Journal Li et al. of / Tai Applied Chi and Gerontology Multidimensional Self-Esteem
Tai Chi as a Means to Enhance Self-Esteem: A Randomized Controlled Trial Fuzhong Li Oregon Research Institute Peter Harmer Willamette University Nigel R. Chaumeton Terry E. Duncan Susan C. Duncan Oregon Research Institute
Using a randomized controlled trial, this study examined whether a 6-month Tai Chi exercise program enhanced elderly individuals’ multidimensional, hierarchical physical self-esteem. Participants either continued their daily routine activities or participated in a Tai Chi exercise class performing slow rhythmic movements. Both global and domain-specific physical esteem measures were assessed at baseline, at 3 months, and at the 6-month termination of the intervention. Growth curve models were used to analyze the repeated-measures data. Results indicated that individuals who participated in the 6-month Tai Chi exercise program showed increased levels of global self-esteem, domain-specific physical self-worth, and subdomain-specific esteem of attractive body, physical strength, and physical condition. Thus, Tai Chi, a simple, low-cost form of physical activity, has the potential to alter favorably specific facets of physical self-worth/ esteem in older adults, which may in turn enhance important aspects of their quality of life.
Much of what is known relative to the physical and psychological benefits of physical activity in older adults has been based on studies employing aerobic activity (walking, jogging, cycling, etc.) as the primary mode of activity (e.g., McAuley et al., 1999). However, alternative and complimentary modes of activity are being embraced as equally useful in the promotion of an active and healthful lifestyle in the elderly. Tai chi, a traditional dancelike exercise AUTHORS’ NOTE: Preparation of this article was supported in part by Grants AG18394 and AG17053 from the National Institute on Aging. The Journal of Applied Gerontology, Vol. 21 No. 1, March 2002 70-89 © 2002 The Southern Gerontological Society
70
Li et al. / Tai Chi and Multidimensional Self-Esteem
71
originating from Chinese culture, has been presented as one alternative. Recent empirical evidence has demonstrated that Tai Chi contributes to a host of physical health benefits, including a reduction in rates of multiple falls (Wolf et al., 1996), reduction in systolic blood pressure (Wolf et al., 1996; Young, Appel, Jee, & Miller, 1999), enhanced stability and strength of knee extension (Jacobson, Chen, Cashel, & Guerrero, 1997), improved postural control (Schaller, 1996; Tse & Bailey, 1992; Wolf et al., 1996), and maintenance of balance and strength gains achieved by a high-intensity, laboratorybased training program (Wolfson et al., 1996). Recent studies have provided initial evidence that Tai Chi may improve many aspects of psychological well-being (e.g., Chen & Sun, 1997; Li, Duncan, et al., 2001; Li, McAuley, et al., 2001). For example, Li, Duncan, et al. (2001) showed that older adults who participated in a 6-month controlled Tai Chi trial exhibited increased levels of health perceptions, life satisfaction, positive affect, and well-being and decreased levels of depression, negative affect, and psychological distress. Grounded on Bandura’s (1986) social cognitive theory, Li, McAuley, et al. (2001) also demonstrated that Tai Chi promoted self-efficacy, which was further shown to be related to exercise behavior in older adults. Thus, as a psychological control variable, self-efficacy appears to represent an important interface between the individual and his or her behavior. Overall, these studies collectively suggest that Tai Chi is capable of generating a sense of psychosocial well-being. The present study focused on the effect of Tai Chi on self-esteem. Selfesteem can be conceptualized as self-regard, an evaluation of one’s worthiness (Rosenberg, Schooler, Schoenbach, & Rosenberg, 1995), with at least two dimensions: perceptions of competence and self-acceptance (Sonstroem, 1997, 1998). Positive self-esteem is widely recognized as an important psychological outcome of exercise participation (McAuley, 1994; Sonstroem, 1984). Indeed, the conclusion of several major reviews of empirical research was that regular exercise improves self-esteem, which consequently contributes to improved quality of life (Folkins & Sime, 1981; Fox, 1997; Hughes, 1984; McAuley, 1994; Sonstroem, 1984, 1997). As such, the study of selfesteem represents an important area of research, particularly in the aging population, as it will (a) shed light on the nature of physical self-esteem/worth and its relationship with physical activity involvement, health, and lifestyles and (b) allow more serious consideration of the idea that self-perceptions play a mediating role in perceived psychological benefit of activity and, ultimately, the quality of life. Recent research on self-esteem has extended the traditional idea of a single global self-esteem paradigm through development of theoretical models and instrumentation that reflect self-esteem as a multidimensional, domain-
