0021-972X/90/7106-1474$02.00/0 Journal of Clinical Endocrinology and Metabolism Copyright © 1990 by The Endocrine Society
Vol. 71, No. 6 Printed in U.S.A.
Effect of Chronic Treatment with the Glucocorticoid Antagonist RU 486 in Man: Toxicity, Immunological, and Hormonal Aspects LOUISA LAUE, MICHAEL T. LOTZE, GEORGE P. CHROUSOS, KEVIN BARNES, D. LYNN LORIAUX, AND THOMAS A. FLEISHER Developmental Endocrinology Branch, National Institute of Child Health and Human Development (L.L., G.P.C., K.B., D.L.L.), the Surgery Branch, National Cancer Institute (M.T.L.), and the Immunology Service, Clinical Pathology Department (T.A.F.), National Institutes of Health, Bethesda, Maryland 20892
receptors with RU 486 was associated with marked compensatory elevations of plasma ACTH and cortisol and increases in 24-h urinary excretion of 17-hydroxysteroids and free cortisol. Unexpectedly, 8 of the 11 subjects developed generalized exanthem after 9 days of RU 486 treatment. One subject developed symptoms and signs consistent with the diagnosis of adrenal insufficiency. Total white blood cell counts, absolute lymphocyte, neutrophil and eosinophil counts, erythrocyte sedimentation rate, and quantitative immunoglobulins did not change with RU 486 therapy. Similarly, T-, B-, and natural killer cell subsets did not change during RU 486 treatment. Futhermore, functional evaluation of lymphocyte cytotoxicity and proliferation revealed no changes. We conclude that administration of high doses of RU 486 to normal volunteers does not result in measurable enhancement of immune function. This suggests that in man, glucocorticoids may not exert a tonic inhibitory effect on the immune system as they appear to do in rodents. Alternatively, the compensatory increase in endogenous cortisol may obviate any effect of the glucocorticoid antagonist on the immune system. RU 486, however, does cause a reversible generalized exanthem in a large proportion of normal volunteers when given chronically and at high doses, and caution from this perspective is recommended. (J Clin Endocrinol Metab 71:1474-1480,1990)
ABSTRACT. Suppression of immune function was traditionally thought to occur only with pharmacological levels of glucocorticoids. However, recent studies in rodents have suggested that glucocorticoids exert tonic antiinflammatory/immunosuppressive effects even at basal nonstress concentrations. To examine whether basal glucocorticoid secretion modulates immune function in man we employed the specific glucocorticoid receptor antagonist RU 486. If a tonic level of inhibition of the immune system by basal glucocorticoid levels was present, then a potentiation or enhancement of immune function might evolve in the absence of glucocorticoid action. To examine this hypothesis, we studied 11 healthy male normal volunteers who received RU 486 (10 mg/kg-day) or placebo vehicle, divided into 2 daily oral doses, for 7-14 days. Blood samples were collected every 2 days for measurement of plasma ACTH and cortisol concentrations along with 24-h urine samples for measurement of 17-hydroxysteroid and free cortisol excretion. Complete and differential blood counts, erythrocyte sedimentation rates, C-reactive protein, antinuclear antibodies, rheumatoid factor, and quantitative immunoglobulins were also determined at 2-day intervals. Leukocytes were obtained by leukopheresis for phenotypic characterization and functional analysis before and 7 days after the initiation of RU 486 or placebo therapy. Blockade of cortisol
W
HILE it is known that stress or "pharmacological" levels of glucocorticoids suppress immune function in mammalian organisms, the effect of physiological resting levels of glucocorticoids on the human immune system is unknown (1-3). Munck and Guyre (4, 5) have suggested that physiological levels of glucocorticoids may modulate the action of numerous intracellular mediators which regulate immune activity. Evidence in support of this hypothesis has come from studies demonstrating enhancement of the inflammatory response in adrenalectomized rats or in rats whose glucocorticoid action was blocked with systemic administration of a glucocorticoid receptor antagonist (6, 7).
It is not known whether blockade of the effects of endogenous cortisol leads to similar enhancement of the inflammatory/immune response in man. If this were the case, agents that block cortisol action might have potential therapeutic applications as immune enhancers. To examine this question we studied several measures of immune function in 11 normal volunteers before and during administration of the glucocorticoid receptor antagonist RU 486. This agent has been successfully used to treat patients with hypercortisolism and as an antiprogestational agent for birth control (8-11).
