Having a Sleeve Gastrectomy
Hope Building Upper G.I. / Bariatrics 0161 206 5062 © G14040703W. Design Services, Salford Royal NHS Foundation Trust, All Rights Reserved 2014. Document for issue as handout. Unique Identifier: SURG24(14). Review date: August 2016
This booklet aims to describe:
What is a Sleeve Gastrectomy?
l What is a sleeve gastrectomy
page 2
l How is the operation performed
page 3
l How the surgery works.
page 3
l The risks and benefits associated with the operation
page 4
l What are the results of the operation
page 6
l Will I need medication when I go home
page 6
l Recovering from the operation
page 7
l Additional information
page 8
l Becoming pregnant after surgery
page 8
l Further information and useful websites
page 9
Alongside this information booklet you will also need to read “Having bariatric surgery”
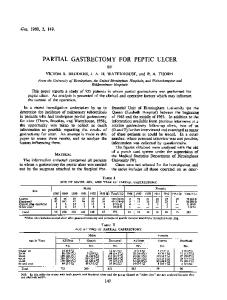
Is a type of weight-loss surgery that is mainly Restrictive. The surgeon removes approximately 60-80% of the stomach, permanently reducing its size so that the remaining stomach resembles a tube or sleeve, the remainder of the stomach is then removed and disposed of. As such when you eat food it enters the new stomach / sleeve and follows the same route as it did before (unlike the gastric bypass).
New stomach pouch
Stomach that is removed
As such there are less absorption difficulties than the bypass. The surgery usually takes about 1 to 2 hours. However, you maybe away from the ward a little longer as you spend sometime in the anaesthetic room before your surgery and in recovery after the operation.
1
© G14040703W. Design Services, Salford Royal NHS Foundation Trust, All Rights Reserved 2014. Document for issue as handout. Unique Identifier: SURG24(14). Review date: August 2016
2
How the operation is performed l The procedure is done using a Keyhole (Laparoscopic) technique l You are put to sleep using a general anaesthetic l The surgeon then makes five small cuts (1-2cm) on your abdomen l Gas is then injected into the abdomen to “blow out the abdominal wall. This enables the surgeon to see the internal organs more clearly l A small tube-like camera is inserted through one of the cuts to view the area of the operation; this is then shown on a large screen l The operation is then carried out using various instruments through the other cuts in your abdomen l Your stomach is stapled to create a thin tube or sleeve, with the excess part of the stomach is removed via one of the cuts 3
The risks and benefits associated with the operation l The gas is then released from your abdomen
Risks:
l The cuts are then closed with either dissolvable stitches or clips
There are risks associated with any type of surgery. Some of the complications that may occur with this operation include:
How the surgery works
l Complications associated with the general anaesthetic
The surgery works in two ways:
Restriction: By reducing the size of the stomach, only small amounts of food can be eaten at any one time, but your appetite is still satisfied.
Reduction in appetite: The part of the stomach that is removed produces an appetiteinducing hormone called Grehlin. After the procedure the hormone is greatly reduced. It is important to remember that this surgery is a tool to aid weight loss after surgery and to maintain it in the long term you must continue to work on your diet and life style.
l Chest infection: people who smoke must stop for a minimum of two weeks before surgery; otherwise your operation will be cancelled on the day l Wound infection; this is rare after laparoscopic surgery. Prophylactic antibiotics are given during the surgery
l Clots in the legs and /or lungs; to minimise the risk, you will be given elastic stockings to wear before the surgery and will be advised to keep them on for 2-3 weeks afterwards. You will also receive a small injection under your skin to thin your blood before surgery and will be sent home on a course of injections for a minimum of 5 days (a nurse will show you how to administer this injection yourself) l There is an approximately 1% risk of a leak from the newly formed staple line along the stomach. This is tested routinely near the end of the operation by using a special blue dye to make sure that it is water tight l While the surgery is a relatively safe procedure the nationally this operation has a mortality rate of 0.5%
© G14040703W. Design Services, Salford Royal NHS Foundation Trust, All Rights Reserved 2014. Document for issue as handout. Unique Identifier: SURG24(14). Review date: August 2016
4
Benefits l Some patients might develop gastro-oesophageal reflux disease (GORD) after restrictive operations such as sleeve gastrectomy or gastric band. This is more likely to occur if you stretch your stomach and if one eats late at night. Adjusting your eating habits and taking medications that reduce stomach acidity tend to help, but in extremely rare instances your surgeon might have to consider conversion to gastric bypass. If you already suffer with GORD, then a sleeve gastrectomy might not be the best choice, although reflux does indeed improve in some patients with weight loss. If your surgeon detects a hiatus hernia at the time of sleeve gastrectomy, this will be repaired and could bring about improvements in your reflux symptoms
5
l On average people tend to achieve approximately 60% excess weight loss (EWL) within the first year of surgery. EWL is defined as any extra weight above the upper limit of the normal body mass index (BMI) of 24.9 kg/m2 l Ability to exercise more comfortably, compared with open surgery l A reduction in complications associated with obesity which can include but not limited to high Blood pressure, Diabetes, Heart disease, Respiratory disease, Increased risk of cancer, Infertility, Improved self-esteem
What are the results of the operation? On average people lose between 55-65% of their excess weight in the first 1-2 years. After that, your weight will usually stabilise. Ideally you will see a marked improvement in obesity-related complications such as diabetes and heart disease. Approximately 10% of patients may regain weight in the long term if they continue to overeat, stretching the stomach and thereby reducing the restrictive effect of the procedure.
