Original Articles
Neuronal Hypertrophy in Acute Appendicitis Shigang Xiong, MD; Prem Puri, MS, FRCS(Ed), FACS; Laszlo Nemeth, MD; D. Sean O’Briain, MB, MRCPath; Denis J. Reen, MSc, PhD
● Objective.—The pathogenesis of appendicitis remains poorly understood. However, there is increasing evidence of involvement of the enteric nervous system in immune regulation and in inflammatory responses. This study was set up to characterize the status of the enteric nervous system in normal and in inflamed appendixes. Methods.—S100– and 29,29-cyclic nucleotide 39 phosphodiesterase–positive Schwann cells, synaptophysin, and neuron-specific, enolase-positive nerve fibers and tryptasepositive mast cells were evaluated with immunohistochemical staining in surgically resected appendixes from 20 children with histologically proven acute appendicitis (HA), 10 histologically normal appendixes (HN) from patients with a clinical diagnosis of appendicitis, and 10 normal appendixes from patients undergoing elective abdominal surgery. Immunostained sections were subjected to quantitative image analysis. The number and size of ganglia and the number of nerve fibers, Schwann cells, and mast cells in each tissue compartment was quantitatively or semiquantitatively measured. Results.—Increased numbers of fibers, Schwann cells, and enlarged ganglia, widely distributed in the muscularis
externa and submucosa, were seen in all HA appendixes and in 4 of 10 HN appendixes. The number and size of ganglia in muscularis externa and in the submucosa of appendixes with HA were significantly greater compared with those in control appendixes (P , .001). A significantly increased number of individually stained nerve fibers and Schwann cells (P , .05) were present in the muscularis externa in HA appendixes compared with control appendixes. Significantly increased numbers of tryptase-positive mast cells (P , .05) were present in the submucosa, muscularis, and especially in the lamina propria in HA specimens, compared with that of control tissue. Conclusions.—The significant increase in neural components and mast cells in acute appendicitis is unlikely to develop during a single acute inflammatory episode. This suggests an underlying chronic abnormality as a secondary reaction to repeated bouts of inflammation, obstruction, or both. These results challenge our current understanding of the pathophysiological processes that give rise to acute appendicitis. (Arch Pathol Lab Med. 2000;124:1429–1433)
T
and mast cells. It is also suggested by the presence of receptors for neuropeptides on immunocompetent cells throughout the gastrointestinal tract.4–6 Increased proliferation of nerves, as well as increased levels of neurotransmitters such as substance P4–7 and vasoactive intestinal peptide,5 has been reported in association with chronic inflammatory bowel disease6–9 and in appendiceal fibrosis, in which the fibrotic lesion frequently contains more Schwann cells and mast cells than fibroblasts.10 This study was set up to investigate the status of the enteric nervous system in appendicitis.
he function of the human appendix remains obscure. However, appendicitis continues to challenge us, with 6% to 20% of the general population developing appendicitis during their lifetime and about 1 in every 6 people undergoing appendectomy.1 The exact etiology and pathogenesis of appendicitis are poorly understood. Although obstruction of the appendiceal lumen, which results in distension and interference with circulation, has been suggested to be a major factor, invasion of the appendix wall by microorganisms is considered to be the last event in the pathogenesis of acute appendicitis.2 There is increasing evidence of interactions between the nervous and the immune systems in various organs,3,4 and perhaps nowhere in the body is it more apparent and important than in the intestine, about which there are considerable data supporting the involvement of the enteric nervous system in immune regulation.4–7 The involvement of the enteric nervous system is suggested from the close spatial and functional relationship that exists between nerves and immunocompetent cells such as lymphocytes4–6 Accepted for publication April 11, 2000. From the Children’s Research Centre, Our Lady’s Hospital for Sick Children, Crumlin, Dublin 12, Ireland. Reprints: Prem Puri, MS, FRCS(Ed), FACS, Director of Research, Children’s Research Centre, Our Lady’s Hospital for Sick Children, Crumlin, Dublin 12, Ireland (e-mail:
[email protected]). Arch Pathol Lab Med—Vol 124, October 2000
METHODS Subjects and Specimens Between January 1995 and July 1996, 271 consecutive patients with a clinical diagnosis of appendicitis underwent emergency appendicectomy at Our Lady’s Hospital for Sick Children, Dublin, Ireland. Appendix specimens obtained at surgery were fixed in formalin, divided into 3 segments from tip to base, and embedded in paraffin. Two hundred twenty appendixes were classified as histologically acute, gangrenous, or perforated; 1 appendix was classified as carcinoid tumor; and 50 appendixes were classified as histologically normal. Twenty appendixes (15 from boys and 5 from girls; mean age, 8.6 6 6 years) were randomly selected from the group of histologically proven acute appendicitis (HA). Ten appendixes (3 from boys, 7 from girls; mean age, 9.6 6 2.1 years) were randomly selected from the group of appendixes classified as histologically normal (HN). Ten normal apNeuronal Hypertrophy in Acute Appendicitis—Xiong et al 1429
Table 1. Details of Primary Antibodies Used Antibody
Cell Specificity
Raised In
Dilution
Source
S100 protein CNPase* Synaptophysin Neuron-specific enolase Mast cell tryptase * 29,29-cyclic nucleotide 39 phosphodiesterase.
