Payment Reform Quarterly Update February 2, 2015
Agenda I. Payment Reform Strategy I. APM Demonstration II. CP3 III.PCHH and 2703
2
Purpose & Structure •
CPCA 2014-17 Strategic Plan – Health System Transformation – Health Center Transformation – California Health+
•
•
Quarterly Webinars 4 x Year- in between board meetings Informed Members – leads to Engaged Members • Leads to Meaningful Work – leads to Major Outcomes!
3
CPCA Payment Reform Strategy
4
CPCA Payment Reform Strategy
5
Legislative Update • Legislation- Introduced – SB 147, Senator Hernandez – Co-Sponsors: CPCA, CAPH, LA Care • SPA – Spring/Summer 2015 • Rate development – Fall 2015 • Implementation- July 2016 through June 2019
6
APM Demonstration
7
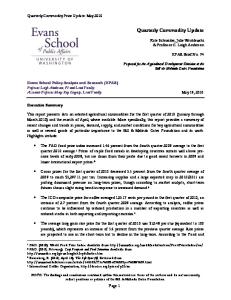
Today- PPS • DHCS sets rates for health plans • Plans pay primary care capitation to health centers • Health centers bill state a wraparound payment • Annual reconciliation
DHCS
Traditional Rate Setting
Health Plan
Primary care capitation
Wrap around payment
FFS for mental health
FQHC
8
Future- APM Demonstration • Conversion of PPS visit to PPS equivalent PMPM – 4 PMPM by aid category – Child/Adult/SPD/MCE • •
EXAMPLE: $100 PPS x 3.5 Avg Adult Visits = $350 $1350/ 12 member months = $29.16 PMPM
• 3 year demonstration with volunteer health centers • Abide by Federal APM– PPS is Floor • Health centers will continue to: – Have site-specific rates – Have ability to do scope change (with State) – Receive annual MEI increases (State to pass to plans)
• Plans will have risk corridor – At risk for max of .75% of wrap cap amount. State responsible for rest. – Can benefit up to .75% of wrap cap if FQHC had to pay back. State 9 would get rest.
Future- APM Demonstration Phased Reconciliation Triggers • Year 1 - Reconciliation would be triggered if traditional visits increased by more than 5% or decreased by more than 30% • 2 - Triggered by more than 5-7.5% or decreased by more than 30% • 3 – Triggered by more than 7.5-10% or decreased by more than 30% Description
– FQHCs would be at risk for 5/7.5/10% of visits and reconciled to PPS for anything above. – FQHCs would keep the margin up to 30% if visits 10 drop, and at 30% reconciliation would be triggered.
Future- APM Demonstration • DHCS sets rates for health plans • Monthly, plan would tell State how many Medi-cal members are assigned to FQHC in demonstration. • State would pay the plan an additional “Wrap Cap” for that site(s) • Wrap around payment becomes a capitation payment that is AID Category specific • Health center would receive 4 per member per month payments (Child, Adult, SPD, Expansion) • Reconciliation between FQHC and plan.
DHCS Wrap CapChild Adult SPD Expansion
Traditional Rate Setting
Health Plan
Primary care capitation
FFS for mental health
FQHC
Wrap CapChild Adult SPD Expansion
11
Future- APM Demonstration Benefits • Financial benefit if panel size increases • Flexibility to use the capitation to meet patient’s needs, improve quality, and be the provider of choice • PPS Rules Gone- billable providers/ same day visit/ groups / four walls – NO MORE! • Capitation is likely future – Demonstration is soft/protected launch • Active management and responsibility of assigned populations
12
Counties Phase 1
Phase 2
Alameda
Kings
Contra Costa
Orange
Humboldt
Riverside
Los Angeles
San Diego
Merced
Stanislaus
Monterey
Tulare
Napa
Yolo
San Mateo Santa Clara Solano
Phase 1 • 20 organizations • 16 nonprofit FQHCs • 4 public FQHCs • 62 sites • 30 nonprofit FQHCs • 32 public FQHCs • 10 counties
Phase 2 • 11 organizations • 10 nonprofit FQHCs • 1 public FQHC • 26 sites • 16 nonprofit FQHCs • 16 public FQHCs • 7 counties 13
PCHH “Patient Centered Health Home” can refer to either…
1. CPCA PCHH Initiative or 2. CA Health Homes for Patients with
Complex Needs (HHPCN)
14
PCHH- Review The California State Innovation Model + Section 2703 = CA Health Homes for Patients with Complex Needs (HHPCN) 15
PCHH- Review Section 2703 SPA • State Option to Provide Health Homes for Enrollees with Chronic Conditions as defined by each state • Funding for 2 years and requirement to demonstrate savings • 90% Federal/ 10% State funding • The California Endowment contributing California’s 10% • States can have more than one SPA • No deadline
16
PCHH- Review What can Section 2703 fund? • • • • • •
Comprehensive care management Care coordination Health promotion Comprehensive transitional care & follow-up Patient and family support Referral to community and social support services
…basically, services not already funded by Medicaid
17
PCHH Updates CalSIM Updates • California was NOT selected for a Round Two Model Test Award • 11 States selected • California WAS selected for a Round Two Model Design Award • $3 million to “design or further refine their plans” and resubmit to CMS within 12 mos 18
PCHH Updates 2703 Updates • Concept paper released November • HHPCN will target all three categories for health home eligibility with an emphasis on high-cost, high-risk, high-utilizers • 2 or more chronic conditions • 1 condition and at risk of a second • Serious mental illness (SMI) 19
PCHH Updates
20
PCHH Updates • Eligibility criteria developed by DHCS • Eligibility determination run by DHCS or health plans • Providers may be able to refer patients • Patients able to opt-out • Medicaid expansion will be included • Medical acuity = tiered service and payments • Chronically homeless enrollees will have additional care management reqs 21
PCHH Updates
22
PCHH Next Steps • DHCS communication to CPCA that 2703 implementation is moving forward • Uncertainty whether CA will pursue reapplication for SIM grant • 1115 Waiver proposition (JSI) – include TA and training so 2703 not dependent on CalSIM • CPCA working with TCE, JSI, CAPH on next steps for 2703 23
P4P & Shared Savings IHA Update • Medi-Cal P4P Southern CA Pilot – Completed Fall 2014 – Proposed next steps include expansion of reporting at the clinic level – Finding: Provider Orgs w/ Commercial P4P experience performed better
24
P4P & Shared Savings IHA Update • Statewide P4P Survey – Preliminary Results – Survey 20/22 CA Medi-Cal Managed Care Plans – 16/22 plans offer some level of incentive plan – CPCA conducting parallel survey of providers
• IHA summary results here: http://www.iha.org/grants-projects-safety-netperformance-measurement.html 25
P4P & Shared Savings 1115 Waiver MCO/Provider Incentive Workgroup – Several models reviewed • P4P • Shared Savings (state to plan & plan to providers) & (plan to county behavioral health) • State also considering changes to the rate setting – –
No longer penalize efficiency Move some administrative costs to medical expense (Care coordination) 26
P4P & Shared Savings
CCHC Innovation: APM and CP3
Value Based Payment System Primary Care Transformation: CMS TCPI CalHIPSO Funding Opportunity
1115 Waiver – Medi-Cal Payers 27
Contact Andie Patterson Director of Government Affairs
[email protected] re: APM
Samantha Jones Assistant Director of Programs
[email protected] re: P4P Erynne Jones Associate Director of Policy
[email protected] re: PCHH 28