07-04-2010
Aiming Higher: A Workshop for LCI‐DK Glenn Ballard Copenhagen March 22, 2010 Graphic courtesy of Extemin: 27th annual mining conference, Arequipa, Peru
Glenn Ballard – a brief CV • Experience – Pipefitter, Foreman, Construction Engineer, Productivity & Quality Specialist, Internal Management Consultant for Brown & Root and Bechtel – Independent Management Consultant. Clients include Petroleos de Venezuela, U.S. Dept. of Energy, Pacific Gas & Electric, Koch Refining, BAA (Heathrow Terminal 5), Channel Tunnel Rail Link (St. Pancras Station)
• Current Position – Professor in the Engineering & Project Management Program, Dept. of Civil & Environmental Engineering, UC Berkeley – Research Director, Project Production Systems Laboratory, UC Berkeley
• Education – M.B.A. – PhD (Civil Engineering)
• Co‐founder – International Group for Lean Construction (1993) – Lean Construction Institute (1997)
1
07-04-2010
Today’s Program 09:30 Desired Outcomes and Agenda, Self‐Introductions 09:45 LCI News 10:30 Integrating within and across projects 11:30 Break 11:50 Creating a lean culture: Learning from breakdowns 12:50 Lunch 12:50 Lunch 13:50 Creating a lean culture: The role of supervision 14:50 Workshop Plus/Delta 15:00 Adjourn
LCI News • The number of LCI chapters in the U.S. – JJanuary 2008 = 2008 0 – January 2009 = 6 – January 2010 = 22
• Negotiations are underway with the major industry associations to fund LCI as a think tank. • There is a movement within the board of directors to make LCI an international organization.
2
07-04-2010
LCI News • Affiliates are growing and active – In December 2009, LCI Germany hosted an I D b 2009 LCI G h t d international conference on Lean in Public Sector Construction – LCI Finland has enrolled major industry players in collaborative research, with a budget >1 million Euro’s – I spoke last Thursday to an LCI Norway meeting with more than 100 people and will speak at a LCI Sweden meeting in Malmo this Wednesday
LCI News • University‐based research centers supporting LCI h t LCI chapters are also growing. Now include: l i N i l d – University of California, Berkeley – University of Washington – San Diego State University – Colorado State University Colorado State University – Michigan State University
3
07-04-2010
LCI News UC Berkeley’s Project Production Systems Laboratory has new and exciting research initiatives and projects: Lean in Public Sector Construction Owner Forum Skanska Nordic: Started in 2005 as supply chain management. Shifting to a lean enterprise focus. Skanska Norway to join Skanska Finland as P2SL contributors Statoil: Meeting the challenges of megaprojects U.S.A. Dept. of Energy: Reduce energy consumption in buildings Construction Industry Institute: Redesign the capital project delivery system from a blank sheet of paper. Research team members include Air Products, Proctor & Gamble, General Services Administration, Tennessee Valley Authority, Bentley Software Systems, and CH2M Hill
One more research project: Whole Life O h j t Wh l Lif Target Value Design
4
07-04-2010
Means
Ends
Conditions of Satisfaction
Sutter Fairfield Medical Office Building Sutter Fairfield MOB
Market benchmark = $22.0 million Target cost = $18.9 million Actual cost = $17.9 million
5
07-04-2010
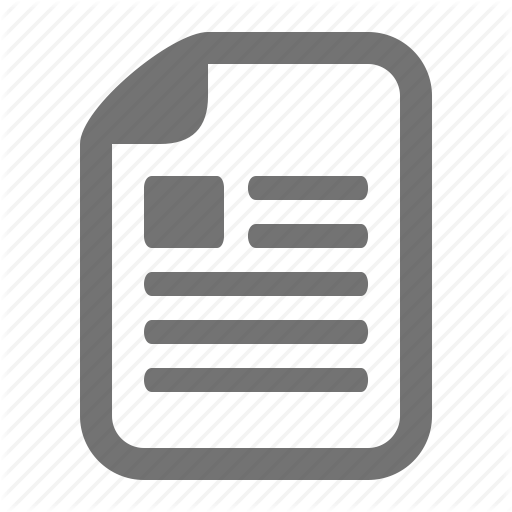
Cathedral Hill Hospital Project: Expected, Allowable & Target Cost
Allowable Cost for Construction (normalized for changes in scope)
Two outcomes of TVD that look to be repeatable (at least within the healthcare and education sectors) 1. Expected cost falls as design develops. 2. Projects are completed below market cost— so far as much as 19% below.
