomes in the cytosol and contain either a carboxyterminal PTS1-signal or a PTS2-signal in the N-terminal part of the protein. Most peroxisomal matrix proteins are equipped with a PTS1-signal, whereas few proteins are known with a PTS2-signal. At present only 3 PTS2proteins (PTS2p) are known in humans, including phytanoyl-CoA hydroxylase. In the cytosol, PTS1-proteins and PTS2-proteins are recognized by their respective receptors, i.e. Pex5p, the PTS1-receptor and Pex7p, the PTS2-receptor, respectively. The loaded receptors subsequently form a complex which docks at the peroxisomal membrane with Pex14p, Pex13p, and Pex17p as key components involved in the docking process. Subsequently, the PTS1- and PTS2-proteins are translocated across the peroxisomal membrane with the help of Pex12p, Pex10p, Pex2p, and Pex8p. The 2 receptors are recycled with the help of Pex1p and Pex6p after which the receptors are ready for another round of protein import.
J Neuropathol Exp Neurol, Vol 60, November, 2001
1027
REFSUM DISEASE
TABLE Biochemical Characteristics of the 2 Groups of Refsum Disease Patients Mapped to 2 Different Loci and RCDP Patients Refsum disease patients Parameters measured Plasma Phytanic acid Fibroblasts ● Whole cell assays Phytanic acid a-oxidation De novo plasmalogen biosynthesis ● Peroxisomal PTS2-enzymes Phytanoyl-CoA hydroxylase Alkyl-DHAP synthase Peroxisomal thiolase ● Peroxisome morphology
Group 1 (10p13)
Group 2 (non-10p13)
RCDP Type 1
↑
↑
↑
↓↓ N
↓↓ ↓
↓ ↓↓↓
↓↓ N N N
↓↓ ↓ ↓ N
↓↓ ↓↓ ↓↓ N
Abbreviation: N 5 normal.
Refsum Disease is Genetically Heterogeneous Recent data have shown that Refsum disease is genetically heterogeneous. First, mapping studies by Wierzbicki et al (51) suggested the existence of 2 loci involved in Refsum disease of which 1 locus on chromosome 10 had to correspond to phytanoyl-CoA hydroxylase deficiency since the PHYH gene is localized on 10p13. Second, our own studies also revealed genetic heterogeneity. Indeed, we failed to identify mutations in the PHYH gene in a subset of patients. In collaboration with the Wierzbicki group we have now resolved the genetic defect in the group of patients mapped to the other locus (manuscript in preparation). To our surprise the gene affected in these patients is the PEX7 gene—the same gene as the one mutated in rhizomelic chondrodysplasia punctata. This conclusion is derived from the following observations. Studies in fibroblasts from these patients revealed that except for phytanoyl-CoA hydroxylase deficiency, there were additional abnormalities reminiscent of those observed in fibroblasts from rhizomelic chondrodysplasia punctata Type I patients, including a deficient de novo plasmalogen synthesis, deficient alkyl-dihydroxyacetonephosphate synthase (alkyl-DHAP synthase) and dihydroxyacetonephosphate acyltransferase activity, and a deficiency of 41kDa peroxisomal thiolase. Although the extent of the deficiencies was milder in fibroblasts from the non-phytanoyl-CoA hydroxylase mutated patients, the same set of abnormalities was found in RCDP Type 1 fibroblasts (Table). Mutation analysis of the PEX7 gene
which is mutated in RCDP Type 1 (52–54), revealed definitive mutations in these Refsum patients, thus establishing the molecular defect in these patients (Van den Brink et al, in preparation). It is remarkable that mutations within the same gene, i.e. the PEX7 gene, can give rise to such widely different clinical entities as rhizomelic chondrodysplasia punctata on one end of the spectrum and Refsum disease on the other. The genetic heterogeneity of Refsum disease is further emphasized by our recent findings of 2-methylacyl-CoA racemase deficiency in some patients with a late-onset sensory neuropathy with some features reminiscent of Refsum disease (55). In these patients both phytanic acid and pristanic acid are elevated, in contrast to true Refsum patients in which only phytanic acid is elevated. Therapy of Refsum Disease The fact that phytanic acid stems exclusively from exogenous sources makes Refsum disease amenable to dietary therapy. For effective treatment, dairy products and ruminant fats, the main sources of dietary phytanic acid, must be eliminated from the diet. Initially, green vegetables were excluded from the diet as well, but the poor availability of chlorophyll-bound phytol indicates that this is not necessary. Reduction of plasma phytanic acid levels by dietary treatment has been documented for many years and in some patients serum phytanic acid levels may even reach normal values, although in most patients the level falls considerably without normalizing completely. Most of the patients show definite clinical improvement (13) although the improvement of clinical symptoms may be slow. The same is true for plasma phytanic acid levels which usually drop slowly, probably due to the large body-stores of phytanic acid. Plasmapheresis has been used in Refsum patients mostly as an adjunct to dietary therapy with the aim of achieving a more rapid decrease of phytanic acid. The J Neuropathol Exp Neurol, Vol 60, November, 2001
