Use of Misoprostol Prior to Hysteroscopy in Postmenopausal Women: A Randomized, Placebo-Controlled Clinical Trial Aurélio Ribeiro da Costa, PhD, Aarão Mendes Pinto-Neto, PhD, Melania Amorim, PhD*, Lúcia Helena Simões Costa Paiva, PhD, Adriana Scavuzzi, MD, and Juliana Schettini, MD From the Department of Obstetrics and Gynecology, Institute for Maternal/Infant Health, Perbambuco (Drs. Costa, Amorim, Schettini, and Scavuzzi); Universidade Federal de Campina Grande Medical School, Paraiba (Dr. Amorim); Universidade Estadual de Campinas, UNICAMP, São Paulo (Drs. Pinto-Neto and Costa Paiva), Perbambuco.
ABSTRACT Study Objective: To compare results of diagnostic hysteroscopy in postmenopausal women using misoprostol for cervical ripening. Design: A randomized, placebo-controlled clinical trial (Canadian Task Force classification Ib). Setting: Hospital Barão de Lucena, Instituto Materno Infantil de Pernambuco. Patients: One hundred-twenty postmenopausal women. Intervention: Postmenopausal women received 200 g of vaginal misoprostol or placebo before hysteroscopy. Measurements and Main Results: Variables measured were procedure time, frequency of hysteroscopy carried out in each group (misoprostol and placebo), degree of pain during procedure, need for dilation, side effects, and complications of hysteroscopy. The 2, Fisher’s exact, and Mann-Whitney tests were used and considered significant when alpha error was ⬍5%. There were similarities between the groups in age (p ⫽ .09), body mass index (p ⫽ .55), time since menopause (p ⫽ .52), and genital bleeding (p ⫽ .52). Pain during the procedure, as measured by visual analog scale, was less severe in the misoprostol group than in the placebo group (median of 05 vs 07, p ⫽ .02), but there were similarities in duration (2.4 min vs 2.0 min, p ⫽ .3), pain during procedure and biopsy (p ⫽ .74 vs p ⫽ .19), need for dilation (p ⫽ .66), side effects, and complications. There were no differences in severity of post-procedure pain. Conclusions: Previous use of misoprostol reduced pain severity during hysteroscopy. Journal of Minimally Invasive Gynecology (2008) 15, 67–73 © 2008 AAGL. All rights reserved. Keywords:
Hysteroscopy; Menopause; Misoprostol; Clinical trial
Misoprostol is a synthetic methyl analogous of PGE1. Its advantages are thermostability, a lower risk of side effects, and reduced costs compared with natural prostaglandins [1–3]. It acts on the extracellular matrix of the cervix dissolving collagen and increasing hyaluronic acid and cervical water by increasing vascular permeability, thus facilitating the passage of neutrophils to tissue stroma. Interleukin-8 produced in the cervix attracts and activates neutrophils, which are an important source of collagenase, facilitating The authors have no commercial, proprietary, or financial interest in the products or companies described in this article. Corresponding author: Melania M. R. Amorim, PhD, Universidade Federal de Campina Grande, R. Neusa Borburema de Souza, Santo Antônio, Campina Grande, Paraíba, Brazil. E-mail:
[email protected] Submitted April 12, 2007. Accepted for publication August 6, 2007. Available at www.sciencedirect.com and www.jmig.org 1553-4650/$ -see front matter © 2008 AAGL. All rights reserved. doi:10.1016/j.jmig.2007.08.596
cervical softening [4]. Its affinity for cellular membrane receptors, bound to protein G, triggers cellular changes as a result of the stimulation of phospholipase C and adenylate cyclase enzymes, thus activating smooth muscle contraction, particularly in the uterus [2,5]. Studies demonstrate the use of misoprostol in many formulations: tablets or gel, in doses of 400, 200, or 100 g, given by mouth or by sublingual, rectal, or vaginal route [6]. The absorption of misoprostol occurs rapidly after oral administration, reaching peak plasma concentrations in 30 to 60 minutes, soon converting into its free acid form. Misoprostol acid is 85% bound to serum proteins. After a 200-g dose, 90% of the drug is excreted within 8 hours, 64% by the kidneys and 15% in the feces. The bioavailability of vaginally administered misoprostol is 3 times higher than that by mouth. After vaginal administration, plasma concentration increases, achieving peaks in 60 minutes.