6
07-04-2010
Why Change a Winning Game? To enable better investment of cost savings in order to generate greater customer value d t t t t l On the case study projects, cost savings were assured late in the project, when investment opportunities had shrunk How can we make opportunities had shrunk. How can we make investments when the lever arm is longer?
Relative Costs
7
07-04-2010
What Changes? • Give the design team a tool to calculate the i impact of design alternatives on facility life t fd i lt ti f ilit lif cycle costs and benefits. • Keep the budget alive during design, recalculating the allowable and target cost based on the anticipated impact of design p p g alternatives on life cycle costs and benefits.
Challenges 1. Persuade clients to develop an operations cost model and use it to calculate their return on investment, and hence what they are willing to invest to get that return. 2. Persuade clients to give the operations cost model to the design team. 3. Learn how to link the product and operations models so changes in the former are reflected in the latter. 4. Persuade financiers to allow a floating budget during design. 5. Learn how to design to a moving target.
8
07-04-2010
Conclusion of LCI Report • What are the key points for you from this session? i ? • What questions have been provoked?
Today’s Program 09:30 Desired Outcomes and Agenda, Self‐Introductions 09:45 LCI News 10:30 Integrating within and across projects 11:30 Break 11:50 Creating a lean culture: Learning from breakdowns 12:50 Lunch 12:50 Lunch 13:50 Creating a lean culture: The role of supervision 14:50 Workshop Plus/Delta 15:00 Adjourn
9
07-04-2010
Outline • What’s meant by “integrate”? • Who can initiate, with what scope for action? Wh i ii ih h f i ? • What can be done?
Aspects of Integration • Align the interests of companies • Build one organization out of individuals from different companies • Coordinate the actions of individuals and work groups toward shared objectives
10
07-04-2010
Owner
Architect
CE
General Contractor Other
SE
CC
EE
Other SC
ME
EC MC
Owner
Architect
CE
General Contractor Other
SE
EE ME
CC
Other SC
EC MC
Traditional Contract Structure
11
07-04-2010
Owner
Architect
CE
General Contractor Other
SE
CC
EE
Other SC
ME
EC MC
Example: Sutter Health Integrated Form of Agreement
Owner
Architect
CE
General Contractor Other
SE
EE ME
CC
Other SC
EC MC
Example: IPD (Orlando, Florida)
12
07-04-2010
13
07-04-2010
Mountain Climbers • If one Primary Team Member makes a mistake each Primary Team Member will pay for it hP i T M b ill f it • Cost reductions anywhere are shared among those in the Partnering Agreement and with the Client • An overrun on the project will reduce the An overrun on the project will reduce the gross profit available for distribution
14
07-04-2010
Who can initiative integration, with what scope for action? • Everyone on a project has some scope for action, even a foreman restricted to her own work even a foreman restricted to her own work group. • Owners have the greatest scope for action, followed by the “process managers” for design and for construction (architects and general contractors). ) • Design and construction specialists can integrate within their individual work, but can also reach out to others and offer to work together.
The 5 Big Ideas
15
07-04-2010
16
07-04-2010
Preferred Partners Companies that have provided greater value without reducing their own profitability Companies with which you have improved shared processes to mutual advantage Companies that meet minimum requirements: safety records and programs, financial stability, licenses, etc. All companies that claim a specific competence
17
07-04-2010
Conclusion of Session • We have looked at a few examples integrating within and across projects. ithi d j t • Can you share examples of your own? • What are the key points for you from this session? • What questions have been provoked? What questions have been provoked?