Schwann cells Schwann cells Neuron Neuron Mast cells
Rabbit Mouse Rabbit Mouse Mouse
1:200 1:100 1:50 1:50 1:50
Dako Sigma Dako Dako Dako
pendixes removed from children (4 from boys, 6 from girls; mean age, 9.1 6 2.6 years) undergoing elective abdominal surgery (fundoplication for gastroesophageal reflux) were used as controls. Sections were cut at 5 mm and stained with routine hematoxylin and eosin stain and by immunohistochemistry. Gangrenous and perforated appendixes were not included in this study because of major structural damage to the lamina propria and submucosal tissue that made analysis impractical.
Immunohistochemistry After the tissue sections were removed from paraffin and rehydrated, they were treated in a microwave, digested proteolytically, and incubated with normal serum from the species in which the second antibody was raised. The Schwann cell markers, S100 protein, and 2929-cyclic nucleotide 39 phosphodiesterase (CNPase), the neuronal markers synaptophysin, neuron-specific enolase (NSE), and mast cell tryptase expression, was determined by incubation overnight at 48C with commercially available primary antibody, followed by incubation with appropriate biotinylated secondary antibody (Dako, Glostrup, Denmark) and strepABCcomplex or ABCcomplex (Dako), prepared according to the manufacturer’s instructions. Tissue-section staining was developed with nitroblue tetrazolium/BCIP (5-bromo-4-chloro-3indolyl-phosphate) (Sigma) or diaminobenzidine (Dako) to give a blue-purple or brown reaction product. Negative controls consisted of tissue sections incubated with normal rabbit or mouse serum used in place of the primary antibody. The primary antibodies we used are described in Table 1.
Image Analysis Immunostained sections were subjected to quantitative microscopic measurement with an IPS1.02 Image Analysis System and Integrating software (Alcatel, Grenoble, France). The number and size of ganglia was expressed as the number per square millimeter of tissue, and the mean size of each ganglion was expressed as square yoctometer per ganglion. The number of mast cells was determined by counting within an area of 1 by 1 mm2 with a graduated eyepiece graticule at 3400 magnification. For each sample, a total of 10 serial squares were evaluated in each field within each tissue compartment. Ten nonoverlapping fields were scanned, and the number of positive cells were expressed as the number per square millimeter of tissue.
Statistical Analysis Statistical tests for significant differences in the number of stained cells and size and number of ganglia between the 2 patient groups and the controls were carried out by analysis of variance at a significance level of P , .05.