Received May 16, 1990. Address all correspondence and requests for reprints to: Louisa Laue, M.D., National Institutes of Health, Building 10, Room 10N262, 9000 Rockville Pike, Bethesda, Maryland 20892.
Subjects and protocol
Materials and Methods The study was approved by the Clinical Research Subpanel of the NICHHD. After giving informed consent, 11 healthy
1474
The Endocrine Society. Downloaded from press.endocrine.org by [${individualUser.displayName}] on 16 January 2017. at 08:52 For personal use only. No other uses without permission. . All rights reserved.
CHRONIC TREATMENT WITH RU 486 normal male volunteers, ranging in age from 19-35 yr, were enrolled in the study. The study was designed initially as a double blind randomized placebo cross-over format in which all subjects were to receive 14 days of RU 486 (or placebo) followed by a 14-day washout period before resumption of treatment for the remaining 14 days with placebo (or RU 486). All subjects received RU 486 at a dose of 10 mg/kg-day or placebo vehicle, administered orally in 2 divided doses, every 12 h. This dose of RU 486 effectively antagonizes glucocorticoid effects in primates and patients with Cushing's syndrome (1214). Before beginning treatment with RU 486 (or placebo) each subject had three serial blood samples and three 24-h urine samples collected during a 5-day period for baseline hormone measurements (plasma ACTH, cortisol, cortisol-binding globulin (CBG), aldosterone, urinary free cortisol, urinary aldosterone, and 17-hydroxysteroids), determination of hematologic, renal, and kidney function, as well as measurement of erythrocyte sedimentation rate, C-reactive protein, antinuclear antibody, rheumatoid factor, and quantitative immunoglobulins. During the RU 486 and placebo treatment periods as well as the 14-day washout period, blood and 24-h urine samples were collected every other day for the same measurements. By chance, the first three patients all received RU 486 first and all developed serious adverse effects after 9-10 days of therapy. RU 486 had to be discontinued, and the subjects prematurely entered into the 14-day washout period of the study. They did not subsequently enter the 14-day placebo period. Subject 4 completed the entire 6-week study without complication. Because of the high incidence of adverse effects the study was revised, such that only the subjects were blinded, and the next five subjects were treated initially with RU 486. Four of these subjects developed side-effects from RU 486 after 9-10 days of treatment that necessitated discontinuation of the drug and premature entry into the 14-day washout period. One additional subject completed the 6-week study without adverse effects. In an attempt to prevent further adverse effects, the last two subjects received only 7 days of RU 486 treatment before entering the 14-day washout period. Peripheral blood mononuclear cells for phenotypic studies of cell subsets plus functional evaluation of cytotoxicity and pro-
1475
liferation were obtained by leukopheresis in each subject. A leukopheresis was performed on both day 0 (pretreatment) and after 7 days of RU 486 treatment in all 11 subjects. The 2 subjects who uneventfully completed the full 6-week study had 2 additional leukophereses, 1 following the 14-day washout period and 1 following the 14-day placebo period. Hormone assays Blood samples were collected for measurement of ACTH (15), cortisol (16), and aldosterone (17) concentrations by previously described RIAs. The plasma concentration of CBG was measured by a competitive binding assay (18). The sensitivity of the assay for ACTH ranged from 0.7-1.1 pmol/L, for cortisol from 5.5-19.3 nmol/L, and for aldosterone from 56-111 pmol/ L. All samples from an individual patient were analyzed in the same assay. The intra- and interassay coefficients of variation were, respectively, 9% and 20% for ACTH, 5% and 11% for cortisol, and 7% and 13% for aldosterone. Urinary free cortisol excretion was measured by Smith-Kline Bioscience Laboratories (Philadelphia, PA) (19), and urinary aldosterone excretion by Hazelton Laboratories (Vienna, VA) (20). Urinary 17-hydroxysteroids were measured by ion exchange chromatography, followed by Porter-Silber analysis (21). Immunological assays Peripheral blood samples were collected for complete blood and differential counts, erythrocyte sedimentation rates, Creactive protein, antinuclear antibodies, rheumatoid factor, and quantitative immunoglobulins (IgG, IgA, and IgM). Peripheral blood mononuclear cells (PBMC) were prepared by leukopheresis and separated on density gradients (LSM, Litton Bionetics, Kensington, MD). PBMC were cryopreserved in 90% human AB serum and 10% dimethylsulfoxide to allow functional assays to be performed in parallel. Leukocyte culture was performed in complete medium consisting of RPMI-1640 (Biofluids, Rockville, MD) and 10% human AB serum (KC Biological, Kansas City, MO) with gentamicin added at 50 mg/L (Gibco, Grand Island, NY), 100 U/mL penicillin, 100 Mg/mL streptomycin, and 2 mM glutamine (NIH, Media Unit).
