Natriuretic Peptide–driven Fluid Management during Ventilator Weaning A Randomized Controlled Trial Armand Mekontso Dessap1,2,3, Ferran Roche-Campo1,4, Achille Kouatchet5, Vinko Tomicic6, Gaetan Beduneau7, Romain Sonneville8, Belen Cabello4, Samir Jaber9, Elie Azoulay10, Diego Castanares-Zapatero11, Jerome Devaquet12, Franc¸ois Lellouche13, Sandrine Katsahian14, and Laurent Brochard1,2,3,15 1 ˆ pitaux de Paris (AP-HP), Centre Hospitalier Universitaire (CHU) Henri Mondor, Service de Re´animation Me´dicale, Cre´teil, Assistance Publique-Ho France; 2Universite´ Paris Est Cre´teil, Faculte´ de Me´decine, Cre´teil, France; 3Institut National de la Sante´ et de la Recherche Me´dicale (INSERM), Unite´ U955, Cre´teil, France; 4Hospital de Sant Pau, Servei de Medicina Intensiva, Barcelona, Spain; 5CHU d’Angers, Service de Re´animation Me´dicale, Angers, France; 6Clinica Alemana, Departamento de Paciente Crı´tico, Santiago de Chile, Chile; 7CHU de Rouen, Service de Re´animation Me´dicale and Unite´ Propre de Recherche et de l’Enseignement Supe´rieur, Equipe d’Accueil (UPRES-EA) 3830, Rouen, France; 8AP-HP, CHU Bichat-Claude Bernard, Service de Re´animation Me´dicale et des Maladies Infectieuses, Universite´ Paris Diderot, Sorbonne Paris Cite´, Paris, France; 9CHU Saint Eloi, De´partement d’Anesthe´sie Re´animation B, INSERM U1046, Montpellier, France; 10AP-HP, CHU Saint Louis, Service de Re´animation Me´dicale, Paris, ˆ pital Universitaire Saint-Luc, Service de Soins Intensifs, Bruxelles, Belgium; 12Ho ˆ pital Foch, Service de Re´animation, Suresnes, France; France; 11Ho 13 Institut Universitaire de Cardiologie et de Pneumologie de Que´bec, Que´bec, Canada; 14AP-HP, CHU Henri Mondor, Unite´ de Recherche Clinique, Cre´teil, France; and 15Intensive Care Division, University Hospital of Geneva, University of Geneva, Geneva, Switzerland
Rationale: Difficult weaning from mechanical ventilation is often associated with fluid overload. B-type natriuretic peptide (BNP) has been proposed as a tool for predicting and detecting weaning failure of cardiovascular origin. Objectives: To investigate whether fluid management guided by daily BNP plasma concentrations improves weaning outcomes compared with empirical therapy dictated by clinical acumen. Methods: In a randomized controlled multicenter study, we allocated 304 patients to either a BNP-driven or physician-driven strategy of fluid management during ventilator weaning. To standardize the weaning process, patients in both groups were ventilated with an automatic computer-driven weaning system. The primary end point was time to successful extubation. Measurements and Main Results: In the BNP-driven group, furosemide and acetazolamide were given more often and in higher doses than in the control group, resulting in a more negative median (interquartile range) fluid balance during weaning (–2,320 [–4,735, 738] vs. -180 [–2,556, 2,832] ml; P , 0.0001). Time to successful extubation was significantly shorter with the BNP-driven strategy (58.6 [23.3, 139.8] vs. 42.4 [20.8, 107.5] h; P ¼ 0.034). The BNP-driven strategy increased the number of ventilator-free days but did not change length of stay or mortality. The effect on weaning time was strongest in patients with left ventricular systolic dysfunction. The two strategies did not differ significantly regarding electrolyte imbalance, renal failure, or shock. (Received in original form May 26, 2012; accepted in final form September 10, 2012) Supported and promoted by the French publicly funded hospital clinical research program (Program Hospitalier de Recherche Clinique). Biosite France supplied the BNP assay devices and kits (Triage MeterPlus) for the study. Dra¨ger Medical provided the AWS-equipped ventilators for the study. Author Contributions: A.M.D., F.L., and L.B. conceived and designed the study; A.M.D., F.R.-C., A.K., V.T., G.B., R.S., B.C., S.J., E.A., D.C.-Z., and J.D. recruited patients and collected data; S.K., A.M.D., and L.B. contributed to data analysis and interpretation; A.M.D., S.K., and L.B. drafted the report; all authors contributed to review and revision of the report, and all authors have seen and approved the final version. Correspondence and requests for reprints should be addressed to Armand Mekontso Dessap, M.D., Ph.D., Service de Re´animation Me´dicale, Centre HospitaloUniversitaire Henri Mondor, 51, avenue du Mal de Lattre de Tassigny, 94010 Cre´teil Cedex, France. E-mail:
[email protected] This article has an online supplement, which is available from this issue’s table of contents at www.atsjournals.org Am J Respir Crit Care Med Vol 186, Iss. 12, pp 1256–1263, Dec 15, 2012 Copyright ª 2012 by the American Thoracic Society Originally Published in Press as DOI: 10.1164/rccm.201205-0939OC on September 20, 2012 Internet address: www.atsjournals.org
AT A GLANCE COMMENTARY Scientific Knowledge on the Subject
Fluid overload is associated with difficult weaning. Studies have demonstrated the usefulness of natriuretic peptides for predicting and diagnosing weaning failure of cardiac origin, which is a common cause of ventilation prolongation. What This Study Adds to the Field
Our study is the first trial of fluid management during weaning from mechanical ventilation. We show that a simple B-type natriuretic peptide–guided fluid management strategy is associated with increased diuretic use, a more negative fluid balance, and a shorter duration of mechanical ventilation, especially in patients with left ventricular systolic dysfunction.