72
Journal of Applied Gerontology
specific, and hierarchical phenomenon (Byrne, 1996; Fox, 1997; Fox & Corbin, 1989; Marsh, 1997). In the area of physical activity research, the development of the Physical Self-Perception Profile (PSPP) (Fox & Corbin, 1989) represents a major advance in the study of self-esteem in the physical domain. Fox and Corbin developed this general physical self-worth scale subsuming four more specific scales of perceived sport competence, physical condition, attractive body, and physical strength. In line with this theoretical conceptualization, they proposed a three-tier model with the four subdomains of esteem (i.e., sport competence, physical condition, body attractiveness, physical strength) at the base of the model influencing physical self-worth, which in turn has an impact on global self-esteem at the apex (see Figure 1). In the context of exercise intervention, the hierarchical structure of this self-esteem model would suggest that changes at the subdomain levels resulting from exercise are related to changes in global self-esteem through the mediation of the domain-specific level of esteem (i.e., physical self-worth/ esteem). This multidimensional, hierarchical physical self-esteem model provides opportunities for developing discriminant validity and for hypothesis testing on the relationship between physical self-esteem and external variables (e.g., exercise behavior, emotional well-being). Given the importance attached to positive self-esteem in physical activity (McAuley, 1994), the role of Tai Chi in positively enhancing self-esteem seems particularly important to investigate. To date, only one study (Kutner, Barnhart, Wolf, McNeely, & Xu, 1997) has examined the relationship between self-esteem and Tai Chi. Although participants in the Tai Chi condition appeared to improve preintervention to postintervention on the global self-esteem measure (Rosenberg, 1965), the change was not statistically significant. The finding may not be surprising in view of the global-level measure of self-esteem used in the study and suggests the need for studies that incorporate domain- specific physical measures of self-esteem if one is interested in capturing physical activity effects. Therefore, this study was designed to examine changes in multidimensional physical self-esteem resulting from a 6-month Tai Chi intervention trial. In line with previous research, it was hypothesized that compared to a control group, individuals who were in the Tai Chi group would increase in self-esteem measures over the course of a 6-month study period. It was also anticipated that changes at the subdomain levels of physical esteem would be related to changes in global self-esteem through the mediation of the domainspecific level of esteem.
Li et al. / Tai Chi and Multidimensional Self-Esteem
Figure 1.
73
A theoretical model of self-esteem.
Method Participants Low-active older adults (N = 98, M age = 73.2 years, SD = 4.9) were recruited to participate in a 6-month randomized controlled exercise trial (see Li, McAuley et al., 2001). Inclusion criteria for participation in the program were (a) age 65 years or above; (b) low active, defined as noninvolvement in a regular exercise program (either structured or unstructured) in the month prior to participation in the study and verified by a brief instrument designed specifically to assess physical activity in older persons (see below); (c) healthy to the degree that participation in an exercise program would not exacerbate any existing symptomology (determined by participant self-report); and (d) willingness to be randomly assigned to treatment conditions. Although not required, participants were encouraged to consult with their personal physician before participating.
74
Journal of Applied Gerontology
Recruitment A total of 148 individuals responded to local newspaper advertisements and flyers at senior centers seeking volunteer participation in a longitudinal study. To screen for prior physical activity level, each respondent was interviewed by telephone using a short version of the Physical Activity Scale for the Elderly (PASE) (Washburn, Smith, Jette, & Janney, 1993), which measured the frequency of leisure activities (i.e., walking outside the home, strenuous sport and recreation) and household activities (i.e., housework, lawn work/yard care, home repair, outdoor gardening) over the previous month. The majority of individuals (88%) indicated that they were engaging in some level of household activity (e.g., dusting, vacuuming, washing dishes) but were not involved in any sport or recreational activities.