Downloaded from http://jnen.oxfordjournals.org/ by guest on January 23, 2017
specific for this disease since it may also accumulate in other genetic diseases as discussed above. In principle, the finding of an elevated plasma phytanic acid level should be followed by detailed studies, preferably in fibroblasts, to establish whether phytanoyl-CoA hydroxylase activity is deficient or not, and if so, to resolve the molecular basis by doing mutation analysis.
1028
WANDERS ET AL
dietary treatment of patients has changed the natural course of the disease to a large extent. Although many symptoms of the disease respond favorably to treatment, the progression of retinitis pigmentosa, polyneuropathy, and hearing loss usually stabilize without actually improving. On the other hand, the prognosis of untreated cases is doubtful as can be concluded from the fate of Refsum’s original patients. Indeed, 10 of the 11 patients developed blindness. Furthermore, half of the untreated patients had died before 30 yr of age. The most probable cause of death in untreated patients is heart failure due to cardiomyopathy, both in young and middle-aged patients. Recent studies by Mukherji and co-workers (56) have suggested that there may be new treatments using the principle of chemical co-substrate rescue of phytanoylCoA hydroxylase, at least in some cases. These workers studied 2 common point mutations in human phytanoylCoA hydroxylase, R275W and R275Q, present at an allele frequency of 7.5% and 12.5%, respectively, in Dutch/ Scandinavian patients with adult Refsum disease (44, 46). Sequence analyses had revealed that the arginine at position 275 (Arg-275, R275) is conserved in all reported hydroxylases. Furthermore, analysis of the sequences in the light of crystal structures for 2 other 2-oxoglutarate dependent oxygenases suggested that Arg-275 in human J Neuropathol Exp Neurol, Vol 60, November, 2001
phytanoyl-CoA hydroxylase must be involved in binding the 5-carboxylate moiety of the co-substrate (normally: 2-oxoglutarate) via an electrostatic interaction. The authors postulated that the R275Q and R275W mutants were inactive due to defective binding of 2-oxoglutarate as caused by the changed configuration of the 2-oxoglutarate binding site, and that it may be possible to rescue the activity of phytanoyl-CoA hydroxylase using alternative 2-oxoacids. Remarkably, this proved to be true. The R275W mutant was significantly rescued with 2-oxobutyrate, 2-oxovalerate, 2-oxoisocaproate, and 2-oxo-5thiahexanoate as co-substrates instead of 2-oxoglutarate, which was completely inactive. In the case of the R275Q mutant pyruvate, 2-oxobutyrate and 2-oxo(iso)valerate were the best substrates. Figure 6 is a schematic representation of the principle of co-substrate rescue in case of the R275W mutant. Future studies should address whether phytanic acid a-oxidation can be induced by increasing the concentration of alternative 2-oxoacids such as pyruvate, 2-oxovalerate and 2-oxo-5-thiahexanoate. Several of the 2-oxoaxids that rescue the activity of the clinically observed R275W and R275Q mutants are generated in vivo from certain amino acids, e.g. 2-oxovalerate from valine, and 2-oxo-5-thiahexanoate from methionine. Thus, certain forms of adult Refsum disease
Downloaded from http://jnen.oxfordjournals.org/ by guest on January 23, 2017
Fig. 6. Chemical co-substrate rescue of a phytanoyl-CoA hydroxylase mutant (R275W). In case of the wild-type enzyme, the guanidino group of arginine at position 275 (Arg-275) interacts with the 5-carboxylate of 2-oxoglutarate. A: In case of the mutant enzyme with a tryptophane (Trp) at position 275, interaction between the aromatic side-chain of Trp-275 and the 5-carboxylate of 2-oxoglutarate is unfavorable. B: However, interaction is favorable in case of the alternative 2-oxoacid, i.e. 2-oxo-5-thiahexanoate, a metabolite of the methionine degradative pathway.