Conclusions: Our results suggest that a BNP-driven fluid management strategy decreases the duration of weaning without increasing adverse events, especially in patients with left ventricular systolic dysfunction. Clinical trial registered with www.clinicaltrials.gov (NCT00473148). Keywords: mechanical ventilation; B-type natriuretic peptide; diuretics
Mechanical ventilation may give rise to complications, the incidence of which increases with the duration of respiratory support (1). The purpose of the weaning procedure is to minimize the duration of mechanical ventilation without incurring a substantial risk of failure. As weaning contributes at least 40% of the total duration of mechanical ventilation, optimizing this process is the main means of shortening the duration of mechanical ventilation (2). Numerous reports suggest that outcomes of mechanically ventilated patients in the intensive care unit (ICU) may be improved by decreasing the pulmonary capillary wedge pressure and/or minimizing a positive fluid balance at the time of weaning (3–6). Considerable attention has been paid to weaning failure due to fluid overload or heart failure (7–10). It has been shown that fluid overload can lead to weaning failure of cardiac origin (8, 11). B-type natriuretic peptide (BNP) is a cardiac biomarker secreted by the ventricular cardiomyocytes in response to increased wall stress. BNP levels before weaning independently
Mekontso Dessap, Roche-Campo, Kouatchet, et al.: BNP for Fluid Management during Ventilator Weaning
predict weaning failure (12). Studies have demonstrated the usefulness of natriuretic peptides for predicting and diagnosing weaning failure of cardiac origin (13, 14). We therefore hypothesized that, during the weaning period, fluid management guided by daily BNP plasma concentrations would improve outcomes compared with empirical therapy dictated by clinical acumen. We tested this hypothesis in the present international, multicenter, randomized controlled trial. To standardize the weaning process, all patients were ventilated using a computer-driven automated weaning system (AWS) (Evita Smart Care system; Drager Medical, Lubeck, Germany) (15). This work has been reported previously in abstract form (16).
METHODS Supplemental information on patients and methods is provided in the online supplement.
Patients Patients admitted to the participating ICUs were screened daily to assess whether they met the inclusion and noninclusion criteria. Inclusion criteria were endotracheal mechanical ventilation for at least 24 hours, SpO2 (arterial oxygen saturation as determined by pulse oximetry) at least 90% with fraction of inspired oxygen (FIO2) not more than 50% and positive end-expiratory pressure (PEEP) not more than 8 cm H2O; hemodynamic stability without vasopressor therapy or fluid bolus (rapid infusion of at least 500 ml of colloids or 1,000 ml of crystalloids) during the past 12 hours (with dopamine < 10 mg/kg/min and dobutamine < 10 mg/kg/min being allowed); sedation stopped or decreased over the past 48 hours (analgesia possibly continued); stable neurological status with Ramsay score not more than 5; body temperature greater than 36.08 C and less than 39.08 C; and informed consent signed by the patient or a close relative. Permanent noninclusion criteria were pregnancy or lactation, age less than 18 years, known allergy to furosemide or sulfonamides, tracheostomy on inclusion,
1257
hepatic encephalopathy, cerebral edema, acute hydrocephalus, myasthenia gravis, acute idiopathic polyradiculoneuropathy, decision to withdraw life support, and prolonged cardiac arrest with a poor neurological prognosis. Temporary noninclusion criteria were extubation scheduled on the same day (patients having already succeeded in a spontaneous breathing trial), persistent acute right ventricular failure, renal insufficiency (defined as any of the following: need for renal replacement therapy, plasma urea . 25 mmol/L, plasma creatinine . 180 mmol/L, creatinine clearance , 30 ml/min, greater than 25% increase in plasma creatinine over the past 24 h), injection of iodinated contrast agent in the past 6 hours, blood sodium greater than 150 mEq/L, blood potassium less than 3.5 mEq/L, or metabolic alkalosis with arterial pH greater than 7.50. When inclusion was delayed because of a temporary noninclusion criterion, enrollment could be performed after correction of the abnormal value.
Study Protocol Patients ventilated in volume-assist or pressure-control mode were eligible for inclusion only if a pressure-support (PS) test was positive. The PS test consisted in changing the ventilator mode to PS, without changing FIO2 or PEEP, as previously described (15) (see the online supplement). In patients already ventilated with PS at the time of inclusion, the positivity criteria of the PS test were checked. The protocol did not require performing a spontaneous breathing trial before enrollment. Only the PS test was asked.
Randomization and Masking Patients fulfilling the inclusion and noninclusion criteria and having a positive PS test were ventilated using the AWS, starting with PS and PEEP levels similar to those used during the PS test. Patients were then immediately assigned to one of two groups (BNP-guided fluid management or usual care based on clinical acumen) via independent Web-based centralized block randomization (available 24 h/d, 7 d/wk), with stratification on the center and underlying disease. Three subgroups
Figure 1. Study flowchart. BNP ¼ B-type natriuretic peptide; FIO2 ¼ fraction of inspired oxygen; PEEP ¼ positive end-expiratory pressure.