RESULTS Histopathologic Findings An extensive neutrophil infiltrate extending throughout the submucosa and into the muscularis externa was seen in all HA specimens. On hematoxylin and eosin staining, ganglia appeared to be more prominent in HA, and to a lesser extent in HN, appendixes compared with controls. Ganglia were found not only between the circular and longitudinal muscle layers but also deep within the muscle layers in all 3 groups of samples. 1430 Arch Pathol Lab Med—Vol 124, October 2000
Neural Components in HA and HN Appendixes Both synaptophysin and NSE stained nerve fibers and S100- and CNPase-immunopositive Schwann cells showed a similar distribution pattern in all the tissue specimens we examined. A large number of nerve fibers and Schwann cells were observed widely distributed throughout the submucosa and the muscularis externa, especially in the circular muscle layers, of HA appendixes (Figures 1, A and 2, A). The number and size of ganglia in the muscularis externa and the submucosa were significantly greater (P , .001; Table 2; Figures 1, A, 2, A, and 3) than in control tissues. In the lamina propria of HA appendixes, fine nerve fibers were prominent, especially near the epithelial surface. Large nerve fiber clusters were sometimes found near the bottom of crypts and between crypts. Many thick nerve bundles were also observed in the serosa. Only a few sparsely distributed immunostained nerve fibers and Schwann cells were seen in control specimens (Figures 1, B and 2, B). Four of 10 HN appendixes displayed increased nerve fibers and Schwann cell number and ganglion size, which was identical to that seen in HA appendixes, whereas the remaining 6 were similar to control tissue in terms of the neuronal components. Mast Cells in HA and HN Appendixes Staining with tryptase indicated the presence of mast cells in all tissue layers in the 3 groups studied. In the HA appendix tissue samples, significantly increased numbers of mast cells were seen in the lamina propria (P , .05) compared with those in the control group (Figures 4, A and B, and 5). In the lamina propria of the HA appendixes, mast cells were frequently clustered close to the epithelium. The lymphoid follicles were negative. There was an increased number of mast cells in HN appendixes compared with the control group, but the increase did not reach statistical significance. DISCUSSION Peripheral nerve tissue under physiological conditions is generally considered to be stable with regard to proliferation and regeneration. Although increased neuronal components and peptidergic neurotransmitters have been reported in association with inflammatory bowel diseases such as ulcerative colitis6,8,9 and Crohn disease,6 there are no reports of altered neural expression in association with acute inflammatory conditions. The surprising finding in this study—of significantly increased numbers of synaptophysin and NSE stained nerve fibers and S100- and CNPase-positive Schwann cells in the acutely inflamed appendix specimens—challenges our understanding of the pathophysiological processes that give rise to acute appendicitis. The pathophysiological basis for this neuronal hypertrophy in acute appendicitis is not known. It has previously Neuronal Hypertrophy in Acute Appendicitis—Xiong et al
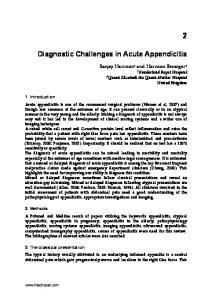
Figure 1. S100 immunohistochemical staining of (A) histologically proven acute appendicitis (HA) and (B) normal appendixes. Significantly increased numbers of S100-immunopositive Schwann cells and ganglia and enlarged ganglia were seen in the muscularis externa (M) and submucosa (S) in HA appendixes. Figure 2. Synaptophysin immunohistochemical staining of (A) histologically proven acute appendicitis (HA) and (B) normal appendixes. Significantly increased numbers of synaptophysin-stained nerve fibers and ganglia and enlarged ganglia are seen in the muscularis externa (M) and submucosa (S) in HA appendixes.
Table 2. Schwann Cells and Ganglia in the Muscularis Externa and Submucosa of HA and Normal Appendices* Variable
HA (n 5 20) Number of Schwann cells, /mm2 Number of ganglia, /mm2 Area of ganglia, m2/ganglion Control (n 5 10) Number of Schwann cells, /mm2 Number of ganglia, /mm2 Area of ganglia, mm2/ganglion * HA indicates histologically proven acute appendicitis. † P , .001.
been suggested that neuronal proliferation in association with appendiceal fibrosis represents a physiological aging phenomenon.11 This theory, however, does not explain the observed neuronal hypertrophy in this study, because all our patients were children with no evidence of appendiceal fibrosis. Furthermore, it does not explain why there is no appendiceal obliteration in up to 50% of patients older than 70 years.12 Arch Pathol Lab Med—Vol 124, October 2000
Submucosa
Muscularis
23.0 6 7.9† 1.6 6 0.5† 682.3 6 100.3†
61.7 6 21.9† 3.9 6 0.9† 672.6 6 47.8
5.2 6 0.3 0.8 6 0.3 160.7 6 34.2
6.9 6 2.5 1.6 6 0.7 269.0 6 25.9
Several studies have shown that inflammation can effect or affect nerve remodeling. Extensive sprouting of neurofilament-immunoreactive nerve fibers has been observed 1 to 2 weeks after a superficial skin wound in patients.13 Dental periapical inflammation, pulpectomy, and pulpal neurosis may result in the formation of a disorganized sprouting and branching of axons.14 The density of peptidergic nerve fibers has been shown to be directly Neuronal Hypertrophy in Acute Appendicitis—Xiong et al 1431
Figure 3. Ganglion size in muscularis externa in tissue from appendixes with histologically proven acute appendicitis (HA), histologically normal appendixes (HN), and control appendixes. * P . .05. ** P , .001.