TABLE 1. Clinical profile and responses of normal male volunteers to RU 486 treatment (10 mg/kg-day) Subject no.
Age (yr)
Duration of treatment (days)
Adverse effects
1 2 3 4 5 6 7 8° 9
19 20 20 24 35 22 19 21 19
9 10 10 14 10 9 9 14 10
Generalized exanthem Generalized exanthem Generalized exanthem None Generalized exanthem Generalized exanthem Generalized exanthem None Signs c/w adrenal cri-
Appearance of adverse effects (days)
21 19
7 7
Generalized exanthem Generalized exanthem
Resolution of adverse effects (days)
9 10 9
D/C RU 486 D/C RU 486 D/C RU 486
5 6 5
10 9 9
D/C RU 486 D/C RU 486 D/C RU 486
5 5 6
10
D/C RU 486 + dexamethasone D/C RU 486 D/C RU 486
2
sis 10 11
Treatment for adverse effects
9 9
Patient 8 received ranitidine concurrently with RU 486.
The Endocrine Society. Downloaded from press.endocrine.org by [${individualUser.displayName}] on 16 January 2017. at 08:52 For personal use only. No other uses without permission. . All rights reserved.
5 5
LAUE ET AL.
1476
JCE&MM990 Vol 71 • No 6
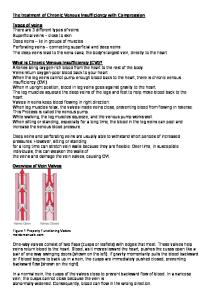
FIG. 1. Histological analysis of typical skin biopsies from two patients who developed a generalized exanthem while taking RU 486. Diffuse dermal, epidermal, and perivascular lymphohistocytic infiltrates are observed. A, Patient 1; 1:250 magnification. B, Patient 1, 1:500 magnification. C, Patient 2, 1:62 magnification. D, Patient 2, 1:250 magnification.
Fluorescent antibody staining and flow cytometric analysis Lymphocytes (106; 100 ^L) were aliquoted into polypropylene tubes (12 x 75 mm; Falcon, Oxnard, CA) and simultaneously directly stained with fluorescein isothiocyanate- or phycoerythrin-labeled monoclonal antibodies. The pan T-cell markers used in this study included CD3 (Leu4) and CD2 (Til). The Tcell subset markers used were CD4 (Leu3) and CD8 (Leu2) as well as double staining with CD3/HLA-DR. The B-cells were evaluated using antibodies to CD20 (Bl) and CD19 (B4). Natural killer (NK) cells were evaluated for the antigens CD16 (anti-IgG Fc receptor, Leu11) and HNK-1 (Leu7). The Leu reagents and anti-HLA-DR were obtained from Becton-Dickinson (Mountain View, CA); the reagents T i l , Bl, and B4 were obtained from Coulter Immunology (Hialeah, FL). Cells were incubated with the appropriate amounts of monoclonal antibody for 30 min at 4 C in phosphate-buffered saline containing 5% goat serum and 0.1% sodium azide. Isotype
reagent controls were prepared similarly. Cells were washed, fixed in 1.0% paraformaldehyde for 10 min, and resuspended in phosphate-buffered saline containing 0.1% sodium azide. Analysis was performed on a FACS Analyzer (Becton-Dickinson) equipped with a Consort 30, as previously described (22). Cytotoxicity testing Cytotoxicity was evaluated after rapid thrawing and culture of PBMC at 106/mL for 3 days in complete medium containing 1000 U/mL recombinant interleukin-2 (Cetus Corp., Emeryville, CA). A 4-h 51Cr release assay was used to measure cytotoxicity against a fresh human melanoma (TU587) and the NK-resistant Daudi leukemia cell line, as previously described (23). Cryopreserved human tumors with viabilities greater than 75% were labeled for 1 h. Cells were washed and tested at three to five effector to target ratios in triplicate at 5 x 103 targets/ well. After 4 h of incubation, the plates were harvested, and
The Endocrine Society. Downloaded from press.endocrine.org by [${individualUser.displayName}] on 16 January 2017. at 08:52 For personal use only. No other uses without permission. . All rights reserved.
>
A. *p