1029
REFSUM DISEASE
might be treated via dietary supplementation of the appropriate amino acids. Pathogenesis
ACKNOWLEDGMENTS The authors gratefully acknowledge Mrs. Maddy Festen for expert preparation of the manuscript and Dr. Jos Ruiter for artwork.
REFERENCES 1. Refsum S. Heredopathia atactica polyneuritiformis. Acta Psychiatr Scand (Suppl) 1946;38:1–303 2. Klenk E, Kahlke W. Ueber das Vorkommen der 3,7,11,15-Tetramethylhexadecansaure (phytansaure) in den Cholesterinestern und anderen Lipidfraktionen der Organe bei einem Krankheitsfall unbekanter Genese (Verdacht auf Heredopathia atactica polyneuritiformis, Refsum’s syndrome). Hoppe Seylers Z Physiol Chem 1963; 333:133–39 3. Skjeldal OH, Stokke O, Refsum S, Norseth J, Petit H. Clinical and biochemical heterogeneity in conditions with phytanic acid accumulation. J Neurol Sci 1987;77:87–96 4. Herbert MA, Clayton PT. Phytanic acid alpha-oxidase deficiency (Refsum disease) presenting in infancy. J Inherit Metab Dis 1994; 17:211–14 5. Wanders RJA, Jakobs C, Skjeldal OH. Refsum Disease. In: Scriver CR, Beaudet AL, Sly WS, Valle D, eds. The metabolic & molecular bases of inherited disease. New York: McGraw-Hill, 2001:3303–21 6. Claridge KG, Gibberd FB, Sidey MC. Refsum disease: The presentation and ophthalmic aspects of Refsum disease in a series of 23 patients. EYE 1992;6:371–75 7. Levy IS. Refsum’s syndrome. Trans Ophthalmol Soc U K 1970;90: 181–86 8. Toussaint D, Danis P. An ocular pathologic study of Refsum’s syndrome. Am J Ophthalmol 1971;72:342–47 9. Goldman JM, Clemens ME, Gibberd FB, Billimoria JD. Screening of patients with retinitis pigmentosa for heredopathia atactica polyneuritiformis (Refsum’s disease). Br Med J 1985;290:1109–10 10. Skjeldal OH. Heredopathia actactica polyneuritiformis (Refsum’s disease). In: Moser HW, ed. Handbook of clinical neurology. Amsterdam: Elsevier Science BV, 1996:485–503 11. Lewis RA, Sumner AJ. The electrodiagnostic distinctions between chronic familial and acquired demyelinative neuropathies. Neurology 1982;32:592–96
J Neuropathol Exp Neurol, Vol 60, November, 2001
Downloaded from http://jnen.oxfordjournals.org/ by guest on January 23, 2017
Although much has been learned about the biochemical and genetic basis of Refsum disease, much less is known about the mechanism by which the accumulation of phytanic acid leads to the clinical manifestations of Refsum disease, including the ophthalmological and neurological manifestations. As described before, electroretinography studies have shown reduction or even the complete absence of rod and cone responses. Furthermore, pathological examinations have revealed an almost complete loss of photoreceptors, thinning of the inner nuclear layer, and reduction of the number of ganglion cells of the retina. It could be that these phenomena are due to the deleterious effect of phytanic acid since it is readily incorporated into phospholipids. In this respect it should be noted that photoreceptor cells are rich in docosahexaenoic acid (DHA), and recent studies have