Health Risk from Air Pollution in Utah bY Steven C. Packham, Ph.D, D.A.B.T.
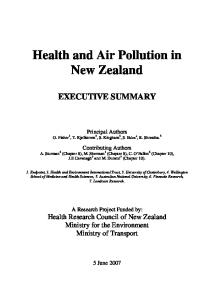
Introduction The most prevalent air contaminants regulated by law in Utah are carbon monoxide (CO), ozone and PMlO (i.e., particles in the air that are 10 microns or smaller in diameter which can be breathed deep into the- lungs). In addition to CO, ozone and PM10, there are national standards for lead, oxides of sulfur and oxides of nitrogen. Most air pollution comes from either industrial and commercial processes, or from cars, trucks, construction equipment, lawn mowers, or other equipment which bum petroleum products as fuel. Each of these pollutants can adversely affect health. Air quality professionals develop inventories of pollution emissions from all known types of sources through engineering calculations, surveys, computer models a n d - direct measurements. Environmental laws require states to reduce emissions and document reductions in emissions inventories in areas of the state where air pollution exceeds the national health standards or where pollution is considered to be a threat to public health or the environment. There are four counties and three cities in Utah that have historically exceeded one or more of the National Ambient Air Quality Standards (see Figure 1). In the last 15 years there has been improvement in air quality in these areas as indicated by the number of times air pollution has exceeded the national standards (Table 1). Table 1. Number of exceedances in non-attainment areas per year.
Performance Measures CO-carbon monoxide PM 10-fine particulate matter 03-ozone SOx-oxides of sulful NOx-oxides of nitrogen Pb-lead This improvement, despite population growth, has been achieved through stricter pollution controls on cars and on industries. Population growth predicted for Utah into the next century
poses the greatest pressure on rising pollution inventories. The Division of Air Quality is developing "maintenance" plans as part of its State Implementation Plan to assure that air quality is not compromised as the state continues its economic growth.
Health Effects and Standards Carbon monoxide, ozone and PMlO differ in how persistent they are in the air and in their health effects. The level of protection offered by federal standards also varies for these pollutants. Carbon monoxide is produced directly from burning fuels such as gasoline and woodburning stoves. It is ubiquitous in all urban areas and CO produced today can stay in the air for over a month. Winds move CO pollution from its various sources to far distances. It is basically air movement, rather than CO decay, which keeps urban CO levels as low as they are. In contrast, ozone is not formed directly from cars or industry, but is a by-product of a chemical reaction between two other groups of pollutants, volatile organic compounds and oxides of nitrogen. This reaction is driven by sunlight and high summer temperatures. Ozone is formed in the afternoon on hot summer days and decays overnight when the temperature drops and the sun goes down. PMlO, unlike CO or ozone, is not a homogeneous substance. It is made up of particles from many different sources. It can include chemically neutral particles similar to little rocks and grains of sand, and it can include chemically potent particles made from condensing gases.- The chemical and physical nature of the particles included in PMlO varies from city to city, county to county and from day to day within those areas depending on weather conditions. The persistency of PMlO in the air depends on how much the particles weigh, on whether they are solid or volatile and on where, when and how they are made. The health effects and the level of protection possible from air standards also differ greatly for these air pollutants. Carbon monoxide displaces oxygen in the blood and prevents the blood from carrying oxygen from
Utah's Health: An Annual Review 1996
21
the lungs to the body. Since CO is 220 times more effective than oxygen at attaching to hemoglobin in the blood, scientists can calculate precisely how much CO in the air will be associated with various levels of CO in the blood and what the corresponding health effects will be. The maximum one-hour standard for CO is set at 0.0003 percent in air, or 35 parts-permillion (ppm). The standard for an eight-hour average concentration is 9 ppm. At these levels of CO in the air, the .blood will have-.only0.5 to 1.7 percent of its hemoglobin tied up by CO. There are no symptoms or adverse health effects from CO at these levels. In fact, symptoms of CO poisoning are not manifest in most healthy people until blood levels exceed 15 percent. The CO air standard provides a large margin of safety for normal individuals and a comfortable level of protection for people which chronic cardiovascular and respiratory disease. The level of protection possible for ozone is much different. Chemically, the ozone molecule is made of three oxygen atoms (03); normal oxygen is made of two oxygen atoms (02). Ozone oxidizes, or reacts with things much more readily than normal oxygen. When ozone is inhaled, it attacks the lining of the respiratory system; i.e., the nose, throat, trachea, bronchi and lungs, and it does this at very low concentrations. Studies have documented respiratory effects from ozone in concentrations as low as 0.25 ppml, or when ozone levels in the air are at 0.000025 percent. Background levels of ozone in unpopulated areas are in the .03-.05 ppm range. The air standard for ozone is currently set at 0.12 ppm. There is virtually no margin of safety between the current standard and where adverse effects have been seen. The threshold toxic level is only 4 to 5 times higher than background levels. In a practical sense, there is a definite limit to how much protection any standard can reasonably be expected to provide from ozone. The ozone standard is presently under review by EPA and is likely to be tightened, though there is very little room to do this without approaching background levels. The air quality standard for PMlO is also under review by EPA. Recommendations to include a standard for particulates in the 2.5 micron and smaller range is expected this summer. The recommendation for a new PM2.5 standard is based on a general consensus that particles made of condensed gases from burning fuels fall into this size range and are biologically more reactive and potent than the