Intervention Assignments Individuals who met the study criteria, agreed to participate, and gave written informed consent (N = 98), were then randomized to either Tai Chi practice (intervention group: n = 53) or to a waiting list (control group: n = 45, M age = 72.73 years, SD = 5.69). The unbalanced groups were partially due to married couples who were assigned as individuals based on practical considerations (e.g., intention to stay in the same class, transportation). Of the seven couples in the participant pool, one agreed to the group randomization as individuals and the remaining six couples were assigned as couples to the groups based on randomly generated numbers (five to the Tai Chi group and one to the control group). Two couples assigned to the Tai Chi group dropped out of the study after the randomization but before receiving intervention. Time conflict with class was the reason for withdrawing. Therefore, the intervention group consisted of 49 participants (M age = 72.84 years, SD = 4.65) who actually began the intervention. Participants’ demographic characteristics and physical activity pattern at baseline are shown in Table 1.
Experimental Protocol Participants in the intervention group attended a 60-minute Tai Chi session twice a week for 6 months. The Tai Chi intervention was a classical Yang style (24 forms) that incorporates elements of balance, postural alignment, and concentration. The sessions consisted of a 15-minute warm-up and 30 minutes of Tai Chi practice, followed by a 15-minute cool-down period. During the practice, participants were required to replicate the motions, postures,
Li et al. / Tai Chi and Multidimensional Self-Esteem
75
Table 1. Participant Demographic Characteristics and Physical Activity Patterns at Baseline
Characteristic
Tai Chi (n = 49)
Age (years)
72.8 (4.7) 88 14.5 (2.9) 25,000 94
Gender (% female) Education (years) Income (average in dollars) Race (% White)
Seldom Sometime Often Physical activity pattern (in percentages) Sitting activities Take a walk and so forth Light sport or recreational activities Moderate sport or recreational activities Strenuous sport or recreational activities Exercises to increase muscular endurance
Control (n = 45) 72.7 (5.7) 92 15.0 (2.5) 22,500 82
Seldom Sometime
Often
2
10
88
17
14
69
94
3
3
93
5
2
96
4
0
97
3
0
97
3
0
98
2
0
99
1
0
99
1
0
99
1
0
98
2
0
Household activity pattern (in percentages) Light housework (e.g., dusting, washing dishes) Heavy housework or chores (e.g., vacuuming, scrubbing floors, washing windows) Home repairs (e.g., painting, wallpapering, electrical work) Lawn work or yard care (e.g., snow or leaf removal, wood chopping) Outdoor gardening Caring for another person (e.g., children, dependent spouse)
Yes
No
Yes
No
95
5
98
2
97
3
93
7
2
98
3
97
4 2
96 98
2 2
98 98
1
99
0
100
NOTE: Values in parentheses are standard deviations.
76
Journal of Applied Gerontology
and speed of movement of the instructor. Participants were also encouraged to practice at home. Participants in the control group were instructed to maintain their routine activities and not to begin any new exercise programs. They were promised a 4-week Tai Chi program at the end of the intervention study.
Measures Background information. A short inventory was administered at baseline to assess demographic characteristics such as age, gender, education, income, and race/ethnicity. Domain-specific self-esteem. The PSPP (Fox & Corbin, 1989) is a 30-item instrument used to assess self-esteem relative to several domains of physical functioning in a hierarchical, multidimensional fashion. The instrument contains a general physical self-worth scale and four subscales specific to perceived sport competence, physical condition, attractive body, and physical strength, with six items per scale. However, given the nature of the sample (low-active older adults), we elected to delete those items that comprised the sports competence dimension. Participants indicated on a 4-point scale the degree to which each item was characteristic or true of them. Responses range from 1 (not at all true) to 4 (completely true). Fox and Corbin provided internal consistency coefficients ranging from .81 to .92 and test-retest reliability coefficients ranging from .81 to .88 over a 23-day lapse period. They have also provided extensive factorial, construct, and predictive validity for the PSPP. Internal consistencies for each dimension in the present study were acceptable across time—Time 1 (T1), Time 2 (T2), and Time 3 (T3): .84 (T1), .81 (T2), and .82 (T3) for physical self-worth; .76 (T1), .89 (T2), and .77 (T3) for physical condition; .84 (T1), .76 (T2), and .82 (T3) for attractive body; and .83 (T1), .83 (T2), and .84 (T3) for physical strength. Global self-esteem. Global self-esteem was assessed via the Rosenberg (1965) self-esteem scale. This scale has been widely used in several areas of self-esteem research, including physical activity (Fox, 1997). The scale consists of 10 items asking participants to indicate their level of agreement/disagreement with each statement. The reliability for this measure across time in the study was .83 (T1), .85 (T2), and .89 (T3).