shown that rat retina photoreceptor cells depend on docosahexaenoic acid for their survival and differentiation, since in the absence of DHA, photoreceptor cell apoptosis is markedly increased. Although DHA is normal in Refsum patients, at least in plasma and erythrocyte membranes (Wanders et al, unpublished), it could well be that phytanic acid through its incorporation in phospholipids disturbs photoreceptor membranes. This is now under active study. Whether this membrane distortion hypothesis is also responsible for the polyneuropathy observed in Refsum patients, which is of the mixed motor and sensory type and mainly affects the distal parts of the lower limbs with muscular atrophy, weakness, and sensory disturbances, remains to be established. Recent studies have shown that phytanic acid is an effective regulator of gene expression by virtue of its capacity to activate certain nuclear receptors, which may well have important consequences for the pathophysiology of Refsum disease. The first evidence suggesting that phytol-derived metabolites may be circulating dietary factors activating nuclear receptors was brought forward by Kitareewan et al (57) who found that phytanic acid is a ligand for all 3 retinoic-X-receptors, RXRa, b, and g. These receptors belong to the large family of nuclear receptors that includes the estrogen receptors, thyroid hormone receptors, the retinoic acid receptors (RARs), the retinoid-X receptors (RXRs) and the more recently identified group of peroxisome proliferator activated receptors (PPARs) (58). More recent studies have shown that phytanic acid is also a potent activator of some of the PPARs, including PPARa (59, 60). Recent studies by Seedorf et al (61) suggest that these in vitro effects of phytanic acid are also observed under in vivo conditions and that phytanic acid is indeed a potent modulator of gene expression affecting nuclear signal transduction pathways. This became especially clear
through studies in mutant mice in which the gene coding for sterol carrier protein X, catalyzing the last step in pristanic acid b-oxidation, was disrupted (61). These mutant mice were completely free of symptoms on a normal laboratory diet but developed severe abnormalities when phytol was added to the diet, which led to drastically increased levels of both pristanic and phytanic acid. The abnormalities observed in the mice included lethargy, reduced muscle tone, ataxia, loss of body weight, and a peripheral neuropathy with uncoordinated movements, unsteady gait, and trembling. Gene expression was found to be greatly altered with increased expression of a series of genes, including the gene coding for liver fatty acid binding protein (L-FABP) and enzymes of mitochondrial and peroxisomal b-oxidation. Furthermore, several genes were also reduced in expression. The implications of these findings for Refsum disease remain to be established. In this respect the availability of a mouse model for Refsum disease is warranted. Construction of such a mouse model is underway.