22 Health Risk from Air Pollution
larger particles. The review of the standard has also been prompted by studies which have shown an association between pollution, including PMlO pollution, and slight increases in mortality rates in over a dozen cities in the United States and Europe.2 These epidemiological studies are being looked at with concern. Taken at face value, they imply that there is no safe level for PMlO. While no one is questioning that PMlO is harmful, there is some controversy over how precise and valid the epidemiological data may be in quantifying risk since the observed associations do not prove a causal relationship between PMlO and premature mortality. Indeed, a number of studies in Utah have failed to show such Despite these conflicting associations .3.4 observations, and even though a feasible mechanism has not been offered for how outdoor PMlO could be affecting at-risk populations in hospitals and care centers, EPA has concluded that the epidemiological studies and anecdotal experience suggest that PM 10 concentrations below the current standard may be posing some, though presently unquantified, risk to public health. Conclusions The health risks from air pollution in Utah are diminishing as Utah experiences fewer and fewer exceedances of the national air quality standards. Risks from exposure to lead and to oxides of sulfur and nitrogen are quite negligible, and there is a comfortable margin of safety between the CO standard and adverse health effects. Transitory exceedances of the CO standard, while undesirable, are not an immanent threat to health. The air pollutants that put Utahns at greatest risk are ozone and PM10. There are two counties, Salt Lake and Davis Counties, with a combined population of over 900,000 currently classified as not attaining the standard for ozone, but both counties have reported ozone levels within the standard for the last five, years and Utah has formally requested that EPA redesignate these counties as being in compliance with the standard. Notwithstanding this progress, ozone remains a risk to health because there is virtually no margin of safety between the standard and adverse health effects. It will take aggressive and vigilant efforts to assure that future population growth does not result in unhealthy ozone levels.
A dose-response curve and threshold level of safety has not been developed for PMlO. PMlO on high pollution days is chemically different from PMlO on cleaner days. Thus, while epidemiological studies have shown associations between high PMlO pollution days and health effects using regression models, one cannot conclude whether those associations are related to a change in the amount, or dose, of the PM10, or in the precise nature of the particles. Furthermore, evidentiary support for the theory that PM is causing mortality is lacking. The criteria of strength of association, specificity, biological gradient, plausibility, coherence, and experimental evidence as outlined by Dr. Austin B. Hill,s and endorsed by EPA6, are not satisfied by the current body of association studies. Since a "safe" level for PMlO has not been identified, an estimate of a margin of safety, if there is one, for the PMlO standard cannot be made. The field must await the results of more specific research which addresses the Hill criteria before such estimates can be made with confidence. Both ozone and PMlO irritate the eyes, nose, throat, and lungs. About 14 to 15 percent of individuals over 55 years of age suffer to some extent from chronic obstructive pulmonary disease. For these individuals and for all who suffer from asthma, bronchitis, or other respiratory diseases, elevated levels of air pollution have an immediate and detectable impact on symptoms. Prolonged and daily exposure to respiratory irritants are believed to increase the risk of developing chronic obstructive pulmonary disease.7
References 1. Folinsbee, L.J. & Horvath, S.M. (1986). Persistence of the acute effects of ozone exposure. Aviat Space Environ Med, 57, 11361143.
2. United States Environmental Protection Agency. OAQPS Staff Paper. (1996). Review of the national ambient air quality standards for particulate matter: Policy assessment of scientific and technical information. Page VII-2. (EPA Publication No. EPA-452lR-96013). Research Triangle Park, North Carolina: Office of Air Quality Planning and Standards. 3. Lyon, J.L. Mori, M. & Gao, R. (1995). Is .there a causal association between excess mortality and exposure to PM-10 air pollution? Additional analyses by location, year, season and cause of death. Inhalation Toxicology, 7, 603-614. 4. Lyon, J.L. (1997). Personal communication. University of Utah Health Sciences Center. Department of Family and Preventative Medicine, Salt Lake City, Utah. 5. Hill, A.B. (1965). The environment and disease: Association or causation. (Presidential address). Proceedings of the Royal Society of Medicine, 58, 295-300. 6. United States Environmental Protection Agency. (April 1995). Air Quality Criteria for Particulate Matter, Volume III of III, pages 12-5 - 12-6. Office of Research and Development, Office of Health and Environmental Assessment, Environmental Criteria and Assessment Office. (EPA Publication No. EPAl600lAP-951001). 7. Pope, 111, C.A., Thun, M.J., Namboodiri, M.M., Dockery, D.W., Evans, J.S., Speizer, F.E., & Heath, Jr., C.W. (1995). Particulate air pollution as a predictor or mortality in a prospective study of U.S. adults. American Journal of Respiratory and Critical Care Medicine, 151, 669-674.