proportional to the histological level of severity of inflammatory bowel disease, where only areas with severe inflammation have been shown to have increased numbers of substance P and vasoactive intestinal peptide immunoreactive nerve fibers.8,9 Analysis of these data suggests that peripheral nerves may physiologically be in a constant state of modeling under different situations and that a variety of stimuli, such as inflammation or injury, can effect or affect nerve remodeling. Neural proliferation may therefore represent a form of inflammatory response. Welldeveloped neuronal changes of the extent seen in this study are unlikely to develop during a single episode of acute inflammation (frequently bouts of only hours or days in duration) and suggest a preexisting stimulus such as repeated episodes of subclinical inflammation or a response to an obstruction. Mast cells, typically located in
Figure 5. Mast cell density in lamina propria in appendixes with histologically proven acute appendicitis (HA), histologically normal appendixes (HN), and control appendixes. * P . .05. ** P , .05.
close association with tissue that form barriers such as the skin, mucosa, and submucosa of the gastrointestinal and respiratory tract, exert their biological effects by releasing preformed mediators stored in granules such as leukotrienes, prostaglandins, and cytokines.15 There is considerable evidence that mast cells are microanatomically and functionally appeased to the peripheral nerves,10,16 resulting in a homeostatic unit in the regulation of gut physiology and host defense. Nerve growth factor has been shown to increase the number of human mast cell colonies17 and prevent apoptosis of rat peritoneal mast cells through the trk proto-oncogene receptor.18 Nerve growth factor not only promotes colony formation of murine interleukin 3–dependent bone marrow–derived cultured mast cells but also induces phenotypic change from bone marrow–derived cultured mast cells to connective tissue– type mast cells.19 Changes in density of mast cells and content of mast cell–released mediators in mucosa and submucosa are a feature of Crohn disease and ulcerative
Figure 4. Tryptase immunohistochemical staining of (A) appendixes with histologically proven acute appendicitis (HA) and (B) normal appendixes. M indicates muscularis externa; S, submucosa; and L, lamina propria. Significantly increased numbers of tryptase-stained mast cells are seen in the lamina propria in HA appendixes. 1432 Arch Pathol Lab Med—Vol 124, October 2000
Neuronal Hypertrophy in Acute Appendicitis—Xiong et al
colitis.20,21 It is not clear how quickly mast cell numbers can increase. The increase in mast cells in acute appendicitis, together with the broad spectrum of activities of mast cell–derived mediators, suggests that this cell type could play a role in the pathogenesis of acute appendicitis, although the exact mechanism remains to be elucidated. It has always been of clinical concern that up to one third of appendixes removed at surgery for suspected appendicitis are subsequently classified as normal by conventional histological staining.22 The discrepancy between clinical presentation and the lack of definitive histopathological support is confounding. We have previously shown23 that in clinically suspected appendicitis, elevated levels of tumor necrosis factor a and interleukin 2 in 22% of appendixes described as HN. A similar phenomenon is suggested by the present study, which has demonstrated increased numbers of nerve fibers, Schwann cells, ganglia, and mast cells in 4 of 10 histologically normal appendixes of a degree, similar to that seen in acute appendicitis. The neuronal hypertrophy in these HN appendixes probably reflects a level of inflammatory response similar to previously described neuronal hypertrophy in association with chronic inflammatory bowel disease.8 The significant increase in neural components and mast cells, together with their extensive distribution in acute appendicitis, suggests a functional link between the enteric nervous system, mast cells, and the pathogenesis of acute appendicitis, although the exact mechanism remains to be elucidated. The neuronal cell hypertrophy observed in this study may represent the reparative phase of an inflammatory process to previous chronic or repeated acute injury to stimuli. The usual histological features of chronic inflammation would, if present in the appendix, be largely obscured by the inherent lymphoid tissue present. Neuronal hypertrophy may represent the most early identifiable morphological characteristic of such inflammation. Therefore, it seems reasonable to question whether acute appendicitis represents a single episode of acute inflammation in the appendix. We consider it more appropriate to suggest that acute appendicitis may represent an exacerbation of an inflammatory process that already exists in the appendix, because to achieve the proliferation of nerve cells and nerve fiber extension observed, the tissue must undergo a series of molecular and cellular events over time.24 The findings of a significant increase in synaptophysin-, NSE-, S100-, and CNPase-immunopositive neuronal components in a substantial proportion of socalled negative appendectomies further supports this hypothesis.