1030
WANDERS ET AL
J Neuropathol Exp Neurol, Vol 60, November, 2001
33. Mihalik SJ, Rainville AM, Watkins PA. Phytanic acid alpha-oxidation in rat liver peroxisomes. Production of alpha-hydroxyphytanoyl-CoA and formate is enhanced by dioxygenase cofactors. Eur J Biochem 1995;232:545–51 34. Croes K, Casteels M, de Hoffmann E, Mannaerts GP, Van Veldhoven PP. alpha-Oxidation of 3-methyl-substituted fatty acids in rat liver. Production of formic acid instead of CO2, cofactor requirements, subcellular localization and formation of a 2-hydroxy-3methylacyl-CoA intermediate. Eur J Biochem 1996;240:674–83 35. Jansen GA, Mihalik SJ, Watkins PA, et al. Phytanoyl-CoA hydroxylase is present in human liver, located in peroxisomes, and deficient in Zellweger syndrome: Direct, unequivocal evidence for the new, revised pathway of phytanic acid alpha-oxidation in humans. Biochem Biophys Res Commun 1996;229:205–10 36. Croes K, Casteels M, Asselberghs S, Herdewijn P, Mannaerts GP, Van Veldhoven PP. Formation of a 2-methyl-branched fatty aldehyde during peroxisomal alpha-oxidation. FEBS Lett 1997;412: 643–45 37. Verhoeven NM, Schor DS, ten Brink HJ, Wanders RJA, Jakobs C. Resolution of the phytanic acid alpha-oxidation pathway: Identification of pristanal as product of the decarboxylation of 2-hydroxyphytanoyl-CoA. Biochem Biophys Res Commun 1997;237:33–36 38. Jansen GA, Verhoeven NM, Denis S, et al. Phytanic acid alphaoxidation: Identification of 2-hydroxyphytanoyl-CoA lyase in rat liver and its localisation in peroxisomes. Biochim Biophys Acta 1999;1440:176–82 39. Foulon V, Antonenkov VD, Croes K, et al. Purification, molecular cloning, and expression of 2-hydroxyphytanoyl-CoA lyase, a peroxisomal thiamine pyrophosphate-dependent enzyme that catalyzes the carbon-carbon bond cleavage during alpha-oxidation of 3methyl-branched fatty acids. Proc Natl Acad Sci U S A 1999;96: 10039–44 40. Jansen GA, van den Brink DM, Ofman R, Draghici O, Dacremont G, Wanders RJA. Identification of pristanal dehydrogenase activity in peroxisomes: Conclusive evidence that the complete phytanic acid alpha-oxidation pathway is localized in peroxisomes. Biochem Biophys Res Commun 2001;283:674–79 41. Wanders RJA, Denis S, van Roermund CWT, Jakobs C, ten Brink HJ. Characteristics and subcellular localization of pristanoyl-CoA synthetase in rat liver. Biochim Biophys Acta 1992;1125:274–79 42. Steinberg SJ, Wang SJ, Kim DG, Mihalik SJ, Watkins PA. Human very-long-chain acyl-CoA synthetase: Cloning, topography, and relevance to branched-chain fatty acid metabolism. Biochem Biophys Res Commun 1999;257:615–21 43. Jansen GA, Wanders RJA, Watkins PA, Mihalik SJ. PhytanoylCoenzyme A hydroxylase deficiency—The enzyme defect in Refsum’s disease. N Engl J Med 1997;337:133–34 44. Jansen GA, Ofman R, Ferdinandusse S, et al. Refsum disease is caused by mutations in the phytanoyl-CoA hydroxylase gene. Nat Genet 1997;17:190–93 45. Mihalik SJ, Morrell JC, Kim D, Sacksteder KA, Watkins PA, Gould SJ. Identification of PAHX, a Refsum disease gene. Nat Genet 1997;17:185–89 46. Jansen GA, Hogenhout EM, Ferdinandusse S, et al. Human phytanoyl-CoA hydroxylase: resolution of the gene structure and the molecular basis of Refsum’s disease. Hum Mol Genet 2000;9:1195– 1200 47. Heymans HSA, Oorthuys JW, Nelck G, Wanders RJA, Schutgens RBH. Rhizomelic chondrodysplasia punctata: Another peroxisomal disorder. N Engl J Med 1985;313:187–88 48. Jansen GA, Mihalik SJ, Watkins PA, et al. Phytanoyl-CoA hydroxylase is not only deficient in classical Refsum disease but also in rhizomelic chondrodysplasia punctata. J Inherit Metab Dis 1997; 20:444–46 49. Gould SJ, Valle D. Peroxisome biogenesis disorders: Genetics and cell biology. Trends Genet 2000;16:340–45
