AJCP / Review Article
B-Acute Lymphoblastic Leukemia/Lymphoblastic Lymphoma Sanam Loghavi, MD,1 Jeffery L. Kutok, MD, PhD,2 and Jeffrey L. Jorgensen, MD, PhD1 From the 1Department of Hematopathology, The University of Texas MD Anderson Cancer Center, Houston; and 2Infinity Pharmaceuticals, Cambridge, MA. Key Words: B-ALL; Cytogenetics; Myeloid; Flow cytometry immunophenotyping Am J Clin Pathol September 2015;144:393-410 DOI: 10.1309/AJCPAN7BH5DNYWZB
Objectives: This session of the 2013 Society of Hematopathology/European Association for Haematopathology Workshop was dedicated to B-acute lymphoblastic leukemia (B-ALL)/lymphoblastic lymphoma (LBL) with recurrent translocations and not otherwise specified. Methods: In this review, we summarize the cases discussed during the workshop, review the pertinent and most recent literature on the respective topics, and provide a few key points that may aid in the workup of patients with B-ALL/LBL. Results: Many of the submitted cases showed interesting diagnostic, immunophenotypic, or clinical aspects of B-ALL with BCR/ABL1, MLL-associated, and other recurrent chromosomal abnormalities. Several cases showed rare aberrancies such as coexistent IGH/BCL2 and MYC rearrangements and raised issues in classification. Other cases had unusual clinical presentations, including B-ALL with hypereosinophilia and therapy-related B-ALL. Several cases highlighted the role of flow cytometry immunophenotyping in distinguishing benign B-cell precursors from aberrant lymphoblasts, and other cases raised questions regarding the clinical importance of myeloperoxidase positivity in acute lymphoblastic leukemia. Conclusions: The complexity and spectrum of cases presented in this review highlight the importance of clinicopathologic correlation and the value of ancillary studies in the classification and workup of patients with B-ALL/LBL.
© American Society for Clinical Pathology
B-acute lymphoblastic leukemia (B-ALL)/lymphoblastic lymphoma (LBL) is a neoplasm of immature B-cell precursors that typically affects children younger than 6 years but is also encountered in older children and in adult populations. The estimated global incidence of B-ALL is around one to five per 100,000 persons per year.1 Patients with B-ALL usually have signs and symptoms of bone marrow (BM) failure, including cytopenias with or without leukocytosis. The diagnosis is established by immunophenotyping, commonly by flow cytometry (FC), which shows immature B lineage. Many cases of B-ALL harbor recurrent chromosomal abnormalities, including balanced chromosomal translocations, which are often critical determinants of prognosis.
B-ALL With Recurrent Cytogenetic Abnormalities What Are the Features of Philadelphia Chromosome–Positive B-ALL? Approximately 20% to 30% of adult acute lymphoblastic leukemias (ALLs) and 5% of pediatric ALLs harbor the Philadelphia (Ph) chromosome. This genetic alteration confers a poor prognosis, as defined by shorter remission duration and shorter survival and higher rates of resistance to standard chemotherapy.2-4 Allogeneic stem cell transplant in first remission is a common therapeutic option. The Ph chromosome is the result of t(9;22)(q34;q11.2) that creates a BCR-ABL1 fusion gene residing on a minute derivative chromosome 22. The fusion gene encodes a constitutively
Am J Clin Pathol 2015;144:393-410 393 DOI: 10.1309/AJCPAN7BH5DNYWZB
Downloaded from http://ajcp.oxfordjournals.org/ by guest on January 17, 2017
ABSTRACT
Loghavi et al / B-ALL/Lymphoblastic Lymphoma
394 Am J Clin Pathol 2015;144:393-410 DOI: 10.1309/AJCPAN7BH5DNYWZB
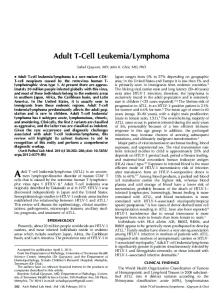
on the unaffected allele.28,29 Recent studies have shown that IKZF1 deletions are independent poor prognostic indicators in BCR-ABL1–negative as well as BCR-ABL1– positive B-ALL in both pediatric and adult patients.30-37 IKZF1 deletions are significantly more common (~70%) in Ph+ B-ALL compared with BCR-ABL1–negative disease.28,35,38-41 Mullighan et al38 identified a high frequency of IKZF1 copy number alterations as well as deleterious mutations of IKZF1 in Ph+ ALL and CML in blast phase but not in chronic phase CML. Their findings suggest that Ikaros alterations are directly linked to leukemogenesis in Ph+ ALL. In a pediatric-based study by van der Veer et al,36 the negative effect of IKZF1 deletion in Ph+ B-ALL persisted even in patients who were treated with TKIs, irrespective of whether they received hematopoietic stem cell transplant. The authors suggested that IKZF1 be used in further risk stratification and therapy planning in patients with BCR-ABL1–positive B-ALL. Martinelli et al39 showed similar effects in adults with Ph+ B-ALL. Using gene expression profiling techniques, recent studies have shown evidence of activated Bruton tyrosine kinase (BTK) and JAK-STAT pathways in B-ALL with IKZF1 deletion, suggesting a potential role for targeted therapy with BTK and JAK inhibitors in this patient population.42,43 What Are the Features of B-ALL With Associated MLL Alterations? Six cases (118, 203, 235, 272, 386, and 415) submitted to this session were examples of de novo B-ALL with MLL (11q23) gene rearrangements. More than 75 gene partners for MLL have been identified.44-47 B-ALL associated with MLL gene rearrangements represents a distinctive group with characteristic clinical findings, gene expression signature, and immunophenotypic and prognostic features. Patients with these tumors have a bimodal age distribution with high prevalence among infants younger than 1 year of age and an increasing incidence in later adulthood, while being relatively uncommon in older children. Approximately 20% of all cases of ALL, including 80% of infant ALL and 10% of older children and adult ALL, exhibit MLL rearrangements. Both infants and adults with B-ALL associated with MLL rearrangements have a poor prognosis.48,49 The t(4;11)(q21;q23) with an AF4 fusion partner is most common in infants, but other fusion partners also can be seen in infants (cases 118 and 386), and t(4;11)(q21;q23) also can be observed in adults (case 272). Most B-ALL cases with MLL alterations show a characteristic aberrant immunophenotype ❚Image 2❚, with absence of CD10 and expression of the myeloid markers CD15, CD33, and/or CD65s.21,48,50 This pattern was seen in four of six cases in this session, with one tumor (case 386) showing partial positivity for CD10. Two cases showed unusual
© American Society for Clinical Pathology
Downloaded from http://ajcp.oxfordjournals.org/ by guest on January 17, 2017
active BCR-ABL1 tyrosine kinase, which in turn promotes unregulated cell proliferation. Case 164 was an example of a patient with Ph+ B-ALL (BCR-ABL1; p190), refractory to induction chemotherapy, who achieved complete remission with dasatinib, a secondgeneration tyrosine kinase inhibitor (TKI). Targeted therapy with TKIs in combination with conventional chemotherapy has dramatically improved the outcome of patients with Ph+ B-ALL.5-8 The addition of the first-generation TKI, imatinib, to standard chemotherapy regimens has substantially increased complete remission rates in patients with B-ALL; however, up to 30% of patients are either initially resistant or eventually go on to develop resistance to imatinib, most commonly as a result of BCR-ABL kinase domain mutations.9,10 Alternatively, imatinib resistance has also been attributed to the Src family of kinases that are involved in ALL leukemogenesis but are unresponsive to imatinib.11,12 The e1a2 (p190) fusion transcript, as seen in patient 164, has been shown to be associated with unfavorable response to imatinib therapy with short-lived responses in the setting of chronic myelogenous leukemia (CML).13-15 Dasatinib, a dual Src/Abl kinase inhibitor, has shown clinical efficacy in inducing substantially better hematologic and cytogenetic remission in patients with Ph+ ALL with imatinib resistance.16-18 The superior effect of dasatinib may be attributed to its increased potency, its ability to inhibit mutant variants of BCR-ABL, and/or its capability to target Src family kinases. Three additional patients with Ph+ B-ALL (cases 109, 314, and 335) were discussed ❚Table 1❚. Ph+ B-ALL blasts often show high expression levels of CD10 (uniform, bright), CD11b, CD13, CD15, CD25, and CD66c, as well as partial or complete lack of CD34 expression.19-22 Case 314 was a child with Down syndrome (DS) and B-ALL. Apart from t(8;14)(q11;q32), which is significantly overrepresented in DS children with B-ALL, the incidence of recurrent chromosomal abnormalities associated with B-ALL, including t(9;22), is significantly lower in this patient population. The lower frequency of unfavorable recurrent cytogenetic abnormalities may account for the better clinical outcome in this population.23-26 Case 210 was a patient with recurrent Ph+ B-ALL with an IKZF1 deletion ❚Image 1❚. The IKZF1 gene encodes for Ikaros, a protein involved in B-cell differentiation and proliferation, presumably by modulating immunoglobulin heavy chain gene (IGH) rearrangement and cell signaling in immature B-cell receptors.27 Wild-type Ikaros has been shown to harbor tumor suppressor activity. Partial or complete deletions of IKZF1 affecting the gene start codon on exon 2 lead to haploinsufficiency, while deletions of DNAbinding domains on exons 4 to 7 result in loss of tumor suppressor activity via their dominant negative effect
AJCP / Review Article
❚Table 1❚ Summary of Cases Submitted to the 2013 Society of Hematopathology/European Association for Haematopathology Workshop: B-Acute Lymphoblastic Leukemia/Lymphoblastic Lymphoma Case No.