1258
AMERICAN JOURNAL OF RESPIRATORY AND CRITICAL CARE MEDICINE
were predefined for stratification: (1) presence of known chronic obstructive pulmonary disease (COPD), (2) presence of known left ventricular systolic dysfunction (LVD, ejection fraction , 45%), and (3) absence of both disorders. Patients with both disorders were classified in the COPD subgroup. The main purpose of stratification was to ensure a homogeneous distribution of COPD and LVD in the two arms. Careful attention was paid to minimizing changes in diuretic therapy practices caused by the research protocol during weaning in the control group. All randomized patients were ventilated using the AWS during weaning and monitored until discharge from the hospital or Day 60 after randomization.
B-Type Natriuretic Peptide Assay A blood sample was collected each morning for a BNP assay in all randomized patients during the weaning phase (while ventilated using the AWS). BNP was assayed using a rapid immunofluorescence test and a bedside measuring device (Triage BNP test; Biosite, Jouy-en-Josas, France; see the online supplement). Two devices were supplied per center: the first, which was used in the BNP-guided group, displayed the BNP result; the second did not show the result in visual display or print form and was used in the control group.
2012
Fluid and Electrolyte Management In the control group, the clinicians were blinded to the BNP assay results, and all treatments, including diuretics, were performed according to usual care, with no explicit protocol. BNP results were uploaded from the device memory at study completion. In the BNP-guided group, on days with a BNP level equal to or greater than 200 pg/ml, fluid intake was restricted (baseline infusion < 500 ml/24 h, parenteral nutrition < 1,000 ml/24 h, no saline solutions apart from nutrition and drugs) and furosemide was administered (as intravenous bolus doses of 10 to 30 mg every 3 h, to achieve a target urine output of 4.5 to 9 ml/kg/3 h) (see the online supplement). The 200-pg/ml threshold was chosen on the basis of a previous study showing that BNP levels were higher in patients who failed weaning from mechanical ventilation than in successfully weaned patients (12). Fluid intake restriction and diuretic administration (according to BNP levels on extubation day) were continued for at least 24 hours after extubation in the BNP-guided group. Sodium, potassium, urea, creatinine, and arterial blood gases were monitored daily in all patients. Recommendations were given to prevent and/or treat possible adverse events related to diuretic treatment in the BNP-guided group, as detailed in the online supplement.
TABLE 1. BASELINE CHARACTERISTICS Usual Care Group (n ¼ 152) Age, yr Sex, male McCabe class 0 1 2 SAPS II at ICU admission SOFA score at ICU admission Reason for intubation Coma Septic shock COPD exacerbation Cardiogenic pulmonary edema Pneumonia Cardiac arrest Surgery Other Events between ICU admission and randomization Septic shock* Ventilator-associated pneumonia Acute respiratory distress syndrome* Use of neuromuscular blockers Steroid treatment Duration of invasive mechanical ventilation before inclusion, d Median (IQR) Mean (SD) Diuretic treatment on the day before randomization Urine output on the day before randomization, ml Pressure support test at inclusion Pressure support level, cm H2O PEEP level, cm H2O FIO2 level Cardiopulmonary disease at randomization COPD LVD Neither SOFA score at randomization Arterial blood gases at randomization pH PaCO2, mm Hg PaO2/FIO2 ratio, mm Hg BNP value at randomization, pg/ml
VOL 186
65 (52–74) 102 (67.1%)
BNP-guided Group (n ¼ 152) 66 (55–76) 93 (61.2%)
96 48 8 44 7
(63.2%) (31.6%) (5.3%) (34–56) (4–9)
93 42 17 43 7
(61.2%) (27.6%) (11.2%) (34–54) (4–9)
22 18 10 19 40 10 19 14
(14.5%) (11.8%) (6.6%) (12.5%) (26.3%) (6.6%) (12.5%) (9.2%)
15 21 15 14 50 6 23 8
(9.9%) (13.8%) (9.9%) (9.2%) (32.9%) (3.9%) (15.1%) (5.3%)
61 32 55 35 53
(40.1%) (21.1%) (36.2%) (23.0%) (34.9%)
70 25 53 32 60
(46.1%) (16.4%) (34.9%) (21.1%) (39.5%)
4.4 6.5 64 1,925
(2.7–7.8) (5.7) (42.1%) (1,400–2,750)
5.0 7.5 64 1,928
(3.0–9.1) (7.6) (42.1%) (1,200–3,080)
14 (10–15) 5 (5–8) 40 (35–50)
13 (10–15) 5 (5–6) 40 (30–50)
38 24 90 4
41 20 91 4
7.43 40 218 296
(25.0%) (15.8%) (59.2%) (2–6) (7.39–7.48) (34–45) (176–266) (113–555)
7.43 41 225 256
(27.0%) (13.2%) (59.9%) (3–5) (7.40–7.46) (37–47) (174–297) (91–700)
Definition of abbreviations: BNP ¼ B-type natriuretic peptide; COPD ¼ chronic obstructive pulmonary disease; FIO2 ¼ fraction of inspired oxygen; ICU ¼ intensive care unit; IQR ¼ interquartile range; LVD ¼ left ventricular systolic dysfunction; PEEP ¼ positive end-expiratory pressure; SAPS II ¼ Simplified Acute Physiology Score II; SOFA ¼ Sequential Organ Failure Assessment. Data are presented as n (%) or median (IQR). * At admission or later during the ICU stay.