Li et al. / Tai Chi and Multidimensional Self-Esteem
77
Procedures All participants completed the measures described previously during an initial group orientation meeting (Week 1). Before beginning, study participants signed consent forms indicating the voluntary and anonymous nature of the study. Instructions were read aloud by the researcher, and sample questions were provided prior to the administration of the questionnaire. In addition, participants were encouraged to clarify any questions or confusions they might have with regard to the questionnaire. No problems were encountered in completing the questionnaire. Participants from the experimental group completed these measures a second (Week 12) and third (Week 24) time either at the end of a class or at home within 1 week. Participants in the control group completed their second and third assessments by mail.
Statistical Analyses The analytical approach involved use of growth curve analysis (randomeffects model) (Bryk & Raudenbush, 1992; Meredith & Tisak, 1990). The model allows estimates of individual slopes to indicate change over time on the outcome variables of interest and use of the slope scores to examine the effect of group assignment. This methodology was used in the current investigation to examine changes in specific facets of the self-esteem measures. The analytic procedure is considered more statistically efficient than repeatedmeasures ANOVA because it uses all available data for each participant rather than dropping cases where one or more data collection time points are missing, as is done in a repeated-measures ANOVA. In addition, because there was missing data, random effects pattern mixture model analyses were conducted to test for the effects of dropping out on estimates of change (Hedeker & Gibbons, 1997; Little & Yau, 1996). For these analyses, a simple contrast of completers (defined as those who completed the study) with dropouts (defined as those who provided less than 3 time points data) was made using this status as a grouping variable in the random effects pattern mixture model. Upon establishing change in scores in all esteem measures, slope scores for each individual were computed. Specifically, the slope for each participant in the Tai Chi group was calculated through within-person ordinary least squares (OLS) regression analysis. These slope scores were then used to calculate correlations among the esteem measures, which allowed an examination of relationships among changes in self-esteem levels.
78
Journal of Applied Gerontology
The study was designed to have adequate power to detect a moderate effect size (i.e., .5 SD) and assumed 20% attrition of randomized participants. Statistical significance was set at the .05 level. SAS PROC mixed procedure was used to estimate the model (SAS Institute, 1992).
Results Intervention Compliance Of the 94 participants who actually began the intervention, 72 completed all three assessments. Nine participants in the intervention group dropped out of the study due to reasons such as traveling, time conflict with class, and family-related commitments (18% attrition rate). Thirteen participants dropped out of the control group due to reluctance to have to wait to join the class at the end of the study (29% attrition rate). Thus, the overall attrition rate at the end of the 24-week study was 23%. Preliminary analysis indicated that there were no significant differences (p = .12) between dropout participants and adherers in the demographic characteristics presented in Table 1. The average attendance rate (two times per week, with a total of 48 possible sessions) in the Tai Chi group was approximately 90%, with a median compliance of 41 sessions and a range of 29 to 47 sessions.
Differences in Baseline Measures Preliminary analyses (t tests or chi-square tests) comparing participants in the Tai Chi group and the control group indicated that the two conditions did not differ significantly (ps ≥ .10) at baseline on any of the demographic measures involving age, gender, income, and education. In addition, there were no significant differences (ps ≥ .13) by group on any of the esteem measures at baseline. These results indicated no need for adjusting any demographic and/or baseline esteem measures in the subsequent main analyses.