68
Journal of Minimally Invasive Gynecology, Vol 15, No 1, January/February 2008
Concentration then slowly declines, reaching 60% of the maximum level 240 minutes after administration. These levels remain stable for 4 hours [7,8]. The main side effects of misoprostol are pain, diarrhea, vomiting, and genital bleeding [9]. Misoprostol has been shown to be effective before hysteroscopy, facilitating cervical dilation and reducing its complications [10]. Moreover, gynecologic assessment of the uterine cavity may be fraught with difficulties in postmenopausal women who represent a significant part of the female population [11–13]. To facilitate the insertion of the hysteroscope into the uterine cavity, a number of mechanisms have been used (e.g., laminaria, dilators, and natural prostaglandins). The natural prostaglandin is aimed at reducing risks related to the procedure, including anesthetic risk in patients with comorbidities. In this context, misoprostol has aroused interest among researchers, mainly in examining postmenopausal women [14 –18]. There are few well-controlled trials with adequate evidence and degree of recommendation, particularly in postmenopausal women. Thus the aim of this study was to compare results of previous use of vaginal misoprostol in postmenopausal women who underwent hysteroscopy without analgesia.
Population and Method A study was conducted of postmenopausal women attending either the Instituto Materno Infantil de Pernambuco or the Hospital Barão de Lucena from February through September 2005. A double-blind, placebo-controlled randomized clinical trial was designed to compare postmenopausal groups undergoing diagnostic hysteroscopy without anesthesia and with prior use of 200 g of misoprostol or placebo, both administered vaginally, for cervical ripening. Sample size was calculated by estimating need of cervical dilatation for hysteroscopy after previous use of medication (misoprostol or placebo), using the module STATCALC of statistical software Epi-Info 3.3.2 (U.S. Centers for Disease Control and Prevention [CDC], Atlanta, GA) [19]. Inclusion criteria were an indication for endometrial assessment due to polyps, myomas, endometrial thickening on ultrasound, or genital bleeding, and all patients signed a consent form to participate in the study. Exclusion criteria were genital infection or prior hysteroscopy procedure. Considering data of a previous study where authors analyzed need of cervical dilatation, about 7% of patients who underwent hysteroscopy after using misoprostol required additional dilatation compared with 31% of patients using placebo. To evidence this difference with a power of 80% and a 5% level of significance, a need for 120 women was calculated. Sixty women were randomly assigned to the misoprostol group and 60 to the placebo group.
Randomization was carried out with a computer-generated table of random numbers in Epitable, part of Epi-Info 6.04d. Allocation to both study groups took place only after patients signed their consent forms. Boxes sequentially numbered from 1 to 120 were prepared, and each number corresponded to a tablet of 200 g misoprostol or placebo (labeled drug A or B), according to the table of random numbers. The 200 g misoprostol tablets were prepared by Hebron, the pharmaceutical company that also manufactured placebo tablets especially for the research, with shape, size, color, and weight similar to the active drug. The tablets were stored in cardboard boxes, and the contents were known only to the pharmacist in charge. After inclusion in the study, the allocated numbered box was opened for each patient, and the principal investigator inserted the tablet into the vaginal cul-de-sac. Patients were told to return to the clinic 8 hours later. All procedures were carried out by the principal investigator in a surgical environment. No anesthesia was given. In all hysteroscopies, a rigid, standard, 4 mm hysteroscope with 30-degree lens was used (Karl Storz GmbH, Tuttlingen, Germany). The technique was performed as described by Tantini [20]. Procedure duration was measured with a Casio chronometer (Casio, Inc., Tokyo, Japan), from the insertion of hysteroscope through the external cervical opening to its withdrawal passing through the same route after the procedure. The presence and intensity of pain during and after the procedure (at 15, 30, 45, and 60 minutes) were assessed. Since pain is a naturally subjective experience, it is difficult to measure. Therefore, the use of standardized tools is important to overcome this problem, making it possible to compare different therapeutic techniques. In this study, a visual analog scale (VAS) was used to record pain stages, ranging from no pain to the worst imaginable pain. A correlated numeric scale was printed in the back of the scale [21]. Before the procedure took place, the VAS was presented to the participants, explaining its objectives and procedures to assess pain. Points for assessment were passage of the hysteroscope through the inner cervical os, cervical clamping, and at the time of biopsy. The need for additional cervical dilation and the presence of side effects such as genital bleeding, nausea, vomiting, diarrhea, and hyperthermia were recorded. Complications such as uterine perforation, false passages, cervical lacerations, and infections were assessed according to the CDC criteria [22]. Patients were contacted by telephone 8 days after the procedure to evaluate for possible complications. Statistical analysis was performed with Epi-Info 3.2.2. Bivariate analysis was initially carried out to test randomization, and patient characteristics in both groups (control variables) were compared. The 2 and Fisher’s exact tests were used to test the association between categorical variables. Measures of central tendency were used according to variable characteristics. Mann-Whitney tests were used to evaluate eventual differences between ordinal
Costa et al.
