Classical and molecular cytogenetics in oncology Kyra Michalova and Zuzana Zemanova Center of Oncocytogenetics Institute of Clinical Biochemistry and Laboratory Diagnostics General University Hospital and First Faculty of medecine, medecine, Charles University Prague
Cytogenetic examination Clinical cytogenetics → determination of karyotype of patients with inborn deffects Prenatal diagnostics → examination of chromosomal complement of embryos embryos,, in vitro fertilization Oncocytogenetics → specification of diagnosis and prognosis of malignant diseases Services of hygiene laboratories - testing of mutagenicity of chemicals on human organism on chromosomal level, level, radiation cytogenetics etc. etc.
Chromosomal aberrations Changes of number or structure of chromosomes I. Inborn (constitutional constitutional)) aberrations are fundamental for origin of syndromes due to anomalies of chromosomes (for example Down Down´´s sy sy)); changes of chromosomes are present in all cells of the body. body. II. II. Acquired changes of chromosomes in malignant cells;; they have clonal character (only certain cellular cells clones are involved involved)).
Cancer cells high
genome
instability
-
one
of
the
most
important events in the malignant process gene
mutations
and
numerical
and/or
structural
chromosomal aberrations
Nonrandom chromosomal aberrations are associated with specific disease subtypes and have a clear prognostic implications. implications
Methods
Conventional cytogenetic analysis
mFISH
I-FISH
mBAND
WCPWCP -FISH
CGH
Array CGH
Conventional cytogenetic analysis
Karyotype analysis Detection of chromosomal aberrations (numerical x structural structural))
krev, kostní dřeň
medium
kolchicin
hypotonie
fixace
preparace
inkubace při 37°C
barvení
Postup při kultivaci a přípravě preparátů k cytogenetickému vyšetření
Chromosomal banding: banding:
Limitations of classical cytogenetics sensitivity of chromosomal banding techniques is limited these techniques require a high rate of dividing cells with good chromosomal morphology (resolution limit of 10 Mb) Mb) in some leukemias malignant cells are not proliferating in the cell culture (only the normal cells are dividing) → the results of cytogenetic examination is not representative for malignant process chromosomal changes in leukemic cells are very often complex or could be cryptic under the limit of light microscopy
Fluorescence in situ hybridization (FISH) permits detection of selected acquired genetic changes in dividing (metaphase metaphase)) and nondividing (interphase nuclei nuclei)) cells is useful in establishing the percentage of neoplastic cells at the time of diagnosis and after therapy FISH studies are used to investigate the origin and progression of hematologic malignancies and to establish which
hematopoietic
neoplastic processes
compartments
are
involved
in
Fluorescence in situ hybridization (FISH)
Cytogenetický preparát
Dvouřetězcová značená DNA
Denaturace buněčné DNA fixované na cytogenetickém preparátu
Denaturace DNA sondy
Hybridizace DNA sondy ke komplementárním úsekům cílové DNA fixované na cytogenetickém preparátu
Analýza fluorescenčních signálů ve fluorescenčním mikroskopu
Probes for specific chromosomal structures:: structures α-satellite DNA - centromeres Determination of numerical aberrations aberrations,, identification of the origin of cenromeres in marker marker--chromosomes, chromosomes, specification of cells after bone marrow transplantation (opposite sex of donor and recipient) metaphase x interphase
Locus specific DNA probes: probes: Mapping of genes on chromosomes chromosomes,, detection of structural rearrangements (translocations translocations,, deletions) deletions) metaphase x interphase
Chromosome painting probes probes:: They contain sequences from whole chromosomes or chromosomal parts (partial probes) probes) Determination of structural rearrangements (translocations and deletions of large extent), extent), identification of origin of marker marker-chromosomes Metaphase only