Downloaded from http://jnen.oxfordjournals.org/ by guest on January 23, 2017
12. Kuntzer T, Ochsner F, Schmid F, Regli F. Quantitative EMG analysis and longitudinal nerve conduction studies in a Refsum’s disease patient. Muscle Nerve 1993;16:857–63 13. Gibberd FB, Billimoria JD, Goldman JM, et al. Heredopathia atactica polyneuritiformis: Refsum’s disease. Acta Neurol Scand 1985; 72:1–17 14. Bergsmark J, Djupesland G. Heredopathia atactica polyneuritiformis (Refsum’s diseases). An audiological examination of two patients. Eur Neurol 1968;1:122–30 15. Refsum S. Heredopathia atactica polyneuritiformis. Phytanic acid storage disease (Refsum disease). In: Vinken PJ, Bruyn GW, de Jong JMB, eds. Handbook of clinical neurology. System disorders and atrophies. Amsterdam: North-Holland Publishing Co., 1975: 181–229 16. Leys D, Petit H, Bonte-Adnet C, et al. Refsum’s disease revealed by cardiac disorders. Lancet 1989;1:621 17. Posada Rodriguez IJ, Gutierrez-Rivas E, Cabello A. Cardiac involvement in neuromuscular diseases. Rev Esp Cardiol 1997;50: 882–901 18. Davies MG, Marks R, Dykes PJ, Reynolds D. Epidermal abnormalities in Refsum’s disease. Br J Dermatol 1977;97:401–6 19. Dykes PJ, Marks R, Davies MG, Reynolds DJ. Epidermal metabolism in heredopathia atactica polyneuritiformis (Refsum’s disease). J Invest Dermatol 1978;70:126–29 20. Refsum S, Stokke O. Refsum’s disease (heredopathia atactica polyneuritiformis). In: Gomez M, ed. Neurocutaneous disease-A practical approach. Boston: Butterworth, 1987:80–160 21. Reynolds DJ, Marks R, Davies MG, Dykes PJ. The fatty acid composition of skin and plasma lipids in Refsum’s disease. Clin Chim Acta 1978;90:171–77 22. Molzer B, Bernheimer H, Barolin GS, Ho¨finger E, Lenz H. Di-, mono- and nonphytanyl triglycerides in the serum: A sensitive parameter of the phytanic acid accumulation in Refsum’s disease. Clin Chim Acta 1979;91:133–40 23. Yao JK, Dyck PJ. Tissue distribution of phytanic acid and its analogues in a kinship with Refsum’s disease. Lipids 1987;22:69–75 24. Stoffel W, Kahlke W. The transformation of phytol into 3,7,11,15tetramethylhexadecanoic (phytanic) acid in heredopathia atactica polyneuritiformis (Refsum’s syndrome). Biochem Biophys Res Commun 1965;19:33–36 25. Steinberg D, Avigan J, Mize C, Eldjarn L, Try K, Refsum S. Conversion of U-C14-phytol to phytanic acid and its oxidation in heredopathia atactica polyneuritiformis. Biochem Biophys Res Commun 1965;19:783–89 26. Mize CE, Herndon JH, Jr., Blass JP, et al. Localization of the oxidative defect in phytanic acid degradation in patients with Refsum’s disease. J Clin Invest 1969;48:1033–40 27. Mize CE, Avigan J, Steinberg D, Pittman RC, Fales HM, Milne GWA. A major pathway for the mammalian oxidative degradation of phytanic acid. Biochim Biophys Acta 1969;176:720–39 