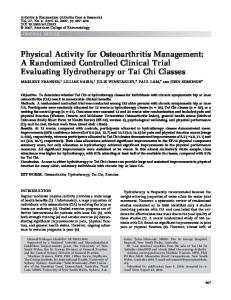
Treatment Outcomes: Effect of Tai Chi on Multidimensional Self-Esteem Over Time Table 2 shows the means and standard deviations of esteem measures at all three time points. Compared to the control group, the mean statistics in Table 2 indicated a general increase in all esteem measures over time for the Tai Chi
Li et al. / Tai Chi and Multidimensional Self-Esteem
79
Table 2. Descriptive Statistics for the Data: Means and Standardized Deviations for Esteem Measures at Baseline, Middle, and Postintervention.
Measure Global esteem Baseline Middle Postintervention Physical self-worth Baseline Middle Postintervention Attractive body Baseline Middle Postintervention Physical strength Baseline Middle Postintervention Physical condition Baseline Middle Postintervention
Tai Chi Group
Control Group
32.310 (4.061) 35.000 (3.823) 35.225 (3.939)
31.067 (4.807) 32.500 (4.554) 32.719 (4.510)
13.511 (4.034) 15.140 (3.796) 15.725 (3.610)
14.044 (3.030) 13.647 (3.209) 14.531 (3.100)
13.214 (3.949) 14.535 (4.061) 14.625 (3.807)
13.667 (3.580) 14.059 (3.601) 14.075 (3.617)
12.986 (3.669) 14.186 (3.881) 14.450 (3.993)
13.622 (3.466) 13.235 (3.970) 13.781 (2.837)
13.423 (3.620) 14.814 (3.850) 14.950 (3.748)
13.311 (3.866) 13.559 (4.009) 14.106 (3.550)
NOTE: The sample size for baseline = 49, middle = 43, and postintervention = 40 for the Tai Chi group; the sample size for baseline = 45, middle = 34, and postintervention = 32, for the control group, respectively.
group. To provide a visual inspection of mean level change in the two groups across time, plots of means over time are presented in Figure 2.
80
Journal of Applied Gerontology
Figure 2. Mean level change in global self-esteem and domain-specific physical self-esteem.
Table 3 presents a corresponding correlation matrix for the two conditions showing the relations among the various dimensions of self-esteem over time. The matrix for the Tai Chi group showed moderate-to-strong correlations among the physical aspects of self-esteem. Dropouts and attrition. In testing for potential effects of dropping out on estimates of mean change, the analysis with the random effects pattern mixture model revealed no evidence of differential change as a function of dropping out. That is, slopes did not differ across the two groups, defined by the variable status: 0 if the person was measured at T1 (completers) and 1 if the person was not measured at T3 (dropouts).
Table 3. Correlations Among Dimensions of Self-Esteem at Three Measurement Time Points
81
Tai Chi Group 1. Global esteem a. Baseline b. Middle c. Post 2. Physical selfworth a. Baseline b. Middle c. Post 3. Attractive body a. Baseline b. Middle c. Post 4. Physical strength a. Baseline b. Middle c. Post 5. Physical condition a. Baseline b. Middle c. Post
1a
1b
1c
2a
2b
2c
1.00 .64 .54
1.00 .71
1.00
.47 .34 .39
.44 .42 .32
.39 .31 .33
3a
3b
3c
.23 .29 .28
1.00 .68 .57
1.00 .64
1.00
.33 .22 .26
.17 .20 .24
.74 .53 .46
.59 .74 .58
.20 .08 .11
.30 .24 .14
.20 .18 .09
.75 .56 .48
.35 .31 .34
.38 .40 .36
.25 .25 .33
.76 .66 .53
4a
4b
4c
.47 .44 .71
1.00 .77 .77
1.00 .73
1.00
.63 .77 .60
.54 .48 .80
.54 .41 .31
.42 .50 .37
.33 .37 .54
1.00 .77 .69
1.00 .70
1.00
.67 .87 .67
.56 .57 .82
.62 .60 .50
.48 .71 .48
.47 .55 .70
.64 .55 .48
.55 .73 .57
.46 .55 .77
5a
5b
5c
1.00 .76 .69
1.00 .70
1.00
(continued)
82
Table 3. Continued
1a Control group 1. Global esteem a. Baseline 1.00 b. Middle .64 c. Post .67 2. Physical selfworth a. Baseline .16 b. Middle .08 c. Post .17 3. Attractive body a. Baseline .24 b. Middle .11 c. Post .03 4. Physical strength a. Baseline .07 b. Middle .10 c. Post .20 5. Physical condition a. Baseline .15 b. Middle .02 c. Post .05
1b
1c
2a
2b
2c
1.00 .83
1.00
–.02 .06 .28
3a
3b
3c
.18 .26 .34
1.00 .62 .66
1.00 .76
1.00
–.07 .11 .19
.08 .28 .30
.71 .64 .56
.52 .72 .60
.10 .11 .18