Misoprostol Before Hysteroscopy in Postmenopausal Women
variables (VAS). Some numerical variables were categorized for analysis, according to their distribution, and different cutoff points were attempted during analysis, such as the variable of procedure duration. In all stages of analysis, an alpha error of less than 5% was considered significant. The current study is in accordance with the Helsinki Declaration (amended in Hong Kong, 1989) and resolution number 196/96 of the National Health Council of Brazil and was previously approved by the ethics committees of the participating hospitals.
Results Out of 120 randomized women, 112 underwent hysteroscopy. Eight women (4 in the treatment group and 4 in the control group) had no procedure; 1 could not tolerate pain during passage of the hysteroscope through the inner cervical os (control group), 5 had severe stenosis (3 in the treatment group and 2 in the control group), 1 had prolapsed myoma (treatment group), and 1 had genital bleeding during procedure (treatment group). These were, however, included in the final analysis, with intention to treat (Fig. 1). There were no differences between the groups regarding proportion of cases undergoing procedure: 91% in the treatment group
69
and 95% in the placebo group (p ⫽ .35). Members of the groups were similar in age, parity, number of pregnancies, body mass index, schooling, time since medication, distension medium, previous cesarean sections or vaginal surgeries, frequency of hypertension, polyposis, or uterine myomatosis (Table 1). The frequency of complications was similar in both the treatment and placebo groups: 1 patient developed infection (endometritis), 5 had cervical tears, 3 had false passages, and 1 had uterine perforation after procedure (Table 2). The severity of pain (VAS) during the procedure was significantly lower in patients using misoprostol when compared with placebo (median of 05 vs 07, p ⫽ .02). However, no differences were observed when pain severity was assessed at the time of cervical clamping or biopsy (Fig. 2). The mean duration of the procedure was similar in the misoprostol and placebo groups (2.4 min vs 2.0 min, p ⫽ .3). The presence of pain during cervical clamping, passage of hysteroscope for procedure, and time of biopsy were also similar (p ⫽ .74; p ⫽ .32; p ⫽ .19, respectively) (Fig. 3). Moreover, no significant differences were observed between the groups regarding postoperative pain at 15 (p ⫽ .74), 30 (p ⫽ .59), 45 (p ⫽ .47), and 60 minutes (p ⫽ .29) (Fig. 4).
tt Eligible (1040) HBL=460 IMIP=580
RECORD
Excluded: Did not meet inclusion criteria HBL=184 IMIP=175 T=359 Absences: HBL=231 IMIP= 330 T=561 Refusal= 0
Randomised (120) HBL=45 IMIP=75 Did not undergo (08) HBL=04 IMIP=04
ALLOCATION
ANALYSIS
MISOPROSTOL HBL=22 IMIP=38 TOTAL=60
Intervention discontinued HBL=02 IMIP=03 TOTAL=05 Lost to follow up=0
PLACEBO HBL=23 IMIP=37 TOTAL=60
Intervention discontinued HBL=02 IMIP=01 TOTAL=03 Lost to follow up=0
Fig. 1. Flowchart of the allocation, randomized and analysis of the patients. HBL ⫽ Hospital Barão de Lucena; IMIP ⫽ Instituto Materno Infantil de Pernambuco.