Diagnosis
Ph+ B-ALL 164 109
B-ALL, Ph+ (BCR/ABL1; p190) B-ALL, Ph+ (BCR/ABL1; p210)
314 335 210 B-ALL with associated with MLL alterations 272 203
386 118 415 B-ALL with associated myeloid proliferations 104 132 371 387 102 B-ALL with a hypodiploid karyotype 11
Refractory to ALL induction therapy but CR with dasatinib Characteristic phenotype: CD10++, CD34+, CD13 dim+, CD38± B-ALL with Ph+ in DS Ph+ is rare in DS; CD10 subset+, CD13+, CD34+ B-ALL with Ph+ and complex karyotype CD10++, CD19+, CD20 dim+, CD33 dim+, CD34 partial+, (monotypic surface light chain) CD45 dim+, TdT+, sk dim+ Recurrent Ph+ B-ALL, with IKZF1, EBF1, and SNP array; IKZF1 deletion associated with poor prognosis PAX5 deletion B-ALL with t(4;11)(q21;q23)/MLL rearranged
Adult, MLL-associated phenotype (CD10–, CD19+, HLADR+ by flow cytometry; PAX5+ and CD79a+ by IHC) B-ALL with 46,XX.ish A cryptic insertional translocation resulting in MLLT1/ ins(11;19)(q23;p13.3p13.3) MLL fusion demonstrated by FISH; MLL-associated (MLL+,MLLT1+;MLLT1+)/MLL rearranged phenotype (CD10–) B-ALL with MLL gene rearrangement Adult presentation; MLL-associated phenotype (CD19+, CD10–, CD15+) Congenital B-ALL with t(11;19)(q23;p13.3)/ 38-week old with MLL-associated phenotype but subset MLL rearranged CD10+; not the typical t(4;11) seen in infants B-ALL with AF9-MLL fusion (t(9;11)) Infant with mature B-cell phenotype with surface l light chains; not typical t(4;11) seen in infants Mature B-cell leukemia/lymphoma with Child with mature B-cell phenotype with sIgM l, negative t(4;11) for CD10, CD20, CD34, and TdT B-ALL with t(5;14)(q31;q32) B-ALL with t(5;14)(q31;q32) B-ALL with eosinophilia and IGH gene rearrangement by FISH B-ALL with hypereosinophilia Concurrent B-ALL and myeloproliferative neoplasm, not otherwise specified
B-ALL with a doubled, near-haploid karyotype Masked hypodiploid karyotype identified by SNP array
TdT+ B-cell neoplasms with BCL2 and/or MYC alterations 159 High-grade TdT+ blastic B-cell leukemia/ lymphoma with t(8;22), t(14;18), and t(3;13)(q27;q14); possible transformation of follicular lymphoma 301 High-grade TdT+ blastic B-cell leukemia/ lymphoma with BCL2 (18q21) and MYC (8q24) translocations 338 High-grade TdT+ blastic B-cell leukemia/ lymphoma with t(14;18) 369 High-grade TdT+ blastic B-cell leukemia/ lymphoma with BCL2 (18q21) and MYC (8q24) translocations 149 B-ALL with t(8;22)(q24.1;q11.2) B-ALL not otherwise specified with normal karyotype 321
Eosinophilia; 47,XY,(5;14)(q31;q32),+22; PDGFRB not involved Eosinophilia; 47,XX,(5;14)(q31;q32) with additional 20q– Eosinophilia; FISH + for IGH rearrangement; FIP1L1PDGFRA, TCR b and g rearrangements negative Marked eosinophilia; FISH negative for abnormalities in PDGFRA, PDGFRB, FGFR1, MLL, IL-3, and BCR-ABL1 fusion 1p uniparental disomy (UPD1p) as well as MPL (p.W515S) gene mutation
B-ALL
© American Society for Clinical Pathology
Widespread lymphadenopathy, sheets of BM blasts; CD10+, CD20 dim+, TdT+, CD34-sIg–; small mature subset, CD20 bright sIg+, CD10-TdT– Abdominal mass, sheets of BM blasts; CD10+, CD19+, TdT+, CD20–, CD34–, sIg– Abdominal mass, sheets of BM blasts; CD10+, CD19+, TdT+, CD20–, CD34–, sIg–, high SSC History of follicular lymphoma and DH lymphoma; retroperitoneal mass, sheets of BM blasts; CD10+, CD19+, TdT+, CD20–, CD34–, sIg– Retroperitoneal lymphadenopathy, sheets of BM blasts; CD10+, CD19+, CD34 subset+, TdT+, CD20– Gene expression profiling: high FLT3 expression, “cluster group 5,” associated with better prognosis
Am J Clin Pathol 2015;144:393-410 395 DOI: 10.1309/AJCPAN7BH5DNYWZB
Downloaded from http://ajcp.oxfordjournals.org/ by guest on January 17, 2017
235
Interesting Features
Loghavi et al / B-ALL/Lymphoblastic Lymphoma
❚Table 1❚ (cont) Summary of Cases Submitted to the 2013 Society of Hematopathology/European Association for Haematopathology Workshop: B-Acute Lymphoblastic Leukemia/Lymphoblastic Lymphoma Case No.
Diagnosis
Interesting Features
Distinguishing B-ALL from normal counterparts by flow cytometry 142
Residual B-ALL
Aberrant phenotype by flow cytometry (4%) posttherapy, CD58 bright+ Presented with cytopenias; 6% aberrant lymphoblasts by flow cytometry; rebiopsy after 6 weeks showed 80% blasts ~50% atypical cells but benign phenotype by flow cytometry
152
B-ALL with initial oligoblastic presentation
178
BM with prominent regenerating immature B-cell population
98
Other unusual immunophenotypic findings in B-ALL 128 260 Therapy-related B-ALL 297
Therapy-related myeloid neoplasm, mixed phenotype acute leukemia (myeloid/B)
B-ALL with minimal CD19 expression B-ALL with partial immunophenotypic shift at relapse Therapy-related B-ALL with t(4;11)(q21;q23)
157
Therapy-related B-ALL
336
Therapy-related B-ALL
96
Therapy-related B-ALL, with t(4;11)(q?21; q?23)/MLL rearrangement Therapy-related abnormal population of B-lymphoid blasts
429
B-ALL associated with HLH (infection-associated hemophagocytic syndrome) 259 Novel therapy 264 224
CD19+, CD15+, TdT+; CD10–; MPO+ by IHC, MPO– by flow cytometry BM CD13+, CD19+, CD33+; CSF blasts with two subsets: CD13+, MPO+, CD19–, CD22–, TdT– vs CD13+, CD22+, TdT+, CD19–, MPO– History of ovarian CA, cytotoxic treatment 3 years prior; blasts with complex karyotype, CD19+, CD22+, TdT+, CD10–, MPO+; subsequent relapse as AML with no B-lineage markers
CD10+, CD19±, CD79a+, TdT+, cIgM+; CD20–, CD34–; monoclonal IGH rearrangement by PCR Blasts at relapse lost TdT, partially lost CD10 and CD43; subset gained sIgM, sk Following cytotoxic therapy for breast carcinoma 1.5 years earlier History of plasma cell myeloma, cytotoxic therapy 6 years ago; 20q– History of AML, cytotoxic therapy 5 years ago; diploid karyotype History of uterine CA, DLBCL DH with cytotoxic therapy 14 years and 1 year earlier, respectively History of AML, cytotoxic therapy 3 years ago; 10.5% aberrant B lymphoblasts; complex karyotype with 2 subclones: 47,XY,+8,i(9)(q10)[cp5]/48,XY,+8,r(9) (p24q34),+21[cp2]/46,XY[13]
B-ALL in a patient with history of HLH secondary to disseminated Mycobacterium tuberculosis infection
B-ALL occurred months after the diagnosis of HLH
Refractory chronic lymphocytic leukemia B-ALL
Disease apparently cured by autologous CART-19 Treatment with CART-19
ABL1, Abl-interactor 1; ALL, acute lymphoblastic leukemia/lymphoma; AML, acute myeloid leukemia; B-ALL, B-acute lymphoblastic leukemia; BCR, breakpoint cluster region; BM, bone marrow; c, cytoplasmic; CA, carcinoma; CART-19, chimeric antigen receptor-modified T-cell therapy against CD19; CD, cluster of differentiation; CR, complete remission; CSF, cerebrospinal fluid; DH, double-hit; DLBCL, diffuse large B-cell lymphoma; DS, Down syndrome; EBF1, early B-cell factor 1; FIP1L1, factor interacting with PAPOLA and CPSF1; FISH, fluorescence in situ hybridization; FLT3, FMS-related tyrosine kinase 3; HLH, hemophagocytic lymphohistiocytosis; Ig, immunoglobulin; IGH, immunoglobulin heavy chain; IHC, immunohistochemistry; IKZF1, Ikaros family zinc finger 1; ins, insertion; ish, in situ hybridization; MLL, mixed-lineage leukemia gene; MLLT1, myeloid/lymphoid leukemia translocated to 1; MPL, proto-oncogene, thrombopoietin receptor; MPO, myeloperoxidase; MYC, myelocytomatosis viral oncogene homolog; PAX5, paired box gene 5; PCR, polymerase chain reaction; PDGFRA, platelet-derived growth factor receptor a; PDGFRB, platelet-derived growth factor receptor b; Ph, Philadelphia chromosome/t(9;22)(q34;q11.2); s, surface; SNP, single-nucleotide polymorphism; SSC, side scatter; TCR, T-cell receptor; TdT, terminal deoxynucleotidyl transferase.
396 Am J Clin Pathol 2015;144:393-410 DOI: 10.1309/AJCPAN7BH5DNYWZB
© American Society for Clinical Pathology
Downloaded from http://ajcp.oxfordjournals.org/ by guest on January 17, 2017
Significance of MPO expression in classification of acute leukemias 228 B-ALL with t(4;11)(11q23)/MLL rearrangement 410 Ph+ acute leukemia, myeloid vs mixed lineage, favor myeloid
AJCP / Review Article
A
❚Image 1❚ Philadelphia chromosome–positive B-acute lymphoblastic leukemia with IKZF1 (Ikaros) deletion. The bone marrow aspirate smears (A) showed sheets of small- to intermediate-sized blasts with finely dispersed chromatin and scant basophilic cytoplasm (Giemsa; ×500). Karyotyping by single-nucleotide polymorphism (B) demonstrated a deletion at 7p12.2, involving IKZF1 exons 6 to 12. (Case 210, courtesy of J. J. Boncher, MD, and J. R. Cook, MD, PhD.)
mature B-cell phenotypes, with expression of clonal surface light chains. One showed blastic morphology (case 118) and could be classified as B-ALL. The second case was difficult to definitively classify, since the neoplasm had Burkitt-like morphology with intermediate-sized cells containing cytoplasmic vacuoles (case 415). The review panel thought this neoplasm was best designated as a mature B-cell leukemia/ lymphoma associated with t(4;11). Additional B-ALL cases with MLL rearrangements are discussed below in the therapy-related section (cases 96 and 297) and with other neoplasms that were myeloperoxidase (MPO) positive (case 228).
© American Society for Clinical Pathology
What Are the Features of B-ALL With Associated Eosinophilia? Four cases submitted to this session (cases 104, 132, 371, and 387) were examples of B-ALL with associated myeloid proliferations. Four of these patients had eosinophilia. In general, the presence of eosinophilia occurring with B-ALL raises several diagnostic possibilities, including but not limited to B-ALL associated with t(5;14) (q31;q32); lymphoid neoplasms with abnormalities of PDGFRA, PDGFRB, or FGFR1; and lymphoid blast crisis of CML. It is important to appropriately identify Ph+ cases and those with PDGFRA or PDGFRB abnormalities
Am J Clin Pathol 2015;144:393-410 397 DOI: 10.1309/AJCPAN7BH5DNYWZB
Downloaded from http://ajcp.oxfordjournals.org/ by guest on January 17, 2017
B
Loghavi et al / B-ALL/Lymphoblastic Lymphoma
B
A
250
Myeloid
150
CD34 APC-A
SSC-H (×1,000)
200 Monos
100 50
Blasts
10
5
10
4
10
3
10
2
Q1-2
Q2-2
Q3-2
Q4-2
Lymphs 2
3
4
5
2
10
5
10
4
10 10
2
3
4
5
4
5
10 10 10 CD117 PE-A
5
10
Q1-2 3
10
Q3-2
2
10
CD11b APC-A
CD19 APC-A
10 10 10 10 CD45 PerCP-A
❚Image 2❚ B-acute lymphoblastic leukemia with associated MLL rearrangement. The bone marrow core biopsy specimen (A) shows sheets of immature blasts. Fluorescence in situ hybridization studies (B) showed loss of a 3′ MLL signal (red) in 123 of 200 cells. Flow cytometry immunophenotyping (C) showed a characteristic aberrant lymphoblast phenotype, positive for CD19, CD15, and CD34 (partial) and negative for CD10. FITC, fluorescein isothiocyanate; PE, phycoerythrin; SSC, side scatter. Case 235, courtesy of J. C. Gomez-Gelvez, MD, and colleagues.)