About the Author Steven C. Packham is the manager of the cost benefitlrisk assessment section o j and the toxicologist for, the State of Utah Division of Air Quality. He received his Ph.D. in medical psychology from the University of Oregon Medical School in 1973. He has been a diplomat of the American Board of Toxicology since 1982.
Utah's Health: An Annual Review 1996
23
State of Utah
Areas exceeding National Ambient Air Quality Standards
Ozone
East Tooele County
Utah Division of Air Quality April, 1994
Utah Health Print: Two Perspectives on Utah's Health Reform Thoughtful Progress by Patrick J. Johnson The 1992 Presidential Campaign fostered intense focus on health care reform. Regardless of how one felt about the Clinton proposal there is little question that health care reform was propelled to the top of the public policy agenda. In the end, however, it became clear that the Health Security Act of 1993 simply tried to do too much too soon. Much of the debate focused on the role of government vis-8vis that of the private sector. The various states watched the development of the health reform agenda in the nation's capitol with great interest and no small amount of trepidation and concern. There were audible signs of relief in most state capitols when the President's proposal met its demise. The states were not merely observers, however. Health care reform initiatives became a central focus of many governors and state legislatures. While the Clinton plan was unacceptable, state elected officials recognized that rising health care costs, lack of access and concerns about the quality of care all needed to be addressed. Utah was no different. Historically, health care costs in Utah were generally below the national average but were rising more rapidly than in many states. Some ten percent of the population was without access to health care due to the lack of health insurance. In addition, more sophisticated and comprehensive measures of quality and cost were needed. On the other hand, Utah consistently ranked among the top five states, relative to health care status, and had what most people considered to be an excellent health care system. Utah launched its health care reform initiative in 1993 under the leadership of Governor Mike Leavitt. The Governor and the legislature created the Health Policy Options Jury. The commission was comprised of legislators, community leaders and representatives from the business community. The options jury made a recommendation describing three different health care reform scenarios for the state to consider. The option favored by the Governor and the Legislature
was predicated on an incremental approach to addressing the issues of cost, access and quality. The recommendation was formalized through the creation of the Utah Health Policy The Commission and adoption of commission is comprised of thirteen members including the Governor who serves as chair, the Lt. Governor who serves as co-chair, six members of the Legislature and six representatives from the business sector, academia and the community. The commission is staffed by an executive director, health policy consultants and support staff. The commission employs a various technical advisory groups (TAGS) to study the various health care reform issues set forth in HealthPrint. Membership on the commission is restricted to nonstakeholders, i.e., health providers, carriers, etc., whose expertise and input in gathered through the TAG process. The health care reform process prescribed in HealthPrint is intentionally incremental. It is based on the belief that health care reform in the state of Utah must be done in a market oriented environment in order to fully incorporate the existing health care system, respect the political environment and strike the proper balance between the role of government and that of the private sector. Since its inception, numerous reforms have been implemented including the expansion of Medicaid to cover more children ages 12-17 and establishing a regulatory framework for the initiation of alliances to encourage like groups to come together to pool their collective buying power. The commission has also successfully proposed numerous small group insurance reforms that have enhanced portability, increased dependent coverage up to age 26 and open avenues to insurance for people with preexisting conditions. While many people are frustrated with what they perceive as a lack of progress or movement toward health care reform that is too slow, it is very important to note that only minor adjustments have been necessary in the reforms that have been implemented in Utah. In many states, including Washington, broad sweeping reforms have been implemented and subsequently repealed because of the injury to the market and other problems. Thus, the general philosophy of HealthPrint is working because it is thoughtful and deliberative in
m.
Utah's Health: An Annual Review 1996
25
nature. Healthprint has proven that moving slowly and carefully is preferred over rapid action that must be undone because of adverse outcomes.