Today’s Program 09:30 Desired Outcomes and Agenda, Self‐Introductions 09:45 LCI News 09:45 LCI News 10:30 Integrating within and across projects 11:30 Break 11:50 Creating a lean culture: Learning from breakdowns 12:50 Lunch 13:50 Creating a lean culture: The role of supervision 14:50 Workshop Plus/Delta 15:00 Adjourn
18
07-04-2010
Breakdowns • …are deviations from target outcomes • …provide learning opportunities: Our knowledge regarding is inadequate. • Types of breakdowns – Near misses, accidents, injuries Near misses accidents injuries – Errors, defects, rework – Broken promises, plan failures
Walter Shewhart’s PDCA Cycle Plan
Act
Do
Check
19
07-04-2010
Plan •Form a testable hypothesis in the form If A, then B. •Specify a current standard; i.e., a basis of comparison. •Describe how and when the experiment will be conducted. •Specify a follow up plan; how the experiment •Specify a follow‐up plan; how the experiment will be evaluated; what will count as evidence that the new method is superior to the previous standard.
Plan‐an example •Problem: I spend lots of time searching for documents in my office. •Hypothesis: If I organize my paper files and keep them organized, I will spend less time looking for things. •Basis of comparison: I have previously listed my paper file folders, but have not kept the list updated. There are piles of unfiled papers on various surfaces in my office. I guesstimate that I spend 20 minutes a day searching for documents. •How the experiment will be conducted: 5S the office •How the experiment will be conducted: 5S the office, including file folder organizing. Complete by the end of the day Sunday, July 27. •Follow‐up plan: Perform the experiment, then measure how much time is spent each day searching for things.
20
07-04-2010
Do Execute the experiment; carry out the plan
Check Measure outcomes Measure outcomes Evaluate outcomes against base line Decide if there is additional room for improvement If so, go back to PLAN If not, go to ACT
21
07-04-2010
Act Put the new process or standard into practice Put the new process or standard into practice: •Change policies or procedures •Educate and train to enable successful performance •Align reward systems
The PDCA Cycle in First Run Studies •A detailed plan for an operation developed prior to starting work, structured to achieve safety, quality, time and cost objectives. •The plan is developed with those involved in doing the work, tested and improved. •Includes timing and location g of activities, work flow, balanced work load, tools, release of work downstream, etc. •The actual process is recorded and analyzed to identify improvements.
PLAN 1. Select work processes to study. 2. Before the first run of each process, assemble people with input or impact. 3. Chart the work process steps. 4. Brainstorm how to eliminate, reduce or overlap process steps. 5. Check process designs for safety; anticipate hazards and specify preventions. 6. From past experience, list probable errors and specify preventions. Plan for feedback and learning by identifying key variables to observe or data to collect. 7. Assign optimum labor, tool and equipment resources.
ACT 10. Reconvene the team, including those who actually did the work, review data and share ideas. Continue until opportunity for improvement is exhausted.
DO 8. Carry out the plan on the first run.
CHECK C C 9. Describe and measure what actually happens: - process steps, sequences and durations - interactions with other operations or crews - errors, omissions and rework - accidents, near misses and hazards - resources used (labor, tools, equipment, support crafts, etc) - outputs
44
22
07-04-2010
A PDCA Cycle for Learning from Breakdowns Prevent
Analyze
Detect
Correct
Prevent •Preventive action depends on our understanding of causation; what causes various types of breakdowns. •When breakdowns occur despite our efforts to prevent, that tells us we have something more to learn about cause and effect.
23
07-04-2010
Detect
When breakdowns do occur, we want to detect them as close to their point of origin as possible, to contain the damage. That is one of the good arguments for small batches and for self inspection.
Correct Once detected, the first step is to take corrective Once detected the first step is to take corrective action. For example, if we have an error in a drawing, we correct the error and replace the drawing.