Q2-2
Q4-2
3
4
5
10 10 10 CD10 PE-A
4
10
Q1-2
Q2-2
Q3-2
Q4-2
3
10
2
10
2
10
3
10 10 10 CD15 FITC-A
because these patients are often responsive to TKI therapy.51,52 Thus, in patients with nonreactive eosinophilia, in addition to conventional cytogenetic analysis, fluorescence in situ hybridization (FISH) studies are recommended to identify FIP1L1-PDGFRA fusions and reciprocal translocations involving PDGFRA (4q12), PDGFRB (5q31-q33), and FGFR1 (8p11-13).53 Among the cases discussed at the workshop, two (cases 104 and 132) demonstrated the t(5;14)(q31;q32) translocation, resulting in juxtaposition of the promoter region of the interleukin-3 (IL-3) gene on chromosome 5 and the IGH gene on chromosome 14.54 In a third patient (case 371), the t(5;14)(q31;q32) was suspected and IGH rearrangement
398 Am J Clin Pathol 2015;144:393-410 DOI: 10.1309/AJCPAN7BH5DNYWZB
was detected by FISH, but conventional cytogenetics were negative for t(5;14)(q31;q32), and IL-3 was not tested by FISH. Cases with t(5;14)(q31;q32) are rare, may affect children and adults, and have variable degrees of eosinophilia. The eosinophilic proliferation is thought to be nonclonal and results from increased IL-3 levels. The neoplastic lymphoblasts typically exhibit a precursor B-cell immunophenotype characterized by CD10 and CD19 expression. Patients with ALL are generally acutely ill and commonly have peripheral blood cytopenias (anemia and/or thrombocytopenia). In addition, the presence of any degree of eosinophilia (above high normal range) ❚Image 3❚, along with any number of lymphoblasts (CD19+/CD10+) identified by FC
© American Society for Clinical Pathology
Downloaded from http://ajcp.oxfordjournals.org/ by guest on January 17, 2017
C
AJCP / Review Article
A
B
immunophenotyping, should prompt a workup to exclude this disease entity. The t(5;14)(q31;q32) is leukemia defining, since there is no minimum required blast count to establish the diagnosis of ALL once this karyotypic abnormality is confirmed. The presence of eosinophilia in case 387 was unexplained. In this neoplasm, there was evidence of IGH rearrangement by FISH, but no abnormalities were detected in PDGFRA, PDGFRB, FGFR1, MLL, IL-3, or BCR-ABL1 fusion. Case 102 was unusual since this 64-year-old man had leukocytosis of 51.3 × 109/L, left-shifted neutrophils, moderate monocytosis, and 2% blasts in the blood smear. The diagnosis of B-ALL was established by BM examination. Three months following chemotherapy, the patient’s BM was hypercellular with atypical megakaryocytes and clustering of megakaryocytes. The diagnosis of concurrent B-ALL and a myeloproliferative neoplasm with MPL p.W515S point mutation, suggestive of a prefibrotic phase of primary myelofibrosis, was established. Whether the B-ALL was a form of leukemic transformation of the preceding myeloproliferative neoplasm or represents a secondary malignancy is unclear. What Is the Importance of a Hypodiploid Karyotype in B-ALL? Hypodiploidy has unfavorable prognostic implications in patients with B-ALL, and therefore identification of hypodiploidy is important.55 One case was submitted to this session. Case 11 was from a 10-year-old boy with B-ALL with a hypodiploid karyotype. The karyotype was initially
© American Society for Clinical Pathology
thought to be a possible hyperdiploid karyotype on conventional cytogenetic studies, due to duplication of the hypodiploid clone. In this case, single-nucleotide polymorphism array analysis was performed, which unveiled the masked hypodiploid karyotype. TdT+ B-Cell Neoplasms With BCL2 and/or MYC Alterations: What Is the Best Classification? Five cases of TdT+ B-cell neoplasms with BCL2 rearrangements, MYC rearrangements, or both were discussed in this session. Four patients had high-grade neoplasms at presentation (cases 149, 159, 301, and 338), and the fifth patient (case 369) had a complicated clinical course that needs more explanation. This patient initially had a lowgrade follicular lymphoma, followed 2 years later by highgrade B-cell lymphoma with a mature immunophenotype with FISH positive for both BCL2 and MYC rearrangements (“double hit”). One year later, the patient had a blastic TdT+ neoplasm involving BM and a retroperitoneal mass, and these were the specimens submitted to the session. Overall, four of these neoplasms showed BCL2 gene rearrangements by FISH and/or conventional karyotyping, two of which had MYC rearrangement, and a third case had BCL2, MYC, and BCL6 rearrangement (“triple hit”). One case had only a MYC rearrangement. All patients presented in a distinctive and similar manner with large abdominal/retroperitoneal masses and replacement of the BM by sheets of blasts. The blasts in all cases were intermediate to large in size, with varying amounts of cytoplasm from case to case ❚Image 4❚.
Am J Clin Pathol 2015;144:393-410 399 DOI: 10.1309/AJCPAN7BH5DNYWZB
Downloaded from http://ajcp.oxfordjournals.org/ by guest on January 17, 2017
❚Image 3❚ B-acute lymphoblastic leukemia with t(5;14)(q31;q32) and hypereosinophilia. A peripheral blood specimen (A) showed marked leukocytosis (WBC count, 136 K/mL) with hypereosinophilia (Giemsa, ×500). The bone marrow aspirate smear (B) showed markedly increased blasts and an increase in mature-appearing eosinophils (Giemsa, ×500). The blasts had an immature B-cell phenotype by flow cytometry. (Case 132, courtesy of Y. Pang, MD, and colleagues.)
Loghavi et al / B-ALL/Lymphoblastic Lymphoma
A
B
C
Prominent vacuoles were seen in one double-hit case and one case with only BCL2 rearrangement. All tumors were positive for CD10, CD19, and TdT; negative or only partially positive for CD34; negative or only dimly positive for CD20; and negative for surface immunoglobulins. Case 159 also had a distinct small subset of mature B cells detectable by FC, positive for CD20 and surface immunoglobulin and negative for CD10 and TdT. Immunohistochemical studies performed on the BM biopsy specimen showed a CD20+ peri- to paratrabecular infiltrate. In case 369, there is strong evidence for transformation of a mature high-grade B-cell lymphoma to a blastic TdT+ neoplasm, with shared cytogenetic aberrations in both specimens. In case 159, there is also morphologic and immunophenotypic evidence strongly suggesting an underlying low-grade B-cell lymphoma, possibly follicular lymphoma. Blastic transformation of follicular lymphoma is a rare event but has been recognized for more than 25 years.56-58 While many cases reported since have shown blastic morphology but a mature immunophenotype, a few cases have shown a true precursor B-cell phenotype, positive for TdT and usually negative for CD20 and surface light chains.56,57,59-64 Most of these cases had double-hit cytogenetics, with rearrangements of both BCL2 and MYC genes. Patients with these neoplasms have a highly aggressive course, with all reported survival durations of less than 1 year.
400 Am J Clin Pathol 2015;144:393-410 DOI: 10.1309/AJCPAN7BH5DNYWZB
The pathogenesis of lymphoblastic transformation of follicular lymphoma is not well understood. The t(14;18) translocation breakpoints in follicular lymphomas show evidence of recombinase and TdT activity, implying origin in an immature B-cell precursor in the BM (reviewed by Kridel et al65). In one scenario, secondary genetic transforming events take place in a residual immature lymphoma precursor cell, which retains its lymphoblastic phenotype.66 In an alternative model, secondary genetic events occur in mature follicular lymphoma cells, leading to “dedifferentiation” with reactivation of an immature immunophenotype. In two reported cases, the transformed lymphoblasts showed somatic hypermutation of their IGH variable region (V) sequences.60,62 These IGHV sequence changes were shared by both the original follicular lymphoma and the lymphoblasts. This finding strongly suggests that in at least some cases, follicular lymphoma may transform by dedifferentiation to a lymphoblastic phenotype. De novo B-ALL with t(14;18)(q32;q21) has also been long recognized.67 Cases with a well-documented immature immunophenotype, including TdT expression, are rare.58,67-79 These tumors share many similarities with follicular lymphoma with lymphoblastic transformation, including frequent association with MYC translocations and a very poor prognosis. Hardianti et al76 demonstrated somatic hypermutation of IGHV gene sequences in three
© American Society for Clinical Pathology
Downloaded from http://ajcp.oxfordjournals.org/ by guest on January 17, 2017
❚Image 4❚ TdT+ blastic B-cell neoplasms with MYC and/or BCL2 rearrangements. Bone marrow (BM) aspirate smears (A) of a case with MYC, BCL2, and BCL6 rearrangements by fluorescence in situ hybridization (FISH) showed large blastic cells with highly irregular nuclear contours, fine chromatin, and scant cytoplasm (Giemsa, ×500). BM aspirate smears (B) of a case with MYC and BCL2 rearrangements by FISH showed large neoplastic cells with round nuclei, fine chromatin, and small amounts of occasionally vacuolated cytoplasm. BM touch imprints (C) of a case with only a BCL2 rearrangement by FISH showed large neoplastic cells with fine chromatin, prominent nucleoli, and vacuolated basophilic cytoplasm (Giemsa, ×500). All had an immature phenotype, including TdT positivity. (A, case 159, courtesy of E. Torlakovic, MD, PhD, and colleagues; B, case 301, courtesy of M. Nakashima, MD, and colleagues; C, case 338, courtesy of N. J. Mason, MD, and colleagues.)
AJCP / Review Article
B-ALL Not Otherwise Specified (Normal Karyotype) A single case in this category was submitted to this session. Case 321 was from a 17-year-old girl who developed B-ALL with a diploid karyotype. Of interest, the lymphoblasts were studied by gene expression profiling that showed high levels of FMS-related tyrosine kinase 3, as well as high expression of “outlier” genes. The overall profile was similar to those seen in what is known as “cluster group 5,” which has been associated with a more favorable prognosis,81 and this patient was in remission 5 years after diagnosis. This case highlights the value of gene expression profiling in diploid cases of B-ALL.