Multicolor FISH - mFISH allows in one hybridization experiment distinguish according to different color every pair of autosomes and sex chromosomes and then it is possible to make analyses of the whole genome and every structural and numerical rearrangement
Multicolor FISH - mFISH analyses of complex chromosomal rearrangements in bone marrow cells of patients with hematological malignancies will bring us detailed informations about involvement of specific chromosomes or their regions into rearrangements
Multicolor banding with high resolution - mBAND enables determination of exact breakpoints of chromosomal aberrations with much higher resolution than classical banding
mBAND 1
mBAND 11
ArrayArray -based comparative genomic hybridization (aCGH aCGH)) new tool to search for recurrent gains or loss of chromosomal regions throughout the genome according to detection with very high resolution of copy number changes at DNA level only recently is aCGH successfully utilised in diagnostics of leukemias and the results revealed a large spectrum of genomic imbalancies, imbalancies, including novel recurrent deletions and amplifications
BAC arrays ∼1MB Oligo arrays ∼100 kb (maximal resolution ∼ 35 kb) kb)
The impact of conventional and molecular cytogenetic analysis in oncohematology Is part of the work up at diagnosis Provides comprehensive information on the karyotype
�
help to specify diagnosis
�
help to determine the prognosis
�
help monitor effectiveness of treatment
Chronic Myeloid Leukemia (CML CML)) Acute Myeloid Leukemia (AML (AML) Acute Lymphoblastic Leukemia (ALL)
Hematological malignancies
Myelodysplastic Syndromes (MDS (MDS)) Chronic Lymphocytic Leukemia (C (CLL LL)) Multiple Myeloma (MM) Non Hodkin Lymphoma (NHL)
Recommended examination procedures - depending on the type of disease and treatment protocol
CML
Chronic Myeloid Leukemia (CML) � � �
1515-20% 20% of all leukemia cases Mainly in adults (median age 65 years years)) TriTri -phasic disease: disease: CP - chronic phase (relatively benign benign,, 3-9 years) AP - More malignant accelerated phase BC - Terminal blast crisis
� �
Blasts increase rapidly (crowd out healthy cells cells))
�
One of the first malignancies in which a therapy targeting the underlying molecular defect has improved the clinical outcome of patients:: Gleevec™ patients leevec™ (Novartis) used for therapy
�
t(9 t(9;22)(q 22)(q34 34;;q11) 11) in 9090-95% 95% of patients (detectable by CC CC)) BCR/ABL fusion gene
One of the bestbest-studied malignancies - has served as a paradigm for elucidation how genetic changes cause cells to become malignant: malignant: Ph chromosome t(9 t(9;22)(q 22)(q34 34;;q11) 11) - BCR/ABL fusion
-
Conventional Cytogenetics: BM 24h/48h cultivation (adults) at least 20 metaphases
normal karyotype or insufficient metaphases or normal karyotype without t(9;22)
FISH: BCR/ABL1
aberrant karyotype
targeted FISH or other molecular cytogenetic techniques (mFISH/mBAND, array CGH)
Report according to ISCN
CML
Chronic Myeloid Leukemia (CML)
� Heterogenous group
of malignant diseases of haemopoiesis
� Accumulation
of immature myeloid cells (myeloblasts) in bone
� Diagnosed in
all age groups
marrow
� Most
commonly affects people older than 60 years (median age 64-68 years)
� Secondary AML,
therapy-related AML
� Aggressive disease - median OS 2-3 � Specific chromosomal aberrations significance → stratification cytogenetic findings
of
monts with clear prognostic therapy according to
AML
Acute Myeloid Leukemia (AML)
Chromosomal aberration
Genes
Prognosis
t(8;21)(q22;q22)
RUNX1-RUNX1T1
good
inv(16)(p13.1q22) or t(16;16)(p13.1;q22)
CBFB-MYH11
good
t(15;17)(q22;q12)
PML-RARA
good
t(9;11)(p22;q23)
MLLT3-MLL
intermedial
t(6;9)(p23;q34)
DEK-NUP214
poor
inv(3)(q21q26.2) or t(3;3)(q21;q26.2)
RPN1-EVI1
worst
t(1;22)(p13;q13)
RBM15-MKL1
good
Rearrangements of MLL gene
MLL
poor
monosomy 7 or deletion of 7q31
poor
deletion of 5q31
?