24
07-04-2010
Analyze But corrective action is not enough if we B i i i h if want to prevent reoccurrence. We must analyze the breakdown to understand why it happened in order to understand causality. That’s the only way we can prevent reoccurrence.
Composite PDCA Cycle Check
Act Prevent
Do Plan
Detect Analyze
Correct
25
07-04-2010
Prevent • Design products to reduce the possibility or probability of safety or quality breakdowns in probability of safety or quality breakdowns in their construction. • Design and test operations against safety, quality, time and cost criteria (virtual and physical prototyping, first run studies) • Mistake proof where possible Mi t k f h ibl • Make evident the purposes and values behind design criteria
Spacers •Anchor bolts must be spaced p evenly and cast into concrete to protrude from the surface so that light poles can be mounted and plumbed. •AJ Speedset™is an adjustable jig that creates a simplified, time saving way to install ¾”, 1”, 1¼” or 1½” anchor bolts in concrete for area lighting.
Source: http://www.rndproducts.com/
26
07-04-2010
AEC Examples of Mistake‐proofing
Color Coding on Site •Color coding shows locations for sheet metal locations for sheet metal straps and pipe hangers.
•Source: John Mack, Southland Ind., presentation at 2007 LCI Ann. Conf.
Used with permission from Per‐Erik Josephson, Chalmers University
27
07-04-2010
Detect (…as closely as possible to its point of origin) Use small batches Do self inspection Do successive inspection Mistake proof detection where possible Promote ‘family feeling’ among team members (to encourage speaking up) • ‘Capture’ errors before they become defects
• • • • •
Color Coding •The heads of these pneumatic pneumatic nails have nails have different colors to correspond to different lengths and diameters. This makes it easy to verify whether or not nails y were installed according to a nailing schedule.
28
07-04-2010
Luotettavuusmittaus, Laboratoriotyömaa Vt 2 Vihti - "Miksi" -kokooma pos Vko
4
Take out the stubs and the 13 little trees 13Take out the topsoil Excavation and cleaning of 13 the rock on E1R2 The rock bank on E2R2 this was extra work that was not in the schedule in the 13 beginning
5
13Crushing of 0-56
6
13The rock bank E2R3
7
13The finishing of the slopes Removing the temporary road and building it to 14 another place Topsoil and excavation 500 50014 740 14Stubs and little trees 14Crushing 14The blasting on 2000-2050 Shaping of the rock bank 14 with crushed aggregate 14Excavation on 2500-2700 14The cut of trees
1 2 3
8 9 10 11 12 13 14 15
Why 1 Machine was in another place. The surface was clay and wet The building of the temporary road took longer than expected
Instead of building the rock bank the crusher was took on this place Test use, the power was not what expected The blasting takes longer than expected, the daily amonts were not achieved The soil thought to be used in here was not suitable for the slopes
16
14The temporary road on S5
17
15Rock bank on 500-740
Lack of equipment
18
15Rock bank E1R1 Removing of top soil and excavation including the 15 cleaning of the rock
Lack of equipment
20 21 22 23 24 25 26 27 28 29 30 31 32 33 34 35 36 37 38 39 40 41
Why 3
Whys Machine was in another area of the project (in Huittinen) The soil was clay, which was not expected
Not important, doesn't affect other work Examination is expensive
Wet place
The soil was different than expected
Decieded that the crusher in this place would be reasonable
At this point the crushed aggregate
The planned buying of the crushed aggregate was more expensive
The blasting had to be done in smaller amounts
The traffic can only be stopped for 12 minutes
The rock will fall on the road
Prices for the rock got up
Instead of building the bank, we took the crusher to this location The crusher was tested and it didn't achieve the power expected
Didn't achieve the amount Soil not suitable for the slopes
Machine breakdown Decieded not to take all out because of the temporary road. The machine working in Huittinen Curshed more than expected The power was more than expected Was finished early The power was more than expected The bank was not in the right level Clay, will be used for slopes later Was finished early There was not suitable material for the suitable soil for the temporary road
19
Why 2 Huittinen site manager was more convincing The soil was not examined before
The operatior was unexperienced
Machine breakdown Part of the soil was left to use in a workroad Worked in another area of the project Crushed more than expected Finished early The bank not finished - must be elevated Clay - will be used for slopes later on Finished early
No suitable soil for bank Limited possibilities to influence the subcontractors equipment The contract Limited possibilities to influence the subcontractors equipment The contract