© American Society for Clinical Pathology
Issues in Immunophenotyping of B-ALL How Does One Distinguish B-ALL From Normal Counterparts by FC? Several cases in this session demonstrated the utility of FC immunophenotyping to distinguish aberrant B-ALL lymphoblasts from their benign counterparts in the BM. CD10+ B-cell precursors, termed hematogones based on their immature-appearing morphology, have a well-characterized immunophenotype notable for a spectrum of expression of several markers during maturation. Multiple studies have characterized the profile of hematogones and highlighted common immunophenotypic aberrancies associated with B lymphoblasts.21,48,82-95 Aberrant blasts may express antigens from an inappropriate cell lineage (eg, myeloid antigens), but it is often more informative to identify altered levels of expression of antigens that are normally expressed on hematogones. Case 142 was from a patient with treated B-ALL who had 4% residual aberrant blasts by FC immunophenotyping on follow-up BM examination. The diagnosis was difficult, since the blast immunophenotype largely overlapped with a hematogone profile with expression of CD10, CD19, CD20, CD34, CD38, and TdT. However, the blasts did show aberrantly increased CD58 expression, demonstrating the utility of an extended minimal residual disease–targeted panel. Case 152 was from a patient who initially had cytopenias and an oligoblastic picture, with only 6% aberrant BM blasts identified by FC immunophenotyping, on the basis of decreased CD45 and increased CD10 expression. Within 6 weeks, this patient developed overt ALL with 80% blasts on a subsequent BM examination. Case 178 was from an adult patient treated for B-ALL; follow-up BM smears showed about 50% morphologically atypical cells suspicious for residual disease ❚Image 5❚. However, FC analysis clearly demonstrated a benign immunophenotype characteristic of regenerating hematogones. Increased hematogones may be seen in healthy children, in response to peripheral cytopenias, and in BM recovery in patients who have undergone chemotherapy or stem cell transplant. Does MPO Expression Occur in B-ALL, and What Is Its Importance? MPO can be present in rare cases of B-ALL, in contrast with the 2008 World Health Organization classification guidelines, which state that MPO expression, together with strong evidence of B-lineage differentiation, is sufficient to classify a case as mixed-phenotype acute leukemia (MPAL).96 MPO detection can be performed by cytochemistry, FC, and/or immunohistochemistry (IHC), and 3% and 10% cutoffs have been used historically as thresholds for MPO positivity by cytochemistry and FC, respectively.97,98
Am J Clin Pathol 2015;144:393-410 401 DOI: 10.1309/AJCPAN7BH5DNYWZB
Downloaded from http://ajcp.oxfordjournals.org/ by guest on January 17, 2017
TdT+ cases, at high rates comparable to follicular lymphomas. In addition, two TdT+ cases in that series showed continuing expression of activation-induced cytidine deaminase (AID). Both the presence of somatic hypermutation and AID expression are strongly associated with mature germinal center B-cell differentiation. These findings suggest a distinct pathogenetic mechanism in at least a subset of cases with t(14;18), in comparison to cases of B-ALL with more typical translocations. These cases also raise the possibility of a history of subclinical follicular lymphoma in these patients. Overall, compared with typical B-ALL/LBL, cases of blastic transformation of follicular lymphoma and de novo lymphoblastic cases associated with t(14;18) show distinctive clinical features, including a poor prognosis, and likely a different pathogenesis. In the opinion of the consensus panel, classifying these cases as B-ALL or B-LBL without further comment could be misleading to clinicians and patients. The consensus of the review panel and participants in this session thought a descriptive diagnosis was more appropriate, such as “high-grade TdT-positive blastic B-cell leukemia/ lymphoma,” and classified cases 159, 301, 338, and 369 as such. If there is a history of follicular lymphoma or evidence for underlying lower grade lymphoma, this should be clearly indicated. A history of lymphoma, extensive lymphadenopathy, or unusual immunophenotype or morphology in a TdT+ B-lineage neoplasm should prompt suspicion and appropriate workup. We recommend FISH to assess for the presence of MYC and BCL2 rearrangements in such cases. MYC gene rearrangements rarely may be observed in B-ALL/LBL in the absence of t(14;18) translocation (recently reviewed by Seo et al80). While the detection of an MYC gene rearrangement may have therapeutic implications, particularly for children on cooperative trials, the prognostic implications are not as clear. The panel classified case 149 as B-ALL with t(8;22)(q24.1;q11.2).
Loghavi et al / B-ALL/Lymphoblastic Lymphoma
B
C
D 10
3
768
10
256 0 0 10
2
10
1
10
0
2
3
10 10 10 CD45-PC5
10
4
512 256
10 1
3
CD10-PE
CD10-PE
10
SS Lin
768
SS Lin
1,024
10
512
4
4
1,024
0
10
1
2
3
10 10 10 CD20-FITC
10
4
0 0 10
2
10
1
10
0
10 1
2
10 10 10 CD45-PC5
3
10
4
0
10
1
2
3
10 10 10 CD20-FITC
4
10
❚Image 5❚ Hematogone hyperplasia in a patient treated for B-acute lymphoblastic leukemia (B-ALL). A bone marrow aspirate at diagnosis of B-ALL (A) showed sheets of lymphoblasts (Giemsa, ×500). The bone marrow aspirate at the end of therapy (B) showed 52% lymphoid cells, some with immature-appearing chromatin concerning for residual blasts (Giemsa, ×500). Flow cytometry immunophenotyping of the blasts at presentation (C) showed CD45 dim cells with bright CD10 and dim CD20 expression. The B-lineage cells at the end of therapy (D) showed normal levels of CD10 in a subset, with an unremarkable spectrum of CD20 expression, consistent with benign regenerating hematogones. FITC, fluorescein isothiocyanate; SS, side scatter. (Case 178, courtesy of D. Grier, MD.)
In a recent study, Guy et al99 proposed a refined threshold of 13% or 28% MPO positivity (using either isotype controls or normal lymphocytes as negative controls) to establish myeloid differentiation by FC immunophenotyping. However, MPO stains by either IHC or FC can be difficult to quantify and are prone to technical artifacts. Borowitz100 has recently published his opinion that MPO positivity as the sole myeloid feature in an otherwise typical ALL should be considered skeptically and may not be sufficient for a diagnosis of MPAL. Three cases with MPO expression were discussed in this session. Case 228 was an acute leukemia with a t(4;11)(11q23) MLL rearrangement, and the blasts had a typical MLL-associated B-ALL immunophenotype (CD10–,
402 Am J Clin Pathol 2015;144:393-410 DOI: 10.1309/AJCPAN7BH5DNYWZB
CD15+, CD19+, TdT+). The neoplastic cells were positive for MPO by IHC ❚Image 6❚ (confirmed with repeat staining by the consensus panel), but MPO expression was not detected by FC immunophenotypic analysis. This discordance appears to further weaken the significance of the MPO staining, and the panel concurred with the submitting diagnosis of B-ALL. Case 410 was a Ph+ acute leukemia that expressed several myeloid markers, including MPO (on a subset of blasts in the cerebrospinal fluid). Blasts in the BM showed strong CD19 expression but no other B-lineage markers, and those in the cerebrospinal fluid were CD22+TdT+ but CD19–. Overall, the number of concurrently expressed B-lineage markers did not appear to definitively support a diagnosis of
© American Society for Clinical Pathology
Downloaded from http://ajcp.oxfordjournals.org/ by guest on January 17, 2017
A
AJCP / Review Article
A
B
MPAL. This case highlights the propensity for Ph+ leukemias to express markers from multiple lineages. Case 98 was a therapy-related leukemia with a complex karyotype and predominantly B-antigen expression (CD19+CD22+TdT+ but CD10–) at presentation. Immunohistochemical staining showed strong coexpression of MPO, consistent with MPAL. After therapy, the patient had a recurrence with acute myeloid leukemia (AML), showing no B-lineage marker expression. It has been well established that cases of MPAL can exhibit phenotypic shift over time following therapy or at relapse and may recur as either AML or ALL.96,101-103 Other Unusual Immunophenotypic Findings in B-ALL Case 128 was a B-ALL with a normal karyotype and an unusual immunophenotype with minimal expression of CD19 but positive for the B-lineage–associated antigens cCD79a+ and cIgM+. Reduced expression levels of CD19 may be seen in a subset of cases of B-ALL (~16%19%),21,87,89 but significant loss of CD19 is rare. However, awareness of such cases is important because many laboratories rely on CD19 expression in the initial identification of potential B lymphoblasts. Case 260 is an example of B-ALL with phenotypic shift at relapse, with loss of immature markers (TdT) and gain of more mature B-lineage markers (surface IgM k) on a subset. Loss and gain of antigens at relapse B-ALL is well known, with loss of CD10, CD20, and/or myeloid antigens and gain of CD20 representing the most common changes.92,104 Antigenic shifts also may manifest as altered intensity of
© American Society for Clinical Pathology
previously expressed antigens. Several possible mechanisms have been proposed that may explain these phenomena: (a) occurrence of a second clonally unrelated leukemia; (b) presence of minor subclones at diagnosis, which are more chemoresistant than the dominant clone and become the prevailing blast populations at relapse; or (c) a phenotypic switch due to gain of additional genetic aberrancies in the course of disease progression.92
Unusual Clinical Presentations Is Therapy-Related B-Acute Lymphoblastic Leukemia/Lymphoma a Distinct Entity? Four cases of therapy-related ALL (t-ALL) were submitted to the workshop (cases 96, 157, 297, and 336). One patient had a history of a solid tumor (breast carcinoma), two had been treated for hematopoietic neoplasms (plasma cell myeloma and AML), and one patient had a history of both uterine carcinoma and diffuse large B-cell lymphoma. The patients all had received cytotoxic chemotherapy, starting between 1 and 6 years prior to the diagnosis of B-ALL. The patient with t-ALL after breast carcinoma ❚Image 7❚ had also received adjuvant radiotherapy. Two patients had t(4;11) involving the MLL locus, and both had received anthracycline-containing regimens within the preceding 12 to 18 months. The patient with myeloma received intensive chemotherapy, including alkylating agents, anthracyclines,
Am J Clin Pathol 2015;144:393-410 403 DOI: 10.1309/AJCPAN7BH5DNYWZB
Downloaded from http://ajcp.oxfordjournals.org/ by guest on January 17, 2017
❚Image 6❚ B-acute lymphoblastic leukemia with t(4;11) involving 11q23, positive for myeloperoxidase (MPO) by immunohistochemistry. A bone marrow core biopsy specimen showed sheets of blasts on H&E stains (A, ×400), with a subset positive for MPO (B, ×200). By flow cytometry, the blasts were positive for CD19 and CD79a, with aberrant expression of CD15. They were negative for CD10, as well as for MPO and all other myeloid antigens tested (CD13, CD33, and CD117). (Case 228, courtesy of J. A. Arias-Stella, MD, and colleagues.)