Mekontso Dessap, Roche-Campo, Kouatchet, et al.: BNP for Fluid Management during Ventilator Weaning
Ventilatory Management During ventilation using the AWS in both groups, sedation was stopped whenever possible, whereas analgesia could be continued, with a target Ramsay score of 2–3. The AWS gradually decreased the PS level while maintaining the patient within a zone of respiratory comfort, as previously described (see the online supplement) (15). When the AWS declared the patient “ready for separation,” extubation was performed as soon as possible (including during the night), after checking for the other required extubation criteria (see the online supplement). Assist-control ventilation was resumed during AWS ventilation in case of respiratory worsening with a respiratory rate greater than 40/minute or hypoxemia (FIO2 . 60% and PEEP . 8 cm H2O required to obtain SpO2 > 90%). The tidal volume target under assist-control ventilation was 6 ml/kg (predicted body weight). BNP was no longer assayed in controlled mode ventilation. When the daily PS test became positive again, the patient was switched back to ventilation using the AWS and managed according to his or her randomization group. The diagnosis of ventilator-associated pneumonia was based on the following usual criteria: systemic signs of infection, new or worsening infiltrates on the chest roentgenogram, purulent tracheal secretions, and bacteriological evidence of pulmonary parenchymal infection (chiefly from distal airway sampling using a protected telescoping catheter or bronchoscopy) (17). Noninvasive ventilation was allowed after extubation if deemed necessary by the attending physician (based on predefined criteria). In the event of reintubation (see the online supplement), the patient was not reventilated using the AWS. Last, a general recommendation was made to investigators to wait until Day 10 after randomization before deciding to perform a tracheotomy, if at all possible.
End Points The primary end point was the time from randomization to successful extubation (patient alive and without reintubation 72 h after extubation). Secondary end points included time to first extubation, time to successful weaning from invasive and noninvasive ventilation (defined
1259
as the time from randomization to completion of 72 h of unassisted spontaneous breathing without noninvasive ventilation for > 3 h/d), ventilator-free days calculated as the number of days without mechanical ventilation within 60 days after randomization (patients who died or were dependent on mechanical ventilation for more than 60 d had zero ventilator-free days), ICU and hospital lengths of stay, ICU and hospital deaths, and mortality on Day 60 after randomization.
Statistical Analysis We estimated the sample size needed to detect an at least 40% decrease in weaning duration in the BNP-guided fluid management group compared with the control group, with an a risk of 5% and a b risk of 10% (power of 90%). In a previous multicenter trial, weaning duration in patients ventilated using the AWS was 4.4 6 4.0 days (15). Assuming a slightly higher standard deviation equal to the mean (4.4), and considering that the use of nonparametric tests might require up to 15% additional subjects (18), a sample size of 150 patients per group was deemed necessary. The data were analyzed with SPSS Base 18 (SPSS Inc, Chicago, IL) and R 2.10.1 (R Foundation for Statistical Computing, Vienna, Austria). Categorical variables were expressed as percentages and continuous data were expressed as medians (25th– 75th percentiles) or means (SD). We used the chi-square or Fisher exact test to compare categorical variables between study groups and the Mann-Whitney test to compare continuous variables, including the primary end point. The primary end point was also analyzed in the three predefined subgroups (COPD, LVD, and neither). We also used the Kaplan-Meier method to assess the effect of BNPguided fluid management on the cumulative probability of successful extubation. Because the proportional hazards assumption was not met during the 60-day follow-up, we used the Breslow-Gehan-Wilcoxon test to assess differences between groups (19). This test allows weighting of time points by the number of cases at risk at each time point (20). Last, the effect of BNP-guided fluid management on the cumulative incidence of successful extubation was assessed while considering the need for continuous sedation as a competing event, according to the
TABLE 2. FLUID MANAGEMENT DURING WEANING Usual Care Group (n ¼ 152) Patients with at least one daily BNP value > 200 pg/ml during weaning, n (%) Patients treated at least once with furosemide during weaning, n (%) Patients treated at least once with acetazolamide during weaning, n (%) Patients treated at least once with any diuretic during weaning, n (%) Cumulative furosemide dose during weaning, mg Median (IQR) Mean (SD) Average daily furosemide dose during weaning, mg Median (IQR) Mean (SD) Cumulative fluid balance during weaning, ml Median (IQR) Mean (SD) Average daily fluid balance during weaning, ml Median (IQR) Mean (SD) Average daily fluid intake during weaning, ml Median (IQR) Mean (SD) Average daily urine output during weaning, ml Median (IQR) Mean (SD) Fluid balance on extubation day,* ml Median (IQR) Mean (SD) Fluid balance the day after extubation,* ml Median (IQR) Mean (SD)
105 108 33 110
(69.1%) (71.1%) (21.7%) (72.4%)
70 (0–160) 180 (544)
BNP-guided Group (n ¼ 152) 100 124 65 127
(65.8%) (81.6%) (42.8%) (83.6%)
P Value 0.541 0.031 ,0.0001 0.019 0.003
118 (23–229) 180 (231) ,0.0001
14 (0 to 40) 30 (50) 2180 (22,556 to 2,832) 847 (6,569)
40 (9 to 78) 47 (41) 22,320 (24,735 to 738) 21,402 (5,818)
237 (2731 to 586) 2136 (1,312)
2640 (21,811 to 225) 2852 (1,456)
2,226 (1,758 to 2,730) 2,324 (876)
2,040 (1,650 to 2,629) 2,188 (774)
2,273 (1,838 to 2,973) 2,461 (1,039)
2,836 (2,057 to 3,905) 3,044 (1,240)
,0.0001
,0.0001
0.105
,0.0001 0.318
21,180 (22,124 to 42) 21,078 (1,639)
21,047 (22,540 to 2350) 21,263 (1,759) 0.223
2715 (21,526 to 30) 751 (1,339)
Definition of abbreviations: BNP ¼ B-type natriuretic peptide; IQR ¼ interquartile range. Negative fluid balance was defined as urine output exceeding fluid intake. * Fluid balances on extubation day and the day after extubation were available in 274 and 229 patients, respectively.