Didn´t achieve the amount expected Crossing the road takes longer than 15Loading the rock on E2R2 expected The amount of traffic We're still learning 15Moving of the electrical line No maintenance window The removing of the stubs 15 and small trees The stubs are not collected 16Rock bank on E1R1 Same as nro 13 The removing of the top soil 16 and excavation More soil than expected Insufficient data More traffic than expected 16Blasting 16No rock - > No haul 16no haul -> no bank 17The blasting on E1R1 More soil than expected 17 Changed the work order, sheet piles 17The pile slab was put in earlier than expected The desicion of the subcontractor to 17The rock bank 2150-2700 Not finished, no machine take the machine to another job Difficult place, took some time before 18The rock bank E1R1 we could make the solution 18 18Changing the soil The operator was sick 18Changing the soil The operator was sick 22Rock bank The operator didn't show up 22Rock bank The operator didn't show up 23Excavation An error (not a fatal one) Worked only for two days, took the 23The excavation on E2R2 machine to another job The subcontractors decision The machine arrived on Thursday 23The blasting instead of Monday The sub 23The rock bank No machine even though planned It wasn't sure if the for of the storage
Lack of equipment Lack of equipment
Didn't achieve the amount The traffic is too high for the trucks to cross the road No window to move the power line The stubs are taken out but not gathered Bank must be elevated More soil than expected Higher traffic than expected Higher traffic than expected Higher traffic than expected More soil than expected More soil than expected Workorder was changed Not final work not ready, no machine No workmotivation No workmotivation The operator was sick The operator was sick The operator didn't show up The operator didn't show up No plans, error of judgement
The machine didn't arrive to the site until Thursday No bulldozer
29
07-04-2010
At your tables, discuss the question “What are you doing to learn from b kd breakdowns” ” Do that for 10 minutes, then pick a spokesperson to share with everyone.
Field Guide to Understanding Human Error By Sidney Dekker 1. Systems are not inherently safe or stable. Safety and stability is created by human action stability is created by human action. 2. “Human error” is not a useful finding from breakdown analysis. It doesn’t explain why what was done made sense to those who did it. 3. If it made sense to them, it’s likely to make sense to others in similar circumstances. 4. Knowing what would have prevented the breakdown does not amount to knowing how to prevent future breakdowns of the same kind. 5. Beware analysis based on hindsight.
30
07-04-2010
The Royal Majesty Accident On June 10, 1995, a passenger ship named Royal Majesty left St. Georges in Bermuda. On board were 1509 passengers and crewmembers who had Boston as their destination destination—677 677 miles away, away of which more than 500 would be over open ocean. Innovations in technology have led to the use of advanced automated systems on modern maritime vessels. Shortly after departure, the ship’s navigator set the ship’s autopilot in the navigation (NAV) mode. In this mode, the autopilot automatically corrects for the effects of set and drift caused by the sea, wind and current in order to keep the vessel within a preset distance of its programmed track.
Not long after departure, when the Royal Majesty dropped off the St. Georges harbor pilot, the navigator compared the position data displayed by the GPS (satellite‐based) and the Loran (ground/radio‐based) positioning systems. He found that the two sets of data indicated positions within about a mile of each other—the expected accuracy in that part of the world. From there on, the Royal Majesty followed its programmed track (336 degrees), as indicated on the automatic radar plotting aid. The navigator plotted hourly fixes on charts of the area using position data from the GPS. Loran oran was used only as a back‐up system, and when checked early on, it revealed positions about 1 mile southeast of the GPS position. About 34 hours after departure, the Royal Majesty ran aground near Nantucket Island. It was about 17 miles off course. The investigation found that the cable leading from the GPS receiver to its antenna had come loose and that the GPS unit (the sole source of navigation input to the autopilot) had defaulted to dead‐ reckoning (DR) mode about half an hour after departure. Evidence about the loss of signal and default to DR mode was minimal, contained in a few short beeps and a small mode annunication on a tiny LCD display meters from where the crew normally worked. In DR mode, there was no more correction for drift. A northeasterly wind had blown the Royal Majesty further and further west.