Loghavi et al / B-ALL/Lymphoblastic Lymphoma
A
B
and etoposide, and 5 years later developed B-ALL with an aberrant karyotype, including a del(20q). The patient with AML received standard chemotherapy and 5 years later had B-ALL with a normal karyotype. One additional patient (case 429) had a history of AML with normal cytogenetics, with relapse 3 years later. Subsequent BM examination over the next year showed persistent myeloid blasts ranging from 4% to 9% of cellularity, with a complex karyotype including clones with trisomy 8 and either isochromosome 9q or ring chromosome 9. A BM aspirate and biopsy specimen 5 years after initial therapy showed a distinct population of aberrant B-lymphoid blasts with no myeloid markers (10.5% of cells). The karyotype was complex and included aberrant clones similar to those observed in previous biopsy specimens. The overall findings suggest evolving therapy-related B-ALL but could represent persistence/recurrence of the original AML, with a lineage shift possibly due to clonal evolution. t-ALL, defined as acute lymphoblastic leukemia arising in the setting of prior chemotherapy and/or radiation therapy, is uncommon compared with de novo disease and represents approximately 12% of all therapy-related leukemias and less than 5% of all adult acute lymphoblastic leukemias. The age of onset is older in t-ALL in comparison to de novo disease, with a reported range of 15 to 94 years.105-109 Primary sites include solid organs and the hematopoietic system.106,108-110 The median latency interval ranges from 19 to 72 months in various studies, depending on the clinical setting and the genetic abnormalities.108,110,111 Underlying dysplasia may be seen in a subset of cases,110 although this may be difficult to appreciate in a typical BM packed with blasts.
404 Am J Clin Pathol 2015;144:393-410 DOI: 10.1309/AJCPAN7BH5DNYWZB
The most common genetic abnormities encountered in the setting of t-ALL are t(4;11)(q21;q23) resulting in an MLL/AF4 fusion, followed by the Ph and hypodiploidy, commonly involving chromosomes 5, 7, and 17.106,110-112 Normal karyotypes may be seen in a minority of cases.108 As observed in therapy-related myeloid neoplasms, MLL rearrangements in t-ALL are most commonly seen following exposure to topoisomerase II inhibitors.110,113 Hypodiploidy is frequently associated with alkylating agents.110 While MLL may be seen with numerous fusion partners in both de novo ALL and in therapy-related myeloid neoplasms, this gene typically is partnered with AF4 in t-ALL, although other rare translocations involving the MLL gene have been described.111 Most cases of t-ALL are of B lineage, and those cases with MLL rearrangements typically show the MLL-associated immunophenotype described above.106 Cases of t-ALL with hypodiploidy are often positive for CD20 as well as CD10.106,110 Patients with t-ALL have a significantly poorer outcome compared with patients with de novo disease, and the median survival of patients with t-ALL is less than 1 year.107,108 Comparison with historical controls suggests that patients with t-ALL have a worse prognosis than do adult patients with de novo B-ALL with similar cytogenetic alterations such as MLL/AF4 fusions.4,107 However, a recent comparison of patients with t-ALL and de novo ALL treated at a single institution found that karyotype but not prior cytotoxic therapy was an independent prognostic indicator in multivariate analysis.110 Thus, it remains an open question if t-ALL should be classified as a distinct entity or whether its distinctive clinical features are due primarily to
© American Society for Clinical Pathology
Downloaded from http://ajcp.oxfordjournals.org/ by guest on January 17, 2017
❚Image 7❚ Therapy-related B-acute lymphoblastic leukemia with t(4;11)(q21;q23). The bone marrow aspirate smear (A) showed intermediate-sized blasts with variable amounts of basophilic cytoplasm (Giemsa, ×500). Cytogenetic studies (B) demonstrated the aberrant karyotype. (Case 297, courtesy of G. Tang, MD, PhD, and S. A. Wang, MD.)
AJCP / Review Article
its association with poor-risk cytogenetics, as well as with older age at presentation.
Novel Therapy Chimeric Antigen Receptor-Modified T-Cell Therapy Against CD19 (CART-19) Chimeric antigen receptor T cells (CARTs) are genetically engineered cells, usually obtained from the patient’s peripheral blood, that express receptors capable of specifically binding to tumor-associated antigens. Chimeric antigen receptors (CARs) are fusion proteins composed of an antigen recognition moiety, usually a monoclonal antibody variable region, and costimulatory (ie, CD28 and 4-1BB) and T-cell activation domains (ie, CD3 ζ). In contrast to T-cell receptors, CARs recognize and bind to cell surface antigens and can be used to treat patients irrespective of human leukocyte antigen type (reviewed by Kochenderfer and Rosenberg125). The pan–B-cell antigen CD19 is an attractive target for using this technique in the treatment of B-cell malignancies. Kochenderfer et al126 demonstrated for the first time dramatic in vivo response to anti-CD19 CARTs in patients
© American Society for Clinical Pathology
Summary In summary, we highlight some key points raised in the workshop and discussed in this review, with a focus on the diagnostic workup of B-ALL/LBL: 1. Deletions and other alterations in the IKZF1 (Ikaros) gene are adverse prognostic indicators, in both Ph+ and Ph– patients with B-ALL. Particularly if targeted therapy becomes available, analysis of this locus may become important in the initial workup of B-ALL. 2. ALL associated with MLL gene rearrangements has a characteristic immunophenotype, CD10– with aberrant expression of CD15, that may provide the first clue to the presence of this poor-prognosis cytogenetic aberration. 3. We recommend evaluation for B-ALL in the diagnostic workup of patients with hypereosinophilia. Conventional cytogenetics, FISH, and/or polymerase chain reaction should be employed to exclude B-ALL with t(5;14)(q31;q32); lymphoid neoplasms with abnormalities of PDGFRA, PDGFRB, or FGFR1; and lymphoid blast crisis of CML. 4. Consider FISH analysis for BCL2 and MYC aberrancies in apparent ALL cases with extensive lymphadenopathy or in patients with a history of lymphoma. A subset of these cases may represent high-grade transformation of mature B-cell lymphomas. In cases with BCL2 rearrangement, we do not recommend the diagnosis of B-ALL/LBL and suggest an alternative descriptive diagnosis such as high-grade TdT+ blastic B-cell leukemia/lymphoma. 5. Hematogones may be markedly increased in BM specimens during early recovery following chemotherapy or stem cell transplant in ALL. FC immunophenotyping can reliably distinguish hematogones from residual ALL blasts. 6. We advocate assessing MPO expression in all new acute leukemias by at least two techniques, including cytochemistry. In a B-ALL with an otherwise typical phenotype, MPO positivity by FC and/or IHC does not always indicate a diagnosis of MPAL. 7. Therapy-related ALL in patients with prior chemotherapy or radiation therapy is often associated with poorprognosis cytogenetic aberrancies, frequently with t(4;11) (q21;q23)/MLL/AF4. It is unclear whether prior therapy is an independent poor prognostic factor.
Am J Clin Pathol 2015;144:393-410 405 DOI: 10.1309/AJCPAN7BH5DNYWZB
Downloaded from http://ajcp.oxfordjournals.org/ by guest on January 17, 2017
B-ALL Associated With Hemophagocytic Lymphohistiocytosis Case 259 was from a patient with B-ALL arising in the setting of hemophagocytic lymphohistiocytosis (HLH; also known as infection-associated hemophagocytic syndrome) secondary to disseminated Mycobacterium tuberculosis infection. In this patient, B-ALL occurred several months after the diagnosis of HLH. This is a rare phenomenon, most commonly observed in the pediatric population. The association of HLH and ALL has been well described,114-123 but unlike the case submitted to the workshop, in most reported cases, the diagnosis of ALL preceded HLH. In many cases, HLH has been associated with a concurrent infectious etiology, possibly due to immune deficiency following chemotherapy or stem cell transplantation for ALL, and in these patients, the term infection-associated hemophagocytic syndrome may be more appropriate. HLH-associated ALL can be of B or T lineage, although most reported cases were T-ALL. The prognosis of these patients is often poor. If untreated, most patients with HLH will succumb to their disease within approximately 2 months. Although the diagnostic criteria for HLH are mostly clinical and laboratory dependent,124 early identification of hemophagocytosis on BM examination can trigger appropriate workup and timely diagnosis, resulting in prompt immunosuppressive therapy.124 Based on our review of the literature, it also seems that the term HLH is used differently by different authors, and criteria need to be refined.
with advanced-stage follicular lymphoma. Several clinical trials have been since conducted employing CART-19 in treating refractory B-cell lymphomas/leukemias of various subtypes, mostly in patients with chronic lymphocytic leukemia127-129 (case 264), but also including a single patient with B-ALL.130 Case 224 was from a patient with multiply relapsed B-ALL with a complex karyotype, successfully treated with CART-19.
Loghavi et al / B-ALL/Lymphoblastic Lymphoma
References 1. Borowitz MJ, Chan JKC. B lymphoblastic leukaemia/ lymphoma, not otherwise specified. In: Swerdlow SH, Campo E, Harris NL, et al, eds. World Health Organization Classification of Tumours of Haematopoietic and Lymphoid Tissues. 4th ed. Lyon, France: IARC Press; 2008:168-170. 2. Preti HA, O’Brien S, Giralt S, et al. Philadelphiachromosome–positive adult acute lymphocytic leukemia: characteristics, treatment results, and prognosis in 41 patients. Am J Med. 1994;97:60-65. 3. Faderl S, Kantarjian HM, Talpaz M, et al. Clinical significance of cytogenetic abnormalities in adult acute lymphoblastic leukemia. Blood. 1998;91:3995-4019. 4. Moorman AV, Harrison CJ, Buck GA, et al. Karyotype is an independent prognostic factor in adult acute lymphoblastic leukemia (ALL): analysis of cytogenetic data from patients treated on the Medical Research Council (MRC) UKALLXII/Eastern Cooperative Oncology Group (ECOG) 2993 trial. Blood. 2007;109:3189-3197. 5. Ottmann OG, Wassmann B, Hoelzer D. Imatinib for relapsed BCR/ABL positive leukemias. Ann Hematol. 2002;81(suppl 2):S36-S37. 6. Wassmann B, Pfeifer H, Scheuring U, et al. Therapy with imatinib mesylate (Glivec) preceding allogeneic stem cell transplantation (SCT) in relapsed or refractory Philadelphiapositive acute lymphoblastic leukemia (Ph+ALL). Leukemia. 2002;16:2358-2365.