70
Journal of Minimally Invasive Gynecology, Vol 15, No 1, January/February 2008
Table 1
Characteristics of patients undergoing diagnostic hysteroscopy with previous use of misoprostol or placebo Characteristic Age in yrs (mean, SD) Parity (median, range) Gestations (median, range) Time since menopause in yrs (mean, SD) BMI (mean, SD) Schooling in yrs (mean, SD) Site (n, %) HBL IMIP Time in hrs since medication (mean, SD) Distension medium CO2 (n, %) Cesarean sections (n, %) Vaginal surgeries (n, %) Hypertension (n, %) Uterine polyposis (n, %) Uterine myoma (n, %) Endometrial thickening (n, %) Genital bleeding (n, %)
Misoprostol n ⫽ 60
Placebo n ⫽ 60
p
95% CI
61.3 04 04 12.5 27 4.3
(8.2) (0–18) (0–20) (8.9) (4.8) (2.8)
59.2 04 05 9.6 27.5 4.0
(9.2) (0–13) (0–15) (9.7) (4.9) (2.9)
.19 .88 .83 .52 .55 .54
0.51–1.04 0.92–2.07 0.81–1.77 0.46–0.92 0.77–1.67 0.71–1.49
22 38 8.4 23 23 20 34 17 10 36 09
(48.9) (50.7) (1.0) (39.0) (56.1) (56.1) (45.9) (48.6) (55.6) (57.1) (39.1)
23 37 8.2 19 18 26 40 18 08 27 14
(51.1) (49.3) (1.1) (32.2) (43.9) (56.5) (54.1) (51.4) (44.4) (42.9) (60.9)
.85
0.66–1.40
.40 .44 .33 .25 .25 .99 .52 .37 .62
0.64–1.34 0.80–1.66 0.58–1.19 0.84–1.83 0.86–1.75 0.66–1.51 0.53–1.35 0.42–1.04 0.63–1.31
BMI ⫽ body mass index; HBL ⫽ Hospital Barão de Lucena; IMIP ⫽ Instituto Materno Infantil de Pernambuco.
When the severity of postoperative pain was evaluated with the VAS, no differences were noticed between the groups at 15 and 30 minutes, as well as at 45 and 60 minutes (median of 2 at 15 minutes and zero at 30 minutes, p ⫽ .66; p ⫽ 0.71; p ⫽ .73; and p ⫽ .30, respectively) (Table 3). The need for cervical dilation was similar between the groups (17.2 vs 20.3; p ⫽ .66). There were also no differences in the frequency of side effects and complications. Genital bleeding and nausea were the only side effects reported (44.8% and 12.3%, respectively, vs 40.4% and 10.5%, respectively; p ⫽ .62 and p ⫽ .70).
misoprostol in anticipation of hysteroscopy reduced pain severity during the procedure in postmenopausal women. Other studies with similar design support several results of our study, even in situations where the cervix offers some resistance, such as in postmenopausal women or in women with a history of previous cervical procedures [9,10,21–23]. Other authors have demonstrated advantages in using misoprostol before hysteroscopy, since it reduces the presence and severity of perceived pain, duration of the procedure, need for dilation, and number of complications [9,13,15,16].
Discussion Misoprostol is a methyl analogous of natural prostaglandins that pharmacologically facilitates cervical ripening [1,2]. The results of this study showed that the use of
Table 2
Frequency distribution of complications in patients undergoing diagnostic hysteroscopy with previous use of misoprostol or placebo Misoprostol
Placebo
Complication
n
%
n
%
2
p*
Uterine perforation Cervical laceration False passage Post-hysteroscopy infection†
1 5 3 1
1.7 8.4 5.0 1.7
2 4 4 0
3.3 6.6 6.6 0.0
0.32 0.14 0.13 1.0
.56 .48 .5 .5
*
Fisher’s exact test. † Endometritis.
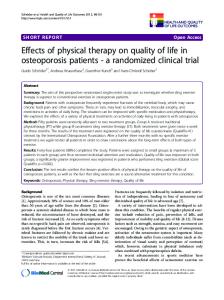
Fig. 2. Comparison of visual analog scale (VAS) scores at cervical clamping, during hysteroscopy, and at time of biopsy in patients with previous use of misoprostol or placebo.
Costa et al.