28. Tsai SC, Avigan J, Steinberg D. Studies on the alpha oxidation of phytanic acid by rat liver mitochondria. J Biol Chem 1969;244: 2682–92 29. Tsai SC, Steinberg D, Avigan J, Fales HM. Studies on the stereospecificity of mitochondrial oxidation of phytanic acid and of -hydroxyphytanic acid. J Biol Chem 1973;248:1091–97 30. Poulos A, Sharp P, Whiting M. Infantile Refsum’s disease (phytanic acid storage disease): A variant of Zellweger’s syndrome? Clin Genet 1984;26:579–86 31. Poulos A, Sharp P, Fellenberg AJ, Danks DM. Cerebro-hepato-renal (Zellweger) syndrome, adrenoleukodystrophy, and Refsum’s disease: Plasma changes and skin fibroblast phytanic acid oxidase. Hum Genet 1985;70:172–77 32. Watkins PA, Howard AE, Mihalik SJ. Phytanic acid must be activated to phytanoyl-CoA prior to its alpha-oxidation in rat liver peroxisomes. Biochim Biophys Acta 1994;1214:288–94
REFSUM DISEASE 50. Wanders RJA. Peroxisomal disorders: Clinical, biochemical, and molecular aspects. Neurochem Res 1999;24:565–80 51. Wierzbicki AS, Mitchell J, Lambert-Hammill M, et al. Identification of genetic heterogeneity in Refsum’s disease. Eur J Hum Genet 2000;8:649–51 52. Braverman N, Steel G, Obie C, et al. Human PEX7 encodes the peroxisomal PTS2 receptor and is responsible for rhizomelic chondrodysplasia punctata. Nat Genet 1997;15:369–76 53. Motley AM, Hettema EH, Hogenhout EM, et al. Rhizomelic chondrodysplasia punctata is a peroxisomal protein targeting disease caused by a non-functional PTS2 receptor. Nat Genet 1997;15:377–80 54. Purdue PE, Zhang JW, Skoneczny M, Lazarow PB. Rhizomelic chondrodysplasia punctata is caused by deficiency of human PEX7, a homologue of the yeast PTS2 receptor. Nat Genet 1997;15:381–84 55. Ferdinandusse S, Denis S, Clayton PT, et al. Mutations in the gene encoding peroxisomal alpha-methylacyl-CoA racemase cause adultonset sensory motor neuropathy. Nat Genet 2000;24:188–91 56. Mukherji M, Kershaw NJ, MacKinnon CH, et al. ‘Chemical cosubstrate rescue’ of phytanoyl-CoA 20hydroxylase mutants causing Refsum’s Disease. Chem Commun 2001;972–73
1031
57. Kitareewan S, Burka LT, Tomer KB, et al. Phytol metabolites are circulating dietary factors that activate the nuclear receptor RXR. Mol Biol Cell 1996;7:1153–66 58. Lemberger T, Desvergne B, Wahli W. Peroxisome proliferator-activated receptors: A nuclear receptor signaling pathway in lipid physiology. Annu Rev Cell Dev Biol 1996;12:335–63 59. Ellinghaus P, Wolfrum C, Assmann G, Spener F, Seedorf U. Phytanic Acid Activates the Peroxisome Proliferator-activated Receptor alfa (PPARalfa) in Sterol Carrier Protein 2-/Sterol Carrier Protein x-deficient Mice. J Biol Chem 1999;274:2766–72 60. Zomer AWM, van der Burg B, Jansen GA, Wanders RJA, Poll-The BT, Van Der Saag PT. Pristanic acid and phytanic acid. Naturally occurring ligands for the nuclear receptor peroxisome proliferatoractivated receptor alpha. J Lipid Res 2000;41:1801–7 61. Seedorf U, Raabe M, Ellinghaus P, et al. Defective peroxisomal catabolism of branched fatty acyl coenzyme A in mice lacking the sterol carrier protein-2/sterol carrier protein-x gene function. Genes Dev 1998;12:1189–201
Downloaded from http://jnen.oxfordjournals.org/ by guest on January 23, 2017 J Neuropathol Exp Neurol, Vol 60, November, 2001