2479 (21,360 to 277) 2646 (1,469)
1260
AMERICAN JOURNAL OF RESPIRATORY AND CRITICAL CARE MEDICINE
VOL 186
2012
TABLE 3. MAIN OUTCOMES
Time to first extubation, h Median (IQR) Mean (SD) Time to successful extubation, h Median (IQR) Mean (SD) Time to successful weaning from invasive and noninvasive ventilation, h Median (IQR) Mean (SD) Ventilator-free days from randomization to Day 14, d Median (IQR) Mean (SD) Ventilator-free days from randomization to Day 28, d Median (IQR) Mean (SD) Ventilator-free days from randomization to Day 60, d Median (IQR) Mean (SD) ICU stay length, d Median (IQR) Mean (SD) Hospital stay length, d Median (IQR) Mean (SD) ICU mortality Hospital mortality Day-60 mortality
Usual Care Group (n ¼ 152)
BNP-guided Group (n ¼ 152)
P Value
47.7 (22.9–124.8) 92.8 (110.2)
39.8 (20.0–72.4) 70.6 (106.8)
0.019
58.6 (23.3–139.8) 112.2 (147.1)
42.4 (20.8–107.5) 86.2 (127.9)
0.034
74.4 (31.7–160.5) 134.3 (187.6)
49.3 (21.9–140.6) 107.1 (141.0)
0.051
9.7 (2.3–12.9) 8.2 (5.2)
12.0 (6.5–13.1) 9.3 (4.9)
0.026
23.3 (14.7–26.7) 18.9 (10.4)
25.9 (19.3–27.1) 20.3 (10.4)
0.038
54.9 (38.7–58.3) 42.8 (23.7)
57.9 (50.4–59.1) 45.7 (22.7)
0.015
8.0 (4.0–13.0) 11.6 (12.3)
8.0 (4.0–14.0) 11.4 (11.2)
0.995
20.0 27.3 19 25 28
20.0 24.0 18 20 21
0.796
(12.0–33.0) (37.3) (12.5%) (16.4%) (18.4%)
(13.0–33.0) (14.2) (11.8%) (13.2%) (13.8%)
0.861 0.433 0.275
Definition of abbreviations: BNP ¼ B-type natriuretic peptide; ICU ¼ intensive care unit; IQR ¼ interquartile range.
Gray model (21, 22). Two-sided P values less than 0.05 were considered significant. This study was registered on ClinicalTrials.gov with the number NCT00473148.
RESULTS Enrollment and Baseline Characteristics
Patients eligible for weaning (1,464) were screened for enrollment between May 2007 and July 2009. Among them, 306 were enrolled and randomized (Figure 1) to the control group (n ¼
152) or BNP-guided group (n ¼ 154). Two patients (assigned to the BNP-guided group) were excluded from the data analysis because of lack of continued consent to use their data. The withdrawal of consent was not related to any particular aspect of the protocol. The two groups were similar at baseline regarding demographic characteristics, reason for intubation, severity of illness, respiratory function, duration of invasive mechanical ventilation, and urine output before study initiation (Table 1). BNP values at randomization and the proportions of patients with COPD and LVD were also similar between the two groups (Table 1). In the overall population, BNP values at randomization
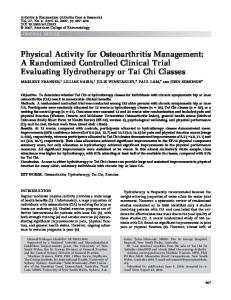
Figure 2. Probability of successful extubation within 60 days after randomization. BNP ¼ B-type natriuretic peptide.
Mekontso Dessap, Roche-Campo, Kouatchet, et al.: BNP for Fluid Management during Ventilator Weaning
1261
were higher in patients with LVD (552 [328–990] pg/ml) than in patients with COPD (263 [115–803] pg/ml; P ¼ 0.006) or neither disease (230 [72–485] pg/ml; P , 0.0001). Diuretics and Fluid Balance
Fluid management during weaning is reported in Table 2. During the weaning process, the percentage of patients with at least one daily BNP value equal to or greater than 200 pg/ml was similar in the two groups. Compared with the control group, the BNP-guided group had a higher proportion of patients receiving diuretics, which were used in higher doses, resulting in a significantly more negative fluid balance during the weaning period. Fluid balance on the day of extubation and the day after extubation were similar between groups. Main End Points
The weaning time was significantly shorter and the number of ventilator-free days significantly higher in the BNP-guided group compared with the control group (Table 3). The probability of successful extubation was significantly increased with the BNPguided strategy (P ¼ 0.022, Breslow test; Figure 2), and this difference persisted after adjustment for need for continuous sedation as a competing event (P ¼ 0.01, Gray test). No difference was found for length of stay, ICU mortality, or hospital mortality (Table 3). Although stratification into three subgroups did not provide sufficient power to analyze each subgroup separately, the differences between the two strategies in times to first extubation, to successful extubation, and to successful weaning were significant in patients with LVD, suggesting a stronger effect of BNP-guided fluid management in this subgroup than in the other two subgroups (Figure 3). Complications during Weaning
Complications during weaning are reported in Table 4. The need for noninvasive ventilation after extubation, reintubation rate within 72 hours after extubation, tracheostomy rate, and need for prolonged mechanical ventilation (.14 d after randomization) were similar between groups. There were no significant between-group differences in the percentages of patients with hypokalemia, hypernatremia, metabolic alkalosis, or renal failure. During the weaning period, significantly fewer patients in the BNP-guided group experienced clinical worsening requiring reventilation with assist-control ventilation, developed ventilatorassociated pneumonia, or needed continuous sedation or episodes of fluid loading, compared with the control group.