Misoprostol Before Hysteroscopy in Postmenopausal Women
number of patients
misoprostol placebo
100 90 80 70 60 50 p = .74 40 30 20 10 0 Clamping of the uterine cervix
Table 3
Comparison of visual analog scale (VAS) scores in patients with previous use of misoprostol or placebo
VAS scores
Misoprostol
Placebo
n
n
%
%
2
p
0.36
.36*
0.18
.66
0.30
.50*
0.13
.71
15 Scores 6-10 Scores 0-5 Median
p = .19
p = .32
04 51 02
7.3 92.7
01 54 00
1.8 98.2
06 51 02
10.5 89.5
02 55 00
3.5 96.5
30 Scores 6-10 Scores 0-5 Median 45
Pain during examination
Endometrial biopsy
Fig. 3. Comparison of pain presence at cervical clamping, during hysteroscopy, and at time of biopsy in patients with previous use of misoprostol or placebo.
Postmenopausal women were recruited for this study. The difficulty in inserting the hysteroscope through the cervical canal, as a consequence of genital atrophy, is the leading cause of discomfort during the procedure. Regardless of the method used, stenosis provoked by hypoestrogenism is associated with pain and failure to perform the procedure [23]. Perez-Medina et al [24] reported the main causes of procedure failure with 2 uterine cavity distension media (CO2 and saline). Six thousand patients were assessed including pre and postmenopausal patients and
misoprostol placebo 90 80 70 Number of patients
71
60 50 40 30 20 10 0
15 min
30 min
45 min
60 min
p = .74
p = .59
p = .47
p = .29
Fig. 4. Frequency distribution of postoperative pain presence in patients with previous use of misoprostol or placebo (diagnostic hysteroscopy).
Scores 6-10 Scores 0-5 Median
00 55 00
00 100
00 55 00
00 100
00 57 00
00 100
00 57 00
00 100
— 0.11
— .73
60 Scores 6-10 Scores 0-5 Median *
— 1.04
— .30
Fisher’s exact test.
women with no history of pregnancy or delivery, despite the homogeneous distribution among the groups. It was found that cervical stenosis due to genital atrophy was the chief cause of failure. Although the groups showed low failure rates (7.6% and 1.7%, respectively), genital atrophy represented one of the main reasons for failure in hysteroscopy, and it was the most common situation among patients who needed local anesthesia. Although studies with similar methods have shown advantages in using misoprostol before hysteroscopy, we found no significant differences in the need for additional dilation, presence of pain during and after the procedure, and complications, as was observed in a trial carried out in Thailand between October 1997 [16] and September 1998 [16]. In the Thai study, 91 women used 200 g of misoprostol or placebo in the posterior cul-de-sac approximately 8 hours before hysteroscopy, and a shorter cervical length was observed in the treated group as compared with the placebo group (3.8 mm vs 7.8 mm, p ⬍.001). It was also found that only 3 patients in the misoprostol group (6.5%) needed additional dilation, compared with 31% in the control group (p ⫽ .05). Moreover, the mean procedure duration in patients from the placebo group was almost twice as long as in the misoprostol group (p ⬍.01) [16]. Most of the previous studies adopted an interval from 8 to 12 hours between use of medication and the procedure, but these studies are based on surgical hysteroscopy with an inpatient regimen. In our study, we analyzed cases of diagnostic hysteroscopy and tried to use the lowest time evaluated in the literature. Therefore, our results can conclude that this interval can be reduced. Using 8 hours between drug administration and hysteroscopy was based on pharmacology. According to experimental studies with monkeys and dogs, the half-life of misoprostol is about 4 hours, and
72
Journal of Minimally Invasive Gynecology, Vol 15, No 1, January/February 2008
human studies show half-life of 4 to 6 hours but a slow elimination that can achieve 72 hours. Other studies demonstrated that with 200 g of misoprostol, 90% of plasma levels are obtained with 8 hours. In addition, higher doses seem to increase genital bleeding and side effects [25]. Nonetheless, the difference between the groups according to duration of the procedure cannot be investigated because we worked with diagnostic hysteroscopy, an outpatient rapid procedure that doesn’t require greater cervical dilatation as occurs in surgical procedures [26]. The incidence of complications in our study was 16.6%, which is above the expected number according to the literature. It was noted that only 1.8% of the patients in the treated group had uterine perforation versus 3.8% of controls (p ⫽ .56), regarding infectious complication, there was only 1 case of endometritis in the misoprostol group. Separately, these findings are in agreement with the literature (1%). This situation suggests that the high frequency of cervical lacerations and false passages might be associated with genital atrophy [17]. Furthermore, members of the population under investigation had particular characteristics, in that they were postmenopausal