406 Am J Clin Pathol 2015;144:393-410 DOI: 10.1309/AJCPAN7BH5DNYWZB
7. Schultz KR, Bowman WP, Aledo A, et al. Improved early event-free survival with imatinib in Philadelphia chromosome–positive acute lymphoblastic leukemia: a Children’s Oncology Group study. J Clin Oncol. 2009;27:5175-5181. 8. Ravandi F, O’Brien S, Thomas D, et al. First report of phase 2 study of dasatinib with hyper-CVAD for the frontline treatment of patients with Philadelphia chromosome– positive (Ph+) acute lymphoblastic leukemia. Blood. 2010;116:2070-2077. 9. Pfeifer H, Wassmann B, Pavlova A, et al. Kinase domain mutations of BCR-ABL frequently precede imatinib-based therapy and give rise to relapse in patients with de novo Philadelphia-positive acute lymphoblastic leukemia (Ph+ ALL). Blood. 2007;110:727-734. 10. Iacobucci I, Ferrari A, Lonetti A, et al. CDKN2A/B alterations impair prognosis in adult BCR-ABL1–positive acute lymphoblastic leukemia patients. Clin Cancer Res. 2011;17:7413-7423. 11. Hu Y, Liu Y, Pelletier S, et al. Requirement of Src kinases Lyn, Hck and Fgr for BCR-ABL1–induced B-lymphoblastic leukemia but not chronic myeloid leukemia. Nat Genet. 2004;36:453-461. 12. Li S. Src-family kinases in the development and therapy of Philadelphia chromosome–positive chronic myeloid leukemia and acute lymphoblastic leukemia. Leuk Lymphoma. 2008;49:19-26. 13. Frank DA, Varticovski L. BCR/abl leads to the constitutive activation of Stat proteins, and shares an epitope with tyrosine phosphorylated Stats. Leukemia. 1996;10:17241730. 14. Ilaria RL Jr, Van Etten RA. P210 and P190(BCR/ABL) induce the tyrosine phosphorylation and DNA binding activity of multiple specific STAT family members. J Biol Chem. 1996;271:31704-31710. 15. Verma D, Kantarjian HM, Jones D, et al. Chronic myeloid leukemia (CML) with P190 BCR-ABL: analysis of characteristics, outcomes, and prognostic significance. Blood. 2009;114:2232-2235. 16. Lombardo LJ, Lee FY, Chen P, et al. Discovery of N-(2chloro-6-methyl- phenyl)-2-(6-(4-(2-hydroxyethyl)piperazin-1-yl)-2-methylpyrimidin-4- ylamino)thiazole-5carboxamide (BMS-354825), a dual Src/Abl kinase inhibitor with potent antitumor activity in preclinical assays. J Med Chem. 2004;47:6658-6661. 17. Ottmann O, Dombret H, Martinelli G, et al. Dasatinib induces rapid hematologic and cytogenetic responses in adult patients with Philadelphia chromosome positive acute lymphoblastic leukemia with resistance or intolerance to imatinib: interim results of a phase 2 study. Blood. 2007;110:2309-2315. 18. Lilly MB, Ottmann OG, Shah NP, et al. Dasatinib 140 mg once daily versus 70 mg twice daily in patients with Ph-positive acute lymphoblastic leukemia who failed imatinib: results from a phase 3 study. Am J Hematol. 2010;85:164-170. 19. Paietta E, Racevskis J, Neuberg D, et al. Expression of CD25 (interleukin-2 receptor alpha chain) in adult acute lymphoblastic leukemia predicts for the presence of BCR/ABL fusion transcripts: results of a preliminary laboratory analysis of ECOG/MRC Intergroup Study E2993. Eastern Cooperative Oncology Group/ Medical Research Council. Leukemia. 1997;11:18871890.
© American Society for Clinical Pathology
Downloaded from http://ajcp.oxfordjournals.org/ by guest on January 17, 2017
Corresponding author: Jeffrey L. Jorgensen, MD, PhD, Dept of Hematopathology, The University of Texas MD Anderson Cancer Center, 1515 Holcombe Blvd, Houston, TX 77030; jljorgen@ mdanderson.org. Acknowledgments: The following were contributors or co-contributors of cases to this session: D. Alapat, B. Alobeid, S. Z. Al-Quran, B. Aqil, J. A. Arias-Stella, T. Arquero, E. Askari, H. Aviv, A. Bagg, N. A. Bakshi, M. G. Bayerl, A. Behdad, G. Bhagat, S. Bhagavathi, J. Biegel, J. J. Boncher, S. A. Brooks, A. Cazorla, Q. Chen, J. R. Cook, K. Craddock, F. E. Craig, C. V. Curry, M. Djokic, J. Echeverry, M. T. Elghetany, H. L. Evans, A. Ewton, D. Fix, T. Gindin, J. C. Gomez-Gelvez, M. C. Gonzalez, R. J. Greiner, D. D. Grier, S. A. Grupp, E. D. Hsi, D. Hoehn, M. T. Howard, J. D. Hoyer, M. Hudspeth, K. HuntKarner, S. Hussein, K. Inamdar, M. Jamali, J. L. Jorgensen, C. H. June, M. Kalos, R. P. Ketterling, J. Khoury, R. L. King, S. Konoplev, J. Lancet, J. Lazarchick, B. L. Levine, M. R. Lewis, Y. Li, J. L. Lopez Lorenzo, K. Maeda, N. J. Mason, A. M. Medina, E. A. Medina, N. Miller, L. Moscinski, M. O. Nakashima, J. L. Oliveira, S. L. Ondrejka, R. Orduz, T. M. Owidah, M. E. Paessler, C. Pang, Y. Pang, P. Papenhausen, E. P. Pareja, M. A. Perez Saenz, M. Pettenati, M. R. Pinilla, D. L. Porter, A. Porwit, C. Ramirez, A. M. Raza, K. K. Reichard, M. D. Reis, H. J. Rogers, M. Sathanoori, C. Serrano, Q. Shen, R. F. Siddiqui, P. L. Sillero, M. Simmons, G. Simona Ene, Z. Singh, L. Smith, C. Soto de Ozaeta, G. Tang, J. Tao, K. S. Theil, E. E. Torlakovic, H. Tsui, M. T. Urrego, M. A. Vasef, F. Vega-Vazquez, T. Villaescusa, D. Viswanatha, C. U. Walter, S. Wang, W. Wang, G. Wertheim, C. L. Willman, C. S. Wilson, D. Wolff, R. R. Xian, M. Zapata, L. Zhang, and X. Zhang.
AJCP / Review Article
© American Society for Clinical Pathology
35. van der Veer A, Waanders E, Pieters R, et al. Independent prognostic value of BCR-ABL1–like signature and IKZF1 deletion, but not high CRLF2 expression, in children with B-cell precursor ALL. Blood. 2013;122:2622-2629. 36. van der Veer A, Zaliova M, Mottadelli F, et al. IKZF1 status as a prognostic feature in BCR-ABL1–positive childhood ALL. Blood. 2014;123:1691-1698. 37. Olsson L, Castor A, Behrendtz M, et al. Deletions of IKZF1 and SPRED1 are associated with poor prognosis in a population-based series of pediatric B-cell precursor acute lymphoblastic leukemia diagnosed between 1992 and 2011. Leukemia. 2014;28:302-310. 38. Mullighan CG, Miller CB, Radtke I, et al. BCR-ABL1 lymphoblastic leukaemia is characterized by the deletion of Ikaros. Nature. 2008;453:110-114. 39. Martinelli G, Iacobucci I, Soverini S, et al. New mechanisms of resistance in Philadelphia chromosome acute lymphoblastic leukemia. Expert Rev Hematol. 2009;2:297-303. 40. Den Boer ML, van Slegtenhorst M, De Menezes RX, et al. A subtype of childhood acute lymphoblastic leukaemia with poor treatment outcome: a genome-wide classification study. Lancet Oncol. 2009;10:125-134. 41. Tokunaga K, Yamaguchi S, Iwanaga E, et al. High frequency of IKZF1 genetic alterations in adult patients with B-cell acute lymphoblastic leukemia. Eur J Haematol. 2013;91:201-208. 42. Feldhahn N, Klein F, Mooster JL, et al. Mimicry of a constitutively active pre–B cell receptor in acute lymphoblastic leukemia cells. J Exp Med. 2005;201:1837-1852. 43. Iacobucci I, Iraci N, Messina M, et al. IKAROS deletions dictate a unique gene expression signature in patients with adult B-cell acute lymphoblastic leukemia. PLoS One. 2012;7:e40934. 44. Armstrong SA, Staunton JE, Silverman LB, et al. MLL translocations specify a distinct gene expression profile that distinguishes a unique leukemia. Nat Genet. 2002;30:41-47. 45. De Braekeleer E, Meyer C, Douet-Guilbert N, et al. Complex and cryptic chromosomal rearrangements involving the MLL gene in acute leukemia: a study of 7 patients and review of the literature. Blood Cells Mol Dis. 2010;44:268-274. 46. De Braekeleer E, Meyer C, Douet-Guilbert N, et al. Identification of MLL partner genes in 27 patients with acute leukemia from a single cytogenetic laboratory. Mol Oncol. 2011;5:555-563. 47. Meyer C, Hofmann J, Burmeister T, et al. The MLL recombinome of acute leukemias in 2013. Leukemia. 2013;27:2165-2176. 48. Pui CH, Rubnitz JE, Hancock ML, et al. Reappraisal of the clinical and biologic significance of myeloid-associated antigen expression in childhood acute lymphoblastic leukemia. J Clin Oncol. 1998;16:3768-3773. 49. Gleissner B, Goekbuget N, Rieder H, et al. CD10- pre–B acute lymphoblastic leukemia (ALL) is a distinct high-risk subgroup of adult ALL associated with a high frequency of MLL aberrations: results of the German Multicenter Trials for Adult ALL (GMALL). Blood. 2005;106:4054-4056. 50. Pui CH, Frankel LS, Carroll AJ, et al. Clinical characteristics and treatment outcome of childhood acute lymphoblastic leukemia with the t(4;11)(q21;q23): a collaborative study of 40 cases. Blood. 1991;77:440-447. 51. Stover EH, Chen J, Lee BH, et al. The small molecule tyrosine kinase inhibitor AMN107 inhibits TEL-PDGFRbeta and FIP1L1-PDGFRalpha in vitro and in vivo. Blood. 2005;106:3206-3213.