DISCUSSION There is currently no objective practical guide to fluid management during weaning from mechanical ventilation. In this randomized controlled trial, a simple BNP-guided fluid management strategy was associated with increased diuretic use, a more negative fluid balance, and a shorter duration of mechanical ventilation, especially in patients with LVD. There was no increase in organ failures. Several factors may confer an advantage to BNP-guided fluid management over the usual clinical approach during weaning. BNP guidance is probably a preventive and patient-tailored strategy allowing more conservative fluid management in patients at high risk for difficult weaning (12, 14). Acute heart failure is a common cause of unsuccessful weaning from mechanical ventilation (9, 10, 13). Its pathophysiology is complex and involves changes in intrathoracic pressure and cardiac
Figure 3. Mean and standard deviation for time (in hours) to first extubation (top), time (in hours) to successful extubation (middle), and time (in hours) to successful weaning from invasive and noninvasive ventilation (bottom) in patients with chronic obstructive pulmonary disease, left ventricular systolic dysfunction, or neither. BNP ¼ B-type natriuretic peptide; COPD ¼ chronic obstructive pulmonary disease; LVD ¼ left ventricular systolic dysfunction; neither ¼ no COPD or LVD. *P , 0.05 between the usual care and BNP-guided groups (Mann-Whitney test).
loading conditions, left ventricular systolic (9) and diastolic (23) dysfunction, and fluid overload (8). Positive fluid balance is associated with prolonged mechanical ventilation (24, 25) and extubation failure (11). In patients with weaning-induced heart failure, successful weaning was achieved after diuretic treatment in several open studies (8, 12). The BNP measurement acted as an incentive to consider negative fluid balance while diuresis was managed according to a predefined protocol to minimize bias. Previous studies of goal-directed fluid management in mechanically ventilated critically ill patients have shown beneficial effects with interventions aimed at lowering fluid balance (4– 6, 26). They differed from ours in terms of the protocols, patient populations, and timing of the interventions (4–6, 26). We used
1262
AMERICAN JOURNAL OF RESPIRATORY AND CRITICAL CARE MEDICINE
VOL 186
2012
TABLE 4. COMPLICATIONS DURING WEANING Usual Care Group (n ¼ 152) Respiratory function Clinical worsening requiring a return to assist-control ventilation Ventilator-associated pneumonia Need for noninvasive ventilation after extubation Reintubation within 72 h after extubation Tracheostomy Mechanical ventilation for .14 d after randomization Cardiovascular function Supraventricular arrhythmia Ventricular arrhythmia Systolic arterial pressure , 90 mm Hg Need for fluid loading Need for catecholamine infusion Neurological function Need for continuous sedation because of clinical worsening Need for continuous analgesia Renal and metabolic functions Arterial pH . 7.50 Blood potassium , 3.5 mEq/L Blood sodium . 150 mEq/L Plasma creatinine . 150 mmol/L Plasma creatinine . 180 mmol/L Blood urea nitrogen . 15 mmol/L Blood urea nitrogen . 25 mmol/L Need for dialysis
BNP-guided Group (n ¼ 152)
P Value
66 27 49/138 17/138 13 20
(43.4%) (17.8%) (35.5%) (12.3%) (8.6%) (13.2%)
42 14 53/142 23/144 21 20
(27.6%) (9.2%) (37.3%) (16.0%) (13.8%) (13.2%)
0.004 0.029 0.752 0.379 0.145 .0.999
18 4 49 53 40
(11.8%) (2.6%) (32.2%) (34.9%) (26.3%)
17 1 40 36 39
(11.2%) (0.7%) (26.3%) (23.7%) (25.7%)
0.857 0.216 0.257 0.032 0.896
80 (52.6%) 70 (46.1%)
61 (40.1%) 61 (40.1%)
0.029 0.297
31 58 7 13 3 36 7 0
20 70 3 10 6 32 8 0
(20.4%) (38.2%) (4.6%) (8.6%) (2.0%) (23.7%) (4.6%) (0%)
(13.2%) (46.1%) (2.0%) (6.6%) (3.9%) (21.1%) (5.3%) (0%)
0.09 0.163 0.198 0.515 0.501 0.582 0.791 .0.999
Definition of abbreviation: BNP ¼ B-type natriuretic peptide. Data represent n (%).