Arch Pathol Lab Med—Vol 124, October 2000
References 1. Jess P, Bjerregaard B, Brynitz S, Holst-Christensen J, Kalaja E, Lund- Kristensen J. Acute appendicitis. Prospective trial concerning diagnostic accuracy and complications. Am J Surg.141:232–234. 2. Zern JT. The appendix: little organ, big trouble. Del Med J. 1995;67:326– 334. 3. Novotny GE, Heuer T, Schottelndreier A, Fleisgarten C. Plasticity of innervation of the medulla of axillary lymph nodes in the rat after antigenic stimulation. Anat Rec 1994;238:213–224. 4. Pascual DW, Beagley KW, Kiyono H, McGhee JR. Substance P promotes Peyer’s patch and splenic B-cell differentiation. Adv Exp Med Biol. 1995;371A: 55–59. 5. Goettxl EJ, Xia M, Ingram DA, et al. Neuropeptide signalling of lymphocytes in immunological responses. Int Arch Allergy Immunol. 1995;170:202–204. 6. Mantyh CR, Vigna SR, Bollinger RR, Mantyh PW, Maggio JE, Pappas TN. Differential expression of substance P receptors in patients with Crohn’s disease and ulcerative colitis. Gastroenterology. 1995;109:850–860. 7. Swain MG, Agro A, Blennerhasset P, Stanisz A, Collins SM. Increased levels of substance P in the myeteric plexus of Trichinella-infected rats. Gastroenterology. 1992;102:1913–1919. 8. Keranen U, Jarvines H, Karkkainen P, Kiniluoto T, Kivilaakso E, Soinila S. Substance P—an underlying factor for pouchitis? Prospective study of substance P– and vasoactive intestinal polypeptide–immunoreactive innervation and mast cells. Dig Dis Sci. 1996;41:1665–1671. 9. Todorovic V, Janic B, Koko V, et al. Colonic vasoactive intestinal polypeptide (VIP) in ulcerative colitis—a radioimmunoassay and immunohistochemical study. Hepatogastroenterology. 1996;43:483–488. 10. Stead RH, Franks AJ, Goldsmith CH, Bienenstock J, Dixon MF. Mast cells, nerves and fibrosis in the appendix a morphological assessment. J Pathol. 1990; 161:209–219. 11. Therkelsen F. On histological diagnosis of appendicitis. Acta Chir Scand. 1946;94:1–48. 12. Muler S. Macroscopic changes in so-called ‘‘chronic’’ appendicitis. Acta Chir Scand. 1959;118:146–154. 13. Hermanson A, Dalsgaard CJ, Bjorklund H, Lindholm U. Sensory reinnervation and sensibility after superficial skin wounds in human patients. Neurosci Lett. 1987;74:377–382. 14. Holland GR. Periapical neural changes after pulpectomy. Oral Surg Oral Med Oral Pathol Oral Radiol Endod. 1995;80:726–734. 15. Galli SJ, Gordon JR, Wershil BK. Mast cell cytokines in allergy and inflammation. Agents Actions. 1993;43(suppl):209–220. 16. Dvorak AM, McLeod RS, Onderdonk AB, et al. Human gut mucosal mast cells ultrastructural observations and anatomic variation in mast cell nerve association in vivo. Int Arch Allergy Immunol. 1992;98:158–168. 17. Matsuda H, Coughlin MD, Bienenstock J, Denburg JA. Nerve growth factor promotes human hemopoietic colony growth and differentiation. Proc Natl Acad Sci U S A. 1988;85:6508–6512. 18. Kawamoto K, Okada T, Kannan Y, Ushio H, Matsumoto M, Matsuda H. Nerve growth factor prevents apoptosis of rat peritoneal mast cells through the trk proto-oncogene receptor. Blood. 1995;86:4638–4644. 19. Matsuda H, Kannan Y, Ushio H, et al. Nerve growth factor induces development of connective tissue–type mast cells in vitro from murine bone marrow cells. J Exp Med. 1991;174:7–14. 20. Fox CC, Lichtenstein LM, Roche JK. Intestinal mast cell response in idiopathologic inflammatory bowel disease. Histamine release from human intestinal mast cell in response to gut epithelial proteins. Dig Dis Sci. 1993;38:1105– 1112. 21. Dvorak AM, McLeod RS, Onderdonk A, et al. Ultrastructural evidence for Piecemeal and anaphylactic degranulation of human gut mucosal mast cells in vivo. Int Arch Allergy Immunol. 1992;99:74–83. 22. Pieper R, Kager L, Nasman P. Acute appendicitis: a clinical study of 1081 cases of emergency appendectomy. Acta Chir Scand. 1982;148:51–62. 23. Wang Y, Reen DJ, Puri P. Is a histologically normal appendix following emergency appendectomy always normal? Lancet. 1996;347:1076–1079. 24. Stead RH. Nerve remodelling during intestinal inflammation. Ann N Y Acad Sci. 1992;664:443–455.
Neuronal Hypertrophy in Acute Appendicitis—Xiong et al 1433