Will I need medication when I go home? YES You will be given a discharge prescription before you go home. This will have all the medications you require. All your medications will be supplied in a form that will allow you to take them while on a liquid diet. You will need to arrange a repeat prescription from your G.P before they run out. What you will be given:
Painkillers: Paracetamol and possibly codeine which should be sufficient on discharge.
Antacid: This is given to reduce the amount of acid in your stomach which will enable your stomach to heal this is extremely important and you will be asked to take these for 6 weeks.
© G14040703W. Design Services, Salford Royal NHS Foundation Trust, All Rights Reserved 2014. Document for issue as handout. Unique Identifier: SURG24(14). Review date: August 2016
6
Anti-coagulation therapy You will be given small injections of heparin to have once a day for a minimum of 5 days, in order to prevent clots in the legs and lungs. You will either be taught to give the injections to yourself before you go home or referred to the district nurse.
Vitamin and Mineral supplements: Your G.P will be asked to start you on iron and multivitamin supplements approximately 3 weeks after your operation Some patients may require further supplementation following surgery, such as calcium and vitamin D.
Your normal medications Will be altered to allow you to take them on a liquid diet. Diabetes medications maybe reduced immediately following your surgery. However as you begin to lose weight your G.P should review your medications on a regular basis. 7
Recovering from the operation It is important to stay mobile after the operation and gentle exercise is very much encouraged. Your wounds will take approximately 1-2 weeks to heal and you are advised to avoid heavy lifting or straining during this time. You should start to build your exercise tolerance such as swimming, brisk walking or going to the gym and aim for four 30 minute sessions per week. Your ability to exercise will improve dramatically following your surgery. As you are aware exercise helps weight loss by burning off extra calories and helps build muscle tone and to a lesser extent, excess skin that results from surgery. You may resume driving 10-14 days following your operation. You should be able to competently carry out an emergency stop and no longer be on strong pain killers. Most people return to work 1-2 weeks following their operation.
Additional information: What will happen if I decide not to go ahead with surgery? You will be referred back to your G.P or referring consultant for conservative (medical) weight management.
What are the alternatives to this procedure? There are alternative surgical and medical treatments available. If you wish to discuss these further you should contact the consultant secretary to arrange a further appointment.
Becoming pregnant after surgery Obesity can cause infertility, but following weight loss surgery ovulation and periods can recommence. Pregnancy is safe after surgery, reduces the risk of miscarriage, high blood pressure and diabetes. However patients are advised not to get pregnant for the first 12 months after surgery, to allow the weight loss to slow down and establish a regular eating pattern. If you were to get pregnant it is advised that you should your dietician and G.P to ensure that you are having all the nutrients you and your baby require. Once you become pregnant you are advised seek medical advice on the medications you are taking to ensure they are suitable for pregnancy. There is no reason why you should not have a normal delivery and be able to breast feed after surgery.
© G14040703W. Design Services, Salford Royal NHS Foundation Trust, All Rights Reserved 2014. Document for issue as handout. Unique Identifier: SURG24(14). Review date: August 2016
8
Further information: Support is available through Salford Royal NHS Foundation Trust:
Specialist Nurse
0161 206 5062
(voicemail service)
Dietitian
0161 206 1223 Secretary
0161 206 0449 Hospital switchboard
0161 789 7373 Useful websites: British Obesity Surgery Patient Association (BOSPA)
www.bospauk.org
08456 020 446
9
Notes British Obesity and Metabolic Surgery Society (BOSS)
www.bomss.org.uk
02073 044 786 Weight Loss Surgery Information and Support (WLSinfo)
www.wlsinfo.org.uk
0151 222 4737 Weight Loss Resources UK www.weightlossresources. co.uk
01733 345 592
Drinkaware – alcohol advice
www.drinkaware.co.uk
020 7766 9900 Salford Royal Bariatric Service
http://www.srft.nhs.uk/ bariatric/
© G14040703W. Design Services, Salford Royal NHS Foundation Trust, All Rights Reserved 2014. Document for issue as handout. Unique Identifier: SURG24(14). Review date: August 2016
10
© G14040703. Design Services Salford Royal NHS Foundation Trust All Rights Reserved 2014 This document MUST NOT be photocopied Information Leaflet Control Policy: Unique Identifier: SURG24(14) Review Date: August 2016
For further information on this leaflet, its references and sources used, please contact 0161 206 5062 Copies of this information are available in other languages and formats upon request.
If you need this interpreting please telephone
In accordance with the Equality Act we will make ‘reasonable adjustments’ to enable individuals with disabilities, to access this treatment / service.
Under the Human Tissue Act 2004, consent will not be required from living patients from whom tissue has been taken for diagnosis or testing to use any left over tissue for the following purposes: clinical audit, education or training relating to human health, performance assessment, public health monitoring and quality assurance. If you object to your tissue being used for any of the above purposes, please inform a member of staff immediately.
Salford Royal operates a smoke-free policy. For advice on stopping smoking contact the Hospital Specialist Stop Smoking Service on 0161 206 1779
Salford Royal NHS Foundation Trust Stott Lane, Salford, Manchester, M6 8HD
If you would like to become a Foundation Trust Member please visit:
If you have any suggestions as to how this document could be improved in the future then please visit:
Telephone 0161 789 7373
www.srft.nhs.uk/ for-members
http://www.srft.nhs.uk/ for-patients
www.srft.nhs.uk