BNP in patients fulfilling criteria for early weaning, whereas they used more complex algorithms usually targeting invasive measurements such as extravascular lung water, central venous pressure, or pulmonary artery occlusion pressure (4–6, 26). We do not know whether driving the protocol instructions by these invasive measurements would have modified the effect of our intervention. Such invasive measurements are difficult to implement in practice in the context of weaning, which is usually associated with a decrease in the overall invasiveness of management. In addition, conventional tools used to diagnose cardiovascular dysfunction raise technical challenges in patients who are being weaned off mechanical ventilation, because of the large swings in intrathoracic pressures. This fact has generated interest in the use of cardiac biomarkers during weaning. Data have suggested that natriuretic peptides (BNP and N-terminal pro–B-type natriuretic peptide [NT-proBNP]) may predict the weaning outcome and help to determine whether weaning failure is caused by cardiovascular dysfunction (12–14). Better outcomes have been shown with explicit BNP-guided pharmacotherapy compared with empirical therapy dictated by clinical acumen in circumstances other than weaning from mechanical ventilation, especially in outpatients with chronic heart failure (27) and in patients presenting to the emergency department with acute dyspnea (28). In our study, although the BNP-guided strategy induced significant benefits in the overall intervention group, patients with LVD showed the strongest effect, whereas those with COPD seemed less likely to benefit. Natriuretic peptides are secreted primarily by the left ventricle in response to changes in left ventricular wall stretch, and their concentrations correlate closely with filling pressures in patients with LVD (29). LVD is a risk factor for weaning failure of cardiovascular origin (9). In patients with LVD, high-pressure pulmonary edema and an inadequate cardiac output may constitute major obstacles to weaning from mechanical ventilation (30). By contrast, weaning difficulties in other groups of patients may be due to other factors such as poor respiratory mechanics, elevated work of breathing, or CO2 retention in patients with COPD (31). In
addition, elevated BNP in patients with COPD may be partly related to pulmonary hypertension and increased right ventricle afterload (32), a form of cardiac dysfunction that may not always respond well to diuretics. Possible explanations for the lower rate of ventilatorassociated pneumonia in the BNP-guided fluid management group may include decreased risk exposure (earlier separation from the ventilator) and a direct effect of fluid balance on bacterial colonization and infectivity. The strict criteria used to diagnose pneumonia limited the possibility that respiratory symptom worsening due to pulmonary edema may have been mistaken for pneumonia in some patients. There were more episodes of worsening and need for sedation in the control group, and our analysis adjusted on sedation suggests that this may be a consequence of a less aggressive reduction of fluid balance in the control group. The BNP-guided strategy had no adverse consequences on hemodynamic or renal function. Arterial pressure, vasopressor requirements, blood urea nitrogen, and creatinine level were similar in the two groups. The protocols were designed to minimize risks, and diuretic therapy was titrated on the basis of the patient’s response and was avoided in patients with worsening renal function. Frequent use of acetazolamide was a necessary part of the protocol to avoid alkalemia. Electrolyte levels were monitored closely during diuretic therapy and were comparable between groups. Because we tested specific management strategies that used several safeguards, we do not know whether the BNP-guided fluid management strategy would be as safe and as beneficial when using the simplified target of a zero fluid balance or zero weight gain. In addition, departures from the specific inclusion and noninclusion criteria used in this trial may lead to clinical outcomes that differ from those observed in this study. This point may affect the generalizability of our study, that is, its external validity, which may also be influenced by the general fluid balance policy of a given ICU. Although cardiac dysfunction is the most important source of BNP variations in critically ill patients, other major factors include sepsis and renal failure. We did not
Mekontso Dessap, Roche-Campo, Kouatchet, et al.: BNP for Fluid Management during Ventilator Weaning
include patients with renal failure, because of the influence of renal function on BNP levels. The weaning procedure was relatively brief in the control group. This finding may be related to our selection criteria and/or to the use of the AWS (15). Using the AWS, however, allowed optimal standardization of the weaning procedure. Because the study was not blinded and all participating physicians were aware of the study question, diuretics may have been used more widely than usual in the control group, which would tend to minimize the difference in weaning duration between the groups. Although a greater clinician presence, assessment, and involvement in the BNP-guided group as compared with the usual care group cannot be excluded, the use of a strict protocol for diuresis and of AWS allowed us to make the weaning process relatively independent from physician care. In conclusion, we found that the use of a BNP-driven fluid management protocol during weaning from mechanical ventilation decreased the fluid balance and duration of weaning without increasing adverse events, compared with physician-guided fluid management, especially in patients with LVD. We detected no significant differences in mortality rate or length of stay between the two approaches. Author disclosures are available with the text of this article at www.atsjournals.org.
References 1. Cook DJ, Walter SD, Cook RJ, Griffith LE, Guyatt GH, Leasa D, Jaeschke RZ, Brun-Buisson C. Incidence of and risk factors for ventilator-associated pneumonia in critically ill patients. Ann Intern Med 1998;129:433–440. 2. Esteban A, Alia I, Ibanez J, Benito S, Tobin MJ; Spanish Lung Failure Collaborative Group. Modes of mechanical ventilation and weaning: a national survey of Spanish hospitals. Chest 1994;106:1188–1193. 3. Humphrey H, Hall J, Sznajder I, Silverstein M, Wood L. Improved survival in ARDS patients associated with a reduction in pulmonary capillary wedge pressure. Chest 1990;97:1176–1180. 4. Mitchell JP, Schuller D, Calandrino FS, Schuster DP. Improved outcome based on fluid management in critically ill patients requiring pulmonary artery catheterization. Am Rev Respir Dis 1992;145:990–998. 5. Martin GS, Mangialardi RJ, Wheeler AP, Dupont WD, Morris JA, Bernard GR. Albumin and furosemide therapy in hypoproteinemic patients with acute lung injury. Crit Care Med 2002;30:2175–2182. 6. Wiedemann HP, Wheeler AP, Bernard GR, Thompson BT, Hayden D, deBoisblanc B, Connors AF Jr, Hite RD, Harabin AL. Comparison of two fluid-management strategies in acute lung injury. N Engl J Med 2006;354:2564–2575. 7. Jubran A, Mathru M, Dries D, Tobin MJ. Continuous recordings of mixed venous oxygen saturation during weaning from mechanical ventilation and the ramifications thereof. Am J Respir Crit Care Med 1998;158:1763–1769. 8. Lemaire F, Teboul JL, Cinotti L, Giotto G, Abrouk F, Steg G, MacquinMavier I, Zapol WM. Acute left ventricular dysfunction during unsuccessful weaning from mechanical ventilation. Anesthesiology 1988; 69:171–179. 9. Caille V, Amiel JB, Charron C, Belliard G, Vieillard-Baron A, Vignon P. Echocardiography: a help in the weaning process. Crit Care 2010; 14:R120. 10. Lamia B, Maizel J, Ochagavia A, Chemla D, Osman D, Richard C, Teboul JL. Echocardiographic diagnosis of pulmonary artery occlusion pressure elevation during weaning from mechanical ventilation. Crit Care Med 2009;37:1696–1701. 11. Frutos-Vivar F, Ferguson ND, Esteban A, Epstein SK, Arabi Y, Apezteguia C, Gonzalez M, Hill NS, Nava S, D’Empaire G, et al. Risk factors for extubation failure in patients following a successful spontaneous breathing trial. Chest 2006;130:1664–1671.