31
07-04-2010
From the investigation board’s report: “Thus, had the officers regularly compared position information from the GPS and the Loran‐C, they should not have missed the discrepant coordinates, particularly as the vessel progressed farther from its intended track.” There were sightings of things that were not on the intended route. The report says: “The second officer’s response to these sightings should have been deliberate and straightforward. He should have been concerned as soon as the BB buoy was not sighted and then again when the lookouts sighted the red lights. Additionally, the second officer should have checked the Loran‐C….”
What do you make of the investigation What do you make of the investigation board’s report? What needs explaining is why normal, professional seamen are liable to misinterpret cues, especially slightly ambiguous cues. The report does not provide an explanation. It simply says that the 2nd officer did not do what a good seaman would have done.
The Swissair 111 accident During the Swissair 111 flight, the crew noticed smoke in the cockpit. A diversion airport (Halifax) was in their vicinity, but they did not make an emergency descent, and never made it there. Instead, the pilots took time sizing up the situation, going through checklists, and making preparations for fuel dumping to reduce their landing weight. The developing fire caught up with them and rendered the aircraft uncontrollable. It crashed into the sea, killing everybody onboard.
How to analyze this breakdown? The following statements are from the accident investigation report. “When the pilots started their descent toward Halifax at 0115:36, they had assessed that h they h were faced f d with h an air conditioning d smoke k anomaly l that h did d d not require an emergency descent. Based on their perception of the limited cues available, they took steps to prepare the aircraft for an expedited descent, but not an emergency descent and landing.”
What do you make of this right off the bat?
32
07-04-2010
“The pilots were unfamiliar with the Halifax International airport and did not have the approach charts readily available. The back‐course instrument landing approach to Runway 06 was not pre‐programmed into their flight management system. The pilots knew that they would have to take additional time to familiarize themselves with, and set up for, the approach and landing. They were given the weather information by the crew of an overflying aircraft, but did not know the runway lengths or orientation. Having runway and instrument approach information available is normal practice and is important in carrying out a safe approach and landing, particularly at an unfamiliar airport at night. …The pilots also knew that the weight of the aircraft exceeded the maximum overweight landing limits for non‐emergency conditions. In addition to these flight management circumstances, the pilots were aware that the meal service was underway, and that it would take some time to secure the cabin for a safe landing. Given the minimal threat from what they perceived to be air conditioning smoke, and the fact that there were no anomalies reported from the passenger cabin, they would likely have considered there to be a greater risk to the passengers and cabin crew if they were to conduct an emergency descent and landing without having prepared the cabin and positioned the aircraft for a stabilized approach and landing. It can be concluded that the pilots would have assessed the relative risks differently had they known that there was a fire in the aircraft.”
Conclusion of Session • We have looked at a few examples of learning f from breakdowns. b kd • Can you share examples of your own? • What are the key points for you from this session? • What questions have been provoked? What questions have been provoked?
33
07-04-2010
Today’s Program 09:30 Desired Outcomes and Agenda, Self‐Introductions 09:45 LCI News 10:30 Integrating within and across projects 11:30 Break 11:50 Creating a lean culture: Learning from breakdowns 12:50 Lunch 12:50 Lunch 13:50 Creating a lean culture: The role of supervision 14:50 Workshop Plus/Delta 15:00 Adjourn
Supervisory practice: The key to creating and sustaining a lean culture •
The primary responsibilities of leaders in a lean p production environment: 1. 2. 3.