Am J Clin Pathol 2015;144:393-410 407 DOI: 10.1309/AJCPAN7BH5DNYWZB
Downloaded from http://ajcp.oxfordjournals.org/ by guest on January 17, 2017
20. Tabernero MD, Bortoluci AM, Alaejos I, et al. Adult precursor B-ALL with BCR/ABL gene rearrangements displays a unique immunophenotype based on the pattern of CD10, CD34, CD13 and CD38 expression. Leukemia. 2001;15:406-414. 21. Seegmiller AC, Kroft SH, Karandikar NJ, et al. Characterization of immunophenotypic aberrancies in 200 cases of B acute lymphoblastic leukemia. Am J Clin Pathol. 2009;132:940-949. 22. Jaso J, Thomas DA, Cunningham K, et al. Prognostic significance of immunophenotypic and karyotypic features of Philadelphia positive B-lymphoblastic leukemia in the era of tyrosine kinase inhibitors. Cancer. 2011;117:40094017. 23. Dordelmann M, Schrappe M, Reiter A, et al. Down’s syndrome in childhood acute lymphoblastic leukemia: clinical characteristics and treatment outcome in four consecutive BFM trials. Berlin-Frankfurt-Munster Group. Leukemia. 1998;12:645-651. 24. Chessells JM, Harrison G, Richards SM, et al. Down’s syndrome and acute lymphoblastic leukaemia: clinical features and response to treatment. Arch Dis Child. 2001;85:321-325. 25. Whitlock JA, Sather HN, Gaynon P, et al. Clinical characteristics and outcome of children with Down syndrome and acute lymphoblastic leukemia: a Children’s Cancer Group study. Blood. 2005;106:4043-4049. 26. Forestier E, Izraeli S, Beverloo B, et al. Cytogenetic features of acute lymphoblastic and myeloid leukemias in pediatric patients with Down syndrome: an iBFM-SG study. Blood. 2008;111:1575-1583. 27. Merkenschlager M. Ikaros in immune receptor signaling, lymphocyte differentiation, and function. FEBS Lett. 2010;584:4910-4914. 28. Iacobucci I, Lonetti A, Cilloni D, et al. Identification of different Ikaros cDNA transcripts in Philadelphia-positive adult acute lymphoblastic leukemia by a high-throughput capillary electrophoresis sizing method. Haematologica. 2008;93:1814-1821. 29. Trageser D, Iacobucci I, Nahar R, et al. Pre–B cell receptormediated cell cycle arrest in Philadelphia chromosome– positive acute lymphoblastic leukemia requires IKAROS function. J Exp Med. 2009;206:1739-1753. 30. Mullighan CG, Su X, Zhang J, et al. Deletion of IKZF1 and prognosis in acute lymphoblastic leukemia. N Engl J Med. 2009;360:470-480. 31. Martinelli G, Iacobucci I, Storlazzi CT, et al. IKZF1 (Ikaros) deletions in BCR-ABL1–positive acute lymphoblastic leukemia are associated with short disease-free survival and high rate of cumulative incidence of relapse: a GIMEMA AL WP report. J Clin Oncol. 2009;27:5202-5207. 32. Kuiper RP, Waanders E, van der Velden VH, et al. IKZF1 deletions predict relapse in uniformly treated pediatric precursor B-ALL. Leukemia. 2010;24:1258-1264. 33. Waanders E, van der Velden VH, van der Schoot CE, et al. Integrated use of minimal residual disease classification and IKZF1 alteration status accurately predicts 79% of relapses in pediatric acute lymphoblastic leukemia. Leukemia. 2011;25:254-258. 34. Yang YL, Hung CC, Chen JS, et al. IKZF1 deletions predict a poor prognosis in children with B-cell progenitor acute lymphoblastic leukemia: a multicenter analysis in Taiwan. Cancer Sci. 2011;102:1874-1881.
Loghavi et al / B-ALL/Lymphoblastic Lymphoma
408 Am J Clin Pathol 2015;144:393-410 DOI: 10.1309/AJCPAN7BH5DNYWZB
70. Walters R, Kantarjian HM, Keating MJ, et al. The importance of cytogenetic studies in adult acute lymphocytic leukemia. Am J Med. 1990;89:579-587. 71. Carli MG, Cuneo A, Piva N, et al. Lymphoblastic lymphoma with primary splenic involvement and the classic 14;18 translocation. Cancer Genet Cytogenet. 1991;57:47-51. 72. Kramer MH, Raghoebier S, Beverstock GC, et al. De novo acute B-cell leukemia with translocation t(14;18): an entity with a poor prognosis. Leukemia. 1991;5:473-478. 73. Nacheva E, Dyer MJ, Fischer P, et al. C-MYC translocations in de novo B-cell lineage acute leukemias with t(14;18)(cell lines Karpas 231 and 353). Blood. 1993;82:231-240. 74. Nakamura F, Tatsumi E, Tani K, et al. Coexpression of cellsurface immunoglobulin (sIg), terminal deoxynucleotidyl transferase (TdT) and recombination activating gene 1 (RAG-1): two cases and derived cell lines. Leukemia. 1996;10:1159-1163. 75. Onciu M, Bueso-Ramos C, Medeiros LJ, et al. Acute lymphoblastic leukemia in elderly patients the Philadelphia chromosome may not be a significant adverse prognostic factor. Am J Clin Pathol. 2002;117:716-720. 76. Hardianti MS, Tatsumi E, Syampurnawati M, et al. Presence of somatic hypermutation and activation-induced cytidine deaminase in acute lymphoblastic leukemia L2 with t(14;18) (q32;q21). Eur J Haematol. 2005;74:11-19. 77. Snuderl M, Kolman OK, Chen YB, et al. B-cell lymphomas with concurrent IGH-BCL2 and MYC rearrangements are aggressive neoplasms with clinical and pathologic features distinct from Burkitt lymphoma and diffuse large B-cell lymphoma. Am J Surg Pathol. 2010;34:327-340. 78. Subramaniyam S, Fraser CR, Rao PH, et al. De novo B lymphoblastic leukemia/lymphoma in an adult with t(14;18) (q32;q21) and c-MYC gene rearrangement involving 10p13. Leuk Lymphoma. 2011;52:2195-2199. 79. Chapiro E, Radford-Weiss I, Cung HA, et al. Chromosomal translocations involving the IGH@ locus in B-cell precursor acute lymphoblastic leukemia: 29 new cases and a review of the literature. Cancer Genet. 2013;206:162-173. 80. Seo JY, Lee SH, Kim HJ, et al. MYC rearrangement involving a novel non-immunoglobulin chromosomal locus in precursor B-cell acute lymphoblastic leukemia. Ann Lab Med. 2012;32:289-293. 81. Harvey RC, Mullighan CG, Wang X, et al. Identification of novel cluster groups in pediatric high-risk B-precursor acute lymphoblastic leukemia with gene expression profiling: correlation with genome-wide DNA copy number alterations, clinical characteristics, and outcome. Blood. 2010;116:4874-4884. 82. Schuurmans Stekhoven JH, Langenhuysen CA, Bakkeren JA, et al. Morphology and incidence of the “posttherapeutic lymphoid cell” in the bone marrow of children with acute lymphoblastic leukemia. Am J Pathol. 1986;124:46-52. 83. Hurwitz CA, Loken MR, Graham ML, et al. Asynchronous antigen expression in B lineage acute lymphoblastic leukemia. Blood. 1988;72:299-307. 84. Weir EG, Cowan K, LeBeau P, et al. A limited antibody panel can distinguish B-precursor acute lymphoblastic leukemia from normal B precursors with four color flow cytometry: implications for residual disease detection. Leukemia. 1999;13:558-567. 85. Huh YO, Ibrahim S. Immunophenotypes in adult acute lymphocytic leukemia: role of flow cytometry in diagnosis and monitoring of disease. Hematol Oncol Clin North Am. 2000;14:1251-1265. © American Society for Clinical Pathology
Downloaded from http://ajcp.oxfordjournals.org/ by guest on January 17, 2017
52. von Bubnoff N, Gorantla SP, Thone S, et al. The FIP1L1-PDGFRA T674I mutation can be inhibited by the tyrosine kinase inhibitor AMN107 (nilotinib). Blood. 2006;107:4970-4972. 53. Gotlib J. World Health Organization–defined eosinophilic disorders: 2014 update on diagnosis, risk stratification, and management. Am J Hematol. 2014;89:325-337. 54. Grimaldi JC, Meeker TC. The t(5;14) chromosomal translocation in a case of acute lymphocytic leukemia joins the interleukin-3 gene to the immunoglobulin heavy chain gene. Blood. 1989;73:2081-2085. 55. Harrison CJ, Moorman AV, Broadfield ZJ, et al. Three distinct subgroups of hypodiploidy in acute lymphoblastic leukaemia. Br J Haematol. 2004;125:552-559. 56. De Jong D, Voetdijk BM, Beverstock GC, et al. Activation of the c-myc oncogene in a precursor–B-cell blast crisis of follicular lymphoma, presenting as composite lymphoma. N Engl J Med. 1988;318:1373-1378. 57. Gauwerky CE, Hoxie J, Nowell PC, et al. Pre–B-cell leukemia with a t(8; 14) and a t(14; 18) translocation is preceded by follicular lymphoma. Oncogene. 1988;2:431-435. 58. Li S, Lin P, Fayad LE, et al. B-cell lymphomas with MYC/8q24 rearrangements and IGH@BCL2/t(14;18) (q32;q21): an aggressive disease with heterogeneous histology, germinal center B-cell immunophenotype and poor outcome. Mod Pathol. 2012;25:145-156. 59. Fiedler W, Weh HJ, Zeller W, et al. Translocation (14; 18) and (8; 22) in three patients with acute leukemia/ lymphoma following centrocytic/centroblastic non-Hodgkin’s lymphoma. Ann Hematol. 1991;63:282-287. 60. Kroft SH, Domiati-Saad R, Finn WG, et al. Precursor B-lymphoblastic transformation of grade I follicle center lymphoma. Am J Clin Pathol. 2000;113:411-418. 61. Sun X, Gordon LI, Peterson LC. Transformation of follicular lymphoma to acute lymphoblastic leukemia. Arch Pathol Lab Med. 2002;126:997-998. 62. Kobrin C, Cha SC, Qin H, et al. Molecular analysis of light-chain switch and acute lymphoblastic leukemia transformation in two follicular lymphomas: implications for lymphomagenesis. Leuk Lymphoma. 2006;47:1523-1534. 63. Young KH, Xie Q, Zhou G, et al. Transformation of follicular lymphoma to precursor B-cell lymphoblastic lymphoma with c-myc gene rearrangement as a critical event. Am J Clin Pathol. 2008;129:157-166. 64. Kaplan A, Samad A, Dolan MM, et al. Follicular lymphoma transformed to “double-hit” B lymphoblastic lymphoma presenting in the peritoneal fluid. Diagn Cytopathol. 2013;41:986-990. 65. Kridel R, Sehn LH, Gascoyne RD. Pathogenesis of follicular lymphoma. J Clin Invest. 2012;122:3424-3431. 66. de Jong D, de Boer JP. Predicting transformation in follicular lymphoma. Leuk Lymphoma. 2009;50:1406-1411. 67. Mufti GJ, Hamblin TJ, Oscier DG, et al. Common ALL with pre–B-cell features showing (8;14) and (14;18) chromosome translocations. Blood. 1983;62:1142-1146. 68. Pegoraro L, Palumbo A, Erikson J, et al. A 14;18 and an 8;14 chromosome translocation in a cell line derived from an acute B-cell leukemia. Proc Natl Acad Sci U S A. 1984;81:7166-7170. 69. Thangavelu M, Olopade O, Beckman E, et al. Clinical, morphologic, and cytogenetic characteristics of patients with lymphoid malignancies characterized by both t(14;18) (q32;q21) and t(8;14)(q24;q32) or t(8;22)(q24;q11). Genes Chromosomes Cancer. 1990;2:147-158.