1263
12. Mekontso-Dessap A, de Prost N, Girou E, Braconnier F, Lemaire F, Brun-Buisson C, Brochard L. B-type natriuretic peptide and weaning from mechanical ventilation. Intensive Care Med 2006;32:1529–1536. 13. Grasso S, Leone A, De Michele M, Anaclerio R, Cafarelli A, Ancona G, Stripoli T, Bruno F, Pugliese P, Dambrosio M, et al. Use of N-terminal pro– brain natriuretic peptide to detect acute cardiac dysfunction during weaning failure in difficult-to-wean patients with chronic obstructive pulmonary disease. Crit Care Med 2007;35:96–105. 14. Zapata L, Vera P, Roglan A, Gich I, Ordonez-Llanos J, Betbese AJ. B-type natriuretic peptides for prediction and diagnosis of weaning failure from cardiac origin. Intensive Care Med 2011;37:477–485. 15. Lellouche F, Mancebo J, Jolliet P, Roeseler J, Schortgen F, Dojat M, Cabello B, Bouadma L, Rodriguez P, Maggiore S, et al. A multicenter randomized trial of computer-driven protocolized weaning from mechanical ventilation. Am J Respir Crit Care Med 2006;174:894–900. 16. Mekontso Dessap A, Roche Campo F, Kouatchet A, Tomicic V, Beduneau G, Surugue G, Cabello B, Jaber S, Azoulay E, Castaranes D, et al. Sevrage de la ventilation mécanique guidé par le peptide natriurétique de type B: essai randomisé contrôlé multinational [abstract]. Reanimation 2011;20:S41. 17. Chastre J, Fagon JY. Ventilator-associated pneumonia. Am J Respir Crit Care Med 2002;165:867–903. 18. Lehmann EL, D’Abrera HJM. Nonparametrics: statistical methods based on ranks. New York: Springer; 2006. pp. 76–81. 19. Breslow N. A generalized Kruskal-Wallis test for comparing K samples subject to unequal patterns of censorship. Biometrika 1970;57:579– 594. 20. Hosmer DW, Lemeshow S, May S. Applied survival analysis: regression modeling of time to event data [Wiley series in probability and statistics]. Hoboken, NJ: Wiley-Interscience; 2008. pp. 47–48. 21. Fine JP, Gray RJ. A proportional hazards model for the model for the subdistribution of a competing risk. J Am Stat Assoc 1999;94:496–509. 22. Gray RJ. A class of K-sample tests for comparing the cumulative incidence of a competing risk. Ann Stat 1988;16:1141–1154. 23. Papanikolaou J, Makris D, Saranteas T, Karakitsos D, Zintzaras E, Karabinis A, Kostopanagiotou G, Zakynthinos E. New insights into weaning from mechanical ventilation: left ventricular diastolic dysfunction is a key player. Intensive Care Med 2011;37:1976–1985. 24. Epstein CD, Peerless JR. Weaning readiness and fluid balance in older critically ill surgical patients. Am J Crit Care 2006;15:54–64. 25. Upadya A, Tilluckdharry L, Muralidharan V, Amoateng-Adjepong Y, Manthous CA. Fluid balance and weaning outcomes. Intensive Care Med 2005;31:1643–1647. 26. Martin GS, Moss M, Wheeler AP, Mealer M, Morris JA, Bernard GR. A randomized, controlled trial of furosemide with or without albumin in hypoproteinemic patients with acute lung injury. Crit Care Med 2005; 33:1681–1687. 27. Porapakkham P, Porapakkham P, Zimmet H, Billah B, Krum H. B-type natriuretic peptide–guided heart failure therapy: a meta-analysis. Arch Intern Med 2010;170:507–514. 28. Lam LL, Cameron PA, Schneider HG, Abramson MJ, Muller C, Krum H. Meta-analysis: effect of B-type natriuretic peptide testing on clinical outcomes in patients with acute dyspnea in the emergency setting. Ann Intern Med 2010;153:728–735. 29. Richards AM, Crozier IG, Yandle TG, Espiner EA, Ikram H, Nicholls MG. Brain natriuretic factor: regional plasma concentrations and correlations with haemodynamic state in cardiac disease. Br Heart J 1993;69:414–417. 30. Zakynthinos S, Routsi C, Vassilakopoulos T, Kaltsas P, Zakynthinos E, Kazi D, Roussos C. Differential cardiovascular responses during weaning failure: effects on tissue oxygenation and lactate. Intensive Care Med 2005;31:1634–1642. 31. Tobin MJ, Laghi F, Brochard L. Role of the respiratory muscles in acute respiratory failure of COPD: lessons from weaning failure. J Appl Physiol 2009;107:962–970. 32. Bando M, Ishii Y, Sugiyama Y, Kitamura S. Elevated plasma brain natriuretic peptide levels in chronic respiratory failure with cor pulmonale. Respir Med 1999;93:507–514.