• •
Develop those who report to you. See that processes run as designed. Improve the processes.
Build standard supervision from bottom up so direct production is supported. Deploy standard supervision from top down; provide leadership.
Creating a Lean Culture/David Mann/Productivity Press Training Within Industry/Donald Dinero/ Productivity Press
34
07-04-2010
Going to gemba on the Cathedral Hill Hospital Project Observe meetings, formal or informal. Ask if it is okay to observe. Explain that you and other managers on the project are beginning the lean practice of ‘going to gemba’; i.e., going to where the work is happening in order to see what’s going on and to offer help. Listen for the language of reliable promising, for assumptions about value, for processes that constrain performance. When you feel y p g q ready and it is not disruptive to the meeting, ask questions to focus attention on what you have observed. Ask how you can help. If appropriate, get and make commitments to act. Plan to follow up on future gemba walks.
Reliable Promising 1 Request “Will You?” Will You?
Inquiry Accepted
Negotiation Submitted
PO Signed
CUSTOMER 4 Declare
Satisfaction
Conditions of
Conditions of Satisfaction Satisfaction & & Completion Date
Date of
“Thank you” y
COMMIT 2
“I Promise I WILL”
PROVIDER
Completion
3
Declare Complete “I’m Done”
35
07-04-2010
Going to gemba on the Cathedral Hill Hospital Project (continued) Note: The negotiation step in reliable promising is one thing to observe closely because it is where behavior impacts coordination. Let’s develop dialogues that illustrate di i L ’ d l di l h ill effective behavior; for example, the ‘customer’ making a request does so clearly and precisely, then after hearing the initial response, asks what change in the request would enable a commitment to be made, or would increase the probability of the commitment being met. Another example: the ‘responder’ always tests their understanding of the request by saying back what they heard and what of the request by saying back what they heard and what they understood it to imply. If they feel uncomfortable making a commitment, they explain their concerns and make a counteroffer.
Going to gemba on the Cathedral Hill Hospital Project (continued yet again) Talk with individuals. “Do you have a few minutes to talk about your work on the project?” If they do not, schedule a time to talk. If they do, “As you likely know, one of our project objectives is to encourage everyone to improve how their work is done. Would you please share how you have improved the way you do your job, or how you intend to improve the way you do your job?” p q y Listen to the response and question until understood. Ask how you can help. Get commitments/make commitments. Write them down. Plan to follow up on future gemba walks.
36
07-04-2010
Leader Standard Work The closer to production, the more a supervisor’s time is spent on repetitive, standard tasks such as team meetings, gemba walks with supervisors, training team members, planning the next day’s/week’s work, identifying and removing constraints on planned tasks, charting and posting visual controls. In repetitive manufacturing, 80% of a front line supervisor’s time is spent on standard tasks; but only 50% of a second level supervisor’s time, and even less further ‘up’ the organizational hierarchy.
At your tables, discuss the questions 1 “Are the 3 duties of the supervisor the right ones” y g y 2 “What are you doing or could you do to make that happen in your organization” Do that for 10 minutes, then pick a Do that for 10 minutes then pick a spokesperson to share with everyone.
37
07-04-2010
Conclusion of Session • We have looked at the role of supervision in creating and sustaining a lean culture. ti d t i i l lt • Can you share examples of your own? • What are the key points for you from this session? • What questions have been provoked? What questions have been provoked?
Today’s Program 09:30 Desired Outcomes and Agenda, Self‐Introductions 09:45 LCI News 10:30 Integrating within and across projects 11:30 Break 11:50 Creating a lean culture: Learning from breakdowns 12:50 Lunch 12:50 Lunch 13:50 Creating a lean culture: The role of supervision 14:50 Workshop Plus/Delta 15:00 Adjourn
38
07-04-2010
What would you like to discuss in the time remaining? • List • Use N/3 to share what’s in our heads • Select one or two topics to discuss in plenary session OR Get volunteers to lead table discussions on topics and the rest vote with their feet their feet
Plus Delta
39