Lost on the Road to Reform by Bill Crim I remember sitting with a group of uninsured Utahns shortly after Governor Leavitt unveiled his "flexible master plan" for health care reform. Most of them were too poor to afford private insurance, yet unable to qualify for Medicaid. Their disappointment was crushing as I explained that HealthPrint would not be an immediate solution to their problem. Despite its promise to establish "a rational process for providing affordable health care coverage for all Utahns," I could see their hope fade as we analyzed each person's situation against the multi-year time frames and questionable assumptions of HealthPrint. Now, three years later, we find ourselves trying to figure out what effect HealthPrint has had. There is no doubt about the countless hours of well-intentioned hard work put in by the Health Policy Commission staff and numerous volunteers. But has HealthPrint had a noticeable impact on those uninsured Utahns it was designed to help? I'm afraid not. As much as I'd like to look optimistically at the small gains that have been made, I can't help but notice that there are still between 150,000 and 200,000 Utahns who don't have any coverage at all-and prospects for their future coverage seem dim. HealthPrint has produced its annual quota of legislation-some of it quite beneficial to small groups of people. But without exception, accomplished "reforms" have been politically easy and relatively insignificant in their effect on the central problem of providing affordable coverage to the bulk of uninsured individuals. The "golden child" of market based health care reform-the Medical Savings Account (MSA)-has failed to produce a single properly filed MSA tax form. Open Enrollment requirements were effectively delayed by the insurance industry and then manipulated to allow the exclusion of even more Utahns from the insurance market. The main hope for the uninsured working poor-Medicaid expansion-
26 Two Perspectives on Utah's Health Reform
has been indefinitely delayed because no one wants to pay the cost. HealthPrint only mentions, but does not assume state responsibility for covering the very large segment of working poor Utahns who earn between 100% and 150% or the federal poverty level. With the main tools for expanding coverage having proven ineffective, "too expensive," or both, the original vision behind HealthPrint has become obscured by a myriad of study items which tinker at the edges of health policy, but do little to make insurance affordable for the working poor. The fact that HealthPrint has not reached its primary destination, and in fact seems lost altogether, leads me to ask if it was ever on the right road at all? Several of Healthprint's basic assumptions seem problematic. Most obvious is the assumption that large numbers of working poor families can be covered under Medicaid and paid for entirely with savings from capitation and administrative efficiencies. To be sure, there were savings generated in the Medicaid system-but never enough to cover the bulk of the uninsured population. The fact that the Legislature raided the savings for three years straight highlights another problem-using Medicaid as the means to insure the working poor is, at best, a temporary fix. Without stronger state and federal leadership, Medicaid will remain a vulnerable program which cannot be counted on from year to year to provide coverage for low-income Utahns. Second, cost containment strategies in HealthPrint rely almost entirely on faulty assumptions about the ability of enhanced market forces to control costs. In order for competition to control costs, a truly FREE market must exist, in which the laws of supply and demand are operative, and in which the consumer can be fully knowledgeable, has the ability to pay the entire cost of the goods, and is free to choose not to transact (i.e. does not lose money, health or life by choosing not to transact). None of these basic market principles applies to the health care situation. Finally, HealthPrint perpetuates the myth that figuring out how to reform our health care system is a complex task. The Health Policy Commission and its numerous Technical Advisory Groups (TAGS) are mired in endless discussions of policy minutiae, which taken individually are worthwhile, useful discussions
to have-but collectively they do not add up to the kind of comprehensive health care reform Utah needs. There is absolutely no mystery about how to provide coverage to the tens of thousands of people who don't have it-you can either require individual coverage or employer-based coverage with adequate subsidies and cost controls, or you can have a Canadian-style insurance system. What is enormously difficult is finding the political will to implement any of the possible solutions. It is ironic that if Governor Leavitt had remained committed to his original plan of using a "decision jury" to make proposals to the public for a non-binding referendum, the political will to move forward may actually have developed. This year's "hot" political issue-the urgent need to rebuild I-15-seems like it could be instructive for Utah citizens and policy-
makers who are concerned about where HealthPrint is leading us. Notice what happens when Governor Leavitt and the state's main political and business leaders agree on the need to solve a problem. A ten year job is scheduled for completion in 4 years. A massive, publicly funded media campaign is devised to educate citizens. The State Legislature commits to come up with at least $1.2 billion dollars to fund the solution (a significantly higher figure than that required to bring all uninsured Utahns into the health care system). I could go on . . ., but there is no doubt that we can solve problems when we put our mind and our political will to it. For the HealthPrint map to get us where we need to go, Governor Leavitt must initiate and support a substantial change in direction and focus for Health Print, and access to health care must be given the same political and financial priority as the reconstruction of 1-15.
About the Authors Patrick J. Johnson is the Executive Director of the Utah Health Policy Commission. He is also the Director of Government Relations for the Utah Department of Health. He is a graduate of the University of Utah's Master of Public Administration Program. Bill Crim is a long time advocate for health care reform. He received his B.A. in Political Science from the University of Utah in 1991. He works for Utah Issues Information Program.
Utah's Health: An Annual Review 1996
27