women whose numbers of estrogen receptors are reduced. One possible explanation for not finding similar results as in the literature might be the parameters used for sample size calculation. Our sample size calculation was based only on the need for dilation [18]. Taking this into consideration, our results were compatible with some double-blind, randomized trials, especially a study carried out at the Queen Mary Hospital in Hong Kong, China, that evaluated 37 postmenopausal women, randomized into 2 groups to receive 400 g of misoprostol orally or vitamin B6. The medication was offered 12 hours before the procedure. The need for additional cervical dilation, as well as procedure duration and complications were assessed, but comparable results between the groups, despite a trend toward improvement, were in favor of the misoprostol group [21]. Perhaps postmenopausal women need different doses or intervals because of their reduced number of prostaglandin receptors and time for adequate drug action, according to ideal plasma concentrations (approximately 6 hours). Another trial carried out at the Mt. Sinai Hospital, Toronto, Canada and at the Women’s College Hospital, Toronto, Ontario, Canada, also evaluated women with similar characteristics as in this study, dividing them into 2 groups of 94 and using 400 g of misoprostol orally or placebo. They observed a greater ease of cervical dilation in the misoprostol group (p ⫽ .08; OR ⫽ 2.6; 95% CI 1.28 –5.29), as measured by the Likert scale [27]. Although other results from our study do not coincide with those of the medical literature, it is worth pointing out that for unequivocal guidance of clinical decision making and establishment of new practices, the best study design for determining intervention or treatment efficacy is the controlled clinical trial, which was used in this investigation [28,29]. The main limitation of the study was the sample
size calculation based on the need for cervical dilation. In view of this, the number of cases may not have been enough to show differences in relation to other parameters assessed, which characterizes a type II statistical error.
Conclusion The results indicate that previous use of misoprostol by the vaginal route for diagnostic hysteroscopy without anesthesia reduced pain severity during the procedure. Considering the particularities of postmenopausal women, we believe it is important to carry out more controlled trials to establish the true advantages of misoprostol and then determine whether or not to adopt this new practice. We must bear in mind that evaluating one’s own results is part of the 5 recommended steps for the practice of evidence-based medicine [26,29].
References 1. Song J. Use of misoprostol in obstetrics and gynecology. Obstet Gynecol Surv. 2000;55:503–510. 2. Hofmeyr GJ, Gulmezoglu AM. Vaginal misoprostol for cervical ripening and induction of labor (Cochrane Review). In: The Cochrane Library. Oxford: Update Software: 2002;2. 3. Muzonzini G, Hofmeyr GJ. Buccal or sublingual misoprostol for cervical ripening and induction of labour (Cochrane Review). In: The Cochrane Library. Oxford: Update Software: 2006;1. 4. Blanchard K, Clark S, Winikoff B, Gaines G, Kabani G, Shannon C. Misoprostol for women’s health: a review. Obstet Gynecol. 2002;99: 316 –332. 5. Arias F. Pharmacology of oxytocin and prostaglandins. Clin Obstet Gynecol. 2000;43:455– 468. 6. Bisharah M. A randomized trial of sublingual misoprostol for cervical priming before hysteroscopy. J Am Gynecol Laparosc. 2003;10:390 – 391. 7. Schoenhard G, Oppermann J, Kohn FE. Metabolism and pharmacokinetic studies of misoprostol. Dig Dis Sci. 1985;30:126 –128. 8. Zieman M, Fong SK, Benowitz NL, Banskter D, Darney PD. Absorption kinetics of misoprostol with oral or vaginal administration. Obstet Gynecol. 1997;90:88 –92. 9. Moraes Filho OB, Albuquerque RM, Pacheco AJ, et al. Misoprostol sublingual versus vaginal para indução do parto a termo. Revista Brasileira de Ginecologia e Obstetricia. 2005;27:24 –31. 10. Preutthipan S, Herabutya Y. A randomized controlled trial of vaginal misoprostol for cervical priming before hysteroscopy. Obstet Gynecol. 1999;94:427– 430. 11. Machado MKN, Pina H, Matos E. Acurácia da histeroscopia na avaliação da cavidade uterina em pacientes com sangramento uterino pós-menopausa. Revista Brasileira de Ginecologia e Obstetricia. 2003;25:237–241. 12. Scavuzzi A, Amorim M, Pinho Neto JS, Santos LS, Comparação entre os achados ultra-sonográficos, histeroscópicos e histopatológicos no sangramento uterino da pós-menopausa. Revista Brasileira de Ginecologia e Obstetricia. 2003;25:229 –235. 13. Pinto-Neto AM, Costa Paiva LHS, Fonsech-Carvasan GH. In: Fernandes CE. Menopausa: Diagnóstico e Tratamento 1st ed. São Paulo: 2003:23–29. 14. Propst AM, Libermam RF, Harlow BL, Ginsburg ES. Complications of hysteroscopy surgery: predicting patients at risk. Obstet Gynecol. 2000;96:517–520.