poor
complex chromosomal aberrations
?
worst
AML
Cytogenetic findings in AML
AML
Prognostic impact of specific chromosomal aberrations in acute myeloid leukemia (AML) 1.0
Kumulative surviving
0.9 0.8
normal karyotype
0.7
complex karyotype
0.6
t(8;21)(q22;q22) t(15;17)(q22;q11)
0.5
inv(16)/t(16;16)
0.4
5q-
0.3
-7/7q-
0.2
+8
0.1
> 50 chromosomes
0.0 0
50 100 150 200 250 300 350 400 450 500 Time (weeks)
Alert 2006
Conventional Cytogenetics: BM 24h/48h cultivation (adults) at least 20 metaphases
aberrant karyotype
normal karyotype or insufficient metaphases
Subtype specific FISH: MLL, 5q31/5p15, 7q31/7, 8/9 PML/RARA, AML1/ETO, CBFB
targeted FISH or other molecular cytogenetic techniques (mFISH/mBAND, array CGH)
Report according to ISCN
AML
Acute Myeloid Leukemia (AML)
�
Accumulation of malignant, immature lymphoid cells in the bone marrow and mostly also in peripheral blood
�
Most common malignancy in children – representing 25% of pediatric cancer
� �
80% of pediatric leukemias
�
Chromosomal aberrations: found up to 90% of cases one of the most important prognostic factors!!
�
Conventional chromosomal analysis are limited by the low mitotic activity of malignant B-lymphocytes → I-FISH for the most common recurrent chromosomal aberrations
Heterogenous implications
disease
-
distinct
therapeutic
and
prognostic
ALL
Acute Lymphoblastic Leukemia (ALL) Overview
Cytogenetic findings in ALL Risk Group Low risk
Cytogenetic finding High hyperdiploidy (51-65 chromosomes)
ETV6-RUNX1 t(1;19)(q23;p13)
IGH-CEBP IGH-ID4 del(6)(q) Aberration of 9p
Standard risk
Aberration of 11q dup(1q) -7 dic(9;20)(p13;q11) dic(9;12)(p11-21;p11-13) Any other aberration normal karyotype t(9;22)(q34;q11) iAMP21
MLL translocations
High risk
„near“ haploidy (˂30 chromosomes) Low hypodiploidy (30-39 chromosomes) t(17;19)(q23;p13) Aberration of 17p Loss of 13q
Moorman et al., Lancet Oncol 2010
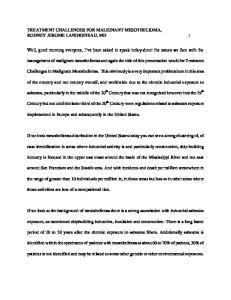
100%
t(12;21)
t(1;19) 50% t(4;11) t(9;22)
1
2
3
4
5
years
Today, karyotype remains the gold standard for classification of patients with childhood ALL into risk group for treatment.
ALL
Prognostic impact of specific chromosomal aberrations in childhood acute lymphoblastic leukemia (ALL)
I-FISH:
Conventional Cytogenetics:
B-ALL: „triple test“
BM direct/24h cultivation (childhood) 24h/48h cultivation (adults) at least 20 metaphases
ETV6/RUNX1 MLL Hyperdiploidy
or aberrant karyotype
T-ALL:
TCR genes targeted FISH or other molecular cytogenetic techniques (mFISH/mBAND, array CGH)
TCRαδ (14q11), TCRβ (7q34), TCRγ (7p14)
Report according to ISCN
TP16 (9p21) ABL1 (9q34)
ALL
Acute Lymphoblastic Leukemia (ALL)
CONCLUSIONS The impact of cytogenetic analyses on clinical diagnostics of hematological malignancies has increased dramatically during recent years → laboratory techniques have to be optimized to provide reliable results for optimal patient care. Quick and correct results save time and money by preventing unnecessary additional diagnostics and suboptimal treatment approaches. Standardization of cytogenetic diagnostic protocols may help to improve diagnosis, and hence treatment outcome of hematologic malignancies.