AJCP / Review Article
© American Society for Clinical Pathology
102. Reardon DA, Hanson CA, Roth MS, et al. Lineage switch in Philadelphia chromosome–positive acute lymphoblastic leukemia. Cancer. 1994;73:1526-1532. 103. Delia D, Polli N, Borrello MG, et al. Mixed-lineage leukemias and phenotypic shifts occurring in relapsed cases of acute T lymphoblastic lymphomas. Leukemia. 1988;2:192S197S. 104. Borowitz MJ, Pullen DJ, Winick N, et al. Comparison of diagnostic and relapse flow cytometry phenotypes in childhood acute lymphoblastic leukemia: implications for residual disease detection: a report from the children’s oncology group. Cytometry B Clin Cytom. 2005;68:18-24. 105. Pagano L, Pulsoni A, Tosti ME, et al. Acute lymphoblastic leukaemia occurring as second malignancy: report of the GIMEMA archive of adult acute leukaemia. Gruppo Italiano Malattie Ematologiche Maligne dell’Adulto. Br J Haematol. 1999;106:1037-1040. 106. Ishizawa S, Slovak ML, Popplewell L, et al. High frequency of pro–B acute lymphoblastic leukemia in adults with secondary leukemia with 11q23 abnormalities. Leukemia. 2003;17:1091-1095. 107. Shivakumar R, Tan W, Wilding GE, et al. Biologic features and treatment outcome of secondary acute lymphoblastic leukemia—a review of 101 cases. Ann Oncol. 2008;19:1634-1638. 108. Chen W, Wang E, Lu Y, et al. Therapy-related acute lymphoblastic leukemia without 11q23 abnormality: report of six cases and a literature review. Am J Clin Pathol. 2010;133:75-82. 109. Holdener SL, Harrington L, Nguyen J, et al. Therapy-related B lymphoblastic leukemia with t(4;11)(q21;q23)/AF4-MLL in a patient with mantle cell lymphoma after recent aggressive chemotherapy—a unique case report. Int J Clin Exp Pathol. 2014;7:1800-1804. 110. Tang G, Zuo Z, Thomas DA, et al. Precursor B-acute lymphoblastic leukemia occurring in patients with a history of prior malignancies: is it therapy-related? Haematologica. 2012;97:919-925. 111. Andersen MK, Christiansen DH, Jensen BA, et al. Therapy-related acute lymphoblastic leukaemia with MLL rearrangements following DNA topoisomerase II inhibitors, an increasing problem: report on two new cases and review of the literature since 1992. Br J Haematol. 2001;114:539-543. 112. Bloomfield CD, Archer KJ, Mrozek K, et al. 11q23 balanced chromosome aberrations in treatment-related myelodysplastic syndromes and acute leukemia: report from an international workshop. Genes Chromosomes Cancer. 2002;33:362-378. 113. Mauritzson N, Albin M, Rylander L, et al. Pooled analysis of clinical and cytogenetic features in treatment-related and de novo adult acute myeloid leukemia and myelodysplastic syndromes based on a consecutive series of 761 patients analyzed 1976-1993 and on 5098 unselected cases reported in the literature 1974-2001. Leukemia. 2002;16:2366-2378. 114. Kakihara T, Imai C, Kaneko T, et al. Atypical hemophagocytic lymphohistiocytosis following bacterial tonsillitis in acute lymphoblastic leukemia. Leuk Lymphoma. 2003;44:1247-1248. 115. Goldschmidt N, Gural A, Kornberg A, et al. Prolonged fever of unknown origin and hemophagocytosis evolving into acute lymphoblastic leukemia. Am J Hematol. 2004;76:364-367. 116. Trebo MM, Attarbaschi A, Mann G, et al. Histiocytosis following T-acute lymphoblastic leukemia: a BFM study. Leuk Lymphoma. 2005;46:1735-1741.
Am J Clin Pathol 2015;144:393-410 409 DOI: 10.1309/AJCPAN7BH5DNYWZB
Downloaded from http://ajcp.oxfordjournals.org/ by guest on January 17, 2017
86. Rimsza LM, Larson RS, Winter SS, et al. Benign hematogone-rich lymphoid proliferations can be distinguished from B-lineage acute lymphoblastic leukemia by integration of morphology, immunophenotype, adhesion molecule expression, and architectural features. Am J Clin Pathol. 2000;114:66-75. 87. McKenna RW. Immunophenotypic analysis of hematogones (B-lymphocyte precursors) in 662 consecutive bone marrow specimens by 4-color flow cytometry. Blood. 2001;98:2498-2507. 88. Riley RS, Massey D, Jackson-Cook C, et al. Immunophenotypic analysis of acute lymphocytic leukemia. Hematol Oncol Clin North Am. 2002;16:245-299, v. 89. Mlcakova A, Babusikova O. Multiparametric flow cytometry in detection of minimal residual disease in acute lymphoblastic leukemia of early B-cell phenotype. Neoplasma. 2003;50:416-421. 90. McKenna RW, Asplund SL, Kroft SH. Immunophenotypic analysis of hematogones (B-lymphocyte precursors) and neoplastic lymphoblasts by 4-color flow cytometry. Leuk Lymphoma. 2004;45:277-285. 91. Babusikova O, Zeleznikova T, Mlcakova A, et al. The knowledge on the 3rd type hematogones could contribute to more precise detection of small numbers of precursor B-acute lymphoblastic leukemia. Neoplasma. 2005;52:502-509. 92. Chen W, Karandikar NJ, McKenna RW, et al. Stability of leukemia-associated immunophenotypes in precursor B-lymphoblastic leukemia/lymphoma: a single institution experience. Am J Clin Pathol. 2007;127:39-46. 93. Babusikova O, Zeleznikova T, Kirschnerova G, et al. Hematogones in acute leukemia during and after therapy. Leuk Lymphoma. 2008;49:1935-1944. 94. Hassanein NM, Alcancia F, Perkinson KR, et al. Distinct expression patterns of CD123 and CD34 on normal bone marrow B-cell precursors (“hematogones”) and B lymphoblastic leukemia blasts. Am J Clin Pathol. 2009;132:573-580. 95. Muzzafar T, Medeiros LJ, Wang SA, et al. Aberrant underexpression of CD81 in precursor B-cell acute lymphoblastic leukemia: utility in detection of minimal residual disease by flow cytometry. Am J Clin Pathol. 2009;132:692-698. 96. Borowitz MJ, Bene MC, Harris NL, et al. Acute leukemias of ambiguous lineage. In: Swerdlow SH, Campo E, Harris NL, et al, eds. WHO Classification of Tumours of Haematopoietic and Lymphoid Tissues. 4th ed. Lyon, France: IARC; 2008:150-155. 97. Bennett JM, Catovsky D, Daniel MT, et al. Proposals for the classification of the acute leukaemias. FrenchAmerican-British (FAB) co-operative group. Br J Haematol. 1976;33:451-458. 98. Bene MC, Castoldi G, Knapp W, et al. Proposals for the immunological classification of acute leukemias. European Group for the Immunological Characterization of Leukemias (EGIL). Leukemia. 1995;9:1783-1786. 99. Guy J, Antony-Debre I, Benayoun E, et al. Flow cytometry thresholds of myeloperoxidase detection to discriminate between acute lymphoblastic or myeloblastic leukaemia. Br J Haematol. 2013;161:551-555. 100. Borowitz MJ. Mixed phenotype acute leukemia. Cytometry B Clin Cytom. 2014;86:152-153. 101. Pane F, Frigeri F, Camera A, et al. Complete phenotypic and genotypic lineage switch in a Philadelphia chromosome– positive acute lymphoblastic leukemia. Leukemia. 1996;10:741-745.
Loghavi et al / B-ALL/Lymphoblastic Lymphoma
410 Am J Clin Pathol 2015;144:393-410 DOI: 10.1309/AJCPAN7BH5DNYWZB
124. Jordan MB, Allen CE, Weitzman S, et al. How I treat hemophagocytic lymphohistiocytosis. Blood. 2011;118:4041-4052. 125. Kochenderfer JN, Rosenberg SA. Treating B-cell cancer with T cells expressing anti-CD19 chimeric antigen receptors. Nat Rev Clin Oncol. 2013;10:267-276. 126. Kochenderfer JN, Wilson WH, Janik JE, et al. Eradication of B-lineage cells and regression of lymphoma in a patient treated with autologous T cells genetically engineered to recognize CD19. Blood. 2010;116:4099-4102. 127. Kalos M, Levine BL, Porter DL, et al. T cells with chimeric antigen receptors have potent antitumor effects and can establish memory in patients with advanced leukemia. Sci Transl Med. 2011;3:95ra73. 128. Porter DL, Levine BL, Kalos M, et al. Chimeric antigen receptor-modified T cells in chronic lymphoid leukemia. N Engl J Med. 2011;365:725-733. 129. Kochenderfer JN, Dudley ME, Feldman SA, et al. B-cell depletion and remissions of malignancy along with cytokine-associated toxicity in a clinical trial of anti-CD19 chimeric-antigen-receptor-transduced T cells. Blood. 2012;119:2709-2720. 130. Brentjens RJ, Riviere I, Park JH, et al. Safety and persistence of adoptively transferred autologous CD19-targeted T cells in patients with relapsed or chemotherapy refractory B-cell leukemias. Blood. 2011;118:4817-4828.
© American Society for Clinical Pathology
Downloaded from http://ajcp.oxfordjournals.org/ by guest on January 17, 2017
117. Kuzmanovic M, Rasovic N, Micic D, et al. Epstein-Barr virus associated hemophagocytic lymphohystiocytosis during maintenance treatment of acute lymphoblastic leukemia. Pediatr Blood Cancer. 2006;46:832. 118. Kawabata Y, Hirokawa M, Saitoh Y, et al. Late-onset fatal Epstein-Barr virus–associated hemophagocytic syndrome following cord blood cell transplantation for adult acute lymphoblastic leukemia. Int J Hematol. 2006;84:445-448. 119. O’Brien MM, Lee-Kim Y, George TI, et al. Precursor B-cell acute lymphoblastic leukemia presenting with hemophagocytic lymphohistiocytosis. Pediatr Blood Cancer. 2008;50:381-383. 120. Breakey VR, Abdelhaleem M, Weitzman S, et al. Hemophagocytic lymphohistiocytosis onset during induction therapy for precursor B-cell acute lymphoblastic leukemia. J Pediatr Hematol Oncol. 2008;30:956-958. 121. Furutani A, Imamura T, Ueda I, et al. Hemophagocytic lymphohistiocytosis during maintenance treatment of precursor B-cell acute lymphoblastic leukemia. Int J Hematol. 2008;88:610-612. 122. Kelly C, Salvi S, McClain K, et al. Hemophagocytic lymphohistiocytosis associated with precursor B acute lymphoblastic leukemia. Pediatr Blood Cancer. 2011;56:658-660. 123. Moritake H, Kamimura S, Nunoi H, et al. Clinical characteristics and genetic analysis of childhood acute lymphoblastic leukemia with hemophagocytic lymphohistiocytosis: a Japanese retrospective study by the Kyushu-Yamaguchi Children’s Cancer Study Group. Int J Hematol. 2014;100:70-78.