Costa et al.
Misoprostol Before Hysteroscopy in Postmenopausal Women
15. Jansen FW, Vredevoogd CB, Von Ulzen K, Hermans J, Trimbos JB, Trimbos-Kemper TC. Complications of hysteroscopy: a prospective, multicenter study. Obstet Gynecol. 2000;96:266 –270. 16. Spirlet MB. Use of misoprostol in gynecology and obstetrics. Gynecol Obstet Fertil. 2002;30:317–324. 17. Barcaite A, Bartusevicius DR, Railaite R, Nadisauskiene R. Vaginal misoprostol for cervical priming before hysteroscopy in perimenopausal and postmenopausal women. Int J Gynaecol Obstet. 2005;91: 141–145. 18. George AV, Basim AR. New developments in ambulatory hysteroscopic surgery. Baillieres Best Pract Res Clin Obstet Gynaecol. 2005; 19:727–742. 19. Fleiss W. Statistical Methods for Rates and Proportions. Wiley, Atlanta; 1981:38 – 45. 20. Tantini C. Técnica do exame de histeroscopia In: Mencaglia L, Albuquerque Neto LC eds. Histeroscopia Diagnóstica. São Paulo: Medsi; 2002:119 –128. 21. Collins SL, Moore RA, McQuay HJ. The visual analogue pain intensity scale: what is moderate pain in millimeters? Rev Pain. 1997;95: 95–97. 22. Magram AJ, Horan TC, Pearson ML, Silver LC, Jarvis WR. Guideline for prevention of surgical site infection, 1999: Centers for Disease
73
23.
24.
25. 26. 27.
28.
29.
Control and Prevention (CDC) Hospital Infection Control Practices Advisory Committee. Am J Infect Control. 1999;27:97–132. Ngai SW, Chan YM, Ho PC. The use of misoprostol prior to hysteroscopy in postmenopausal woman. European Society of Human Reproduction and Embryology. 2001;16:1486 –1488. Perez-Medina T, Bajo MJ, Martinez-Cortes L, Castellanos P, Perez de Avila I. Six thousand office diagnostic-operative hysteroscopies. Obstet Gynecol. 2000;71:33–38. Karim A. Antiulcer prostaglandin misoprostol: single and multiple dose pharmacokinetic profile. Prostaglandins. 1987;33:40 –50. Schoenhard G, Oppermann J, Kohn FE. Metabolism and pharmacokinetic studies of misoprostol. Dig Dis Sci. 1985;30:126 –128. Thomas AJ, Leyland N, Durand N, Windrin RC. The use of misoprostol as a cervical ripening agent in operative hysteroscopy: a double-blind, placebo-controlled trial. Am J Obstet Gynecol. 2002; 186:876 – 879. Sackett DL, Straus SE, Richardson WS, Rosenberg W, Haynes RB. Evidence-Based Medicine. How to Practice and Teach EBM 2nd ed. Toronto: Churchill Livingstone; 2000. Moher D, Schultz KF, Altman DG. The consort statement: revised recommendations for improvising the quality of reports of parallelgroup randomised trials. Lancet. 2001;357:1191–1194.