.22 .21 .17
.65 .43 .42
–.09 .13 .08
.06 .29 .16
.68 .64 .54
4a
4b
4c
.47 .65 .72
1.00 .76 .63
1.00 .83
1.00
.63 .69 .57
.67 .61 .71
.32 .25 .27
.46 .51 .50
.34 .38 .49
1.00 .78 .64
1.00 .72
1.00
.63 .80 .52
.56 .71 .66
.69 .60 .47
.60 .75 .51
.46 .68 .57
.55 .59 .41
.51 .60 .41
.50 .54 .68
5a
5b
5c
1.00 .76 .67
1.00 .69
1.00
Li et al. / Tai Chi and Multidimensional Self-Esteem
83
Growth curve analyses. Table 4 presents growth curve results of the randomized controlled trial. Adopting terminology from the conventional repeatedmeasures ANOVA, the estimates (i.e., the beta weights) shown in Table 4 are equivalent to Group × Time interaction effects in that they represent the degree to which esteem differences in the two treatment conditions vary across time. Results revealed statistically significant (p ≤ .01) improvement of Tai Chi group in all esteem measures, including global self-esteem, showing that the intervention group increased levels of esteem over time in relation to the control group. This set of results indicated that participants receiving Tai Chi had better outcomes than those on the waiting list on all self-esteem measures. Relationships among changes in self-esteem levels: Tai Chi group analyses. Having examined changes in esteem measures resulting from the Tai Chi intervention, we examined whether change in one specific measure of self-esteem was related to change in other types of esteem. Slope scores generated from OLS analyses were used for this purpose. The resulting correlation matrix is presented in Table 5. The matrix shown in Table 5 indicated that subdomain slope scores were positively related to changes at the domain level (ps < .001) and slope scores between global self-esteem and physical self-worth were statistically significant (r = .31, p < .05), implying that physical self-worth mediated relations between global self-esteem and subdomain levels of physical condition, attractive body, and strength condition. These findings are in concert with the multidimensional hierarchical conceptualization of the self-esteem model described earlier.
Discussion This study was designed to examine changes in multidimensional, hierarchical physical self-esteem resulting from a 6-month randomized controlled trial of Tai Chi. The findings serve to increase our understanding of both the patterns of self-esteem change resulting from Tai Chi and the underlying structure of physical self-esteem. The results from the present study indicate that compared to the no-treatment control group, the Tai Chi group yielded significant gains over time in global self-esteem, domain-specific physical self-esteem, and all subdomain-specific measures of self-esteem. Specifically, Tai Chi participants reported higher levels of perceptions within the three specific subdomains of the physical self (i.e., attractive body, physical strength, and physical condition) and general overall physical self-worth as a
84
Journal of Applied Gerontology
Table 4. Growth Curve Results of the Randomized Controlled Trial (Group by Time Interaction)
Variable
Estimate ( , N = 94)
Global self-esteem Physical self-worth Attractive body Physical strength Physical condition
.23*** .23*** .13** .20*** .37**
**p < .01. ***p < .001.
Table 5. Correlations Among Change Scores of Dimensions of Self-Esteem (Tai Chi Group, n = 40)
Variable Global self-esteem (GSE) Physical self-worth (PSW) Attractive body (AB) Physical strength (PS) Physical condition (PC)
GSE 1.000 .310* a .203 a –.077 a .159
PSW
AB
PS
PC
1.000 .717*** 1.000 .587*** .641*** 1.000 .671*** .728*** .665*** 1.000
a. Nonsignificant. *p < .05. ***p < .001.
result of the 6-month Tai Chi participation. The results also indicated support for the proposed hierarchical structure of self-esteem in that subdomain levels of esteem were shown to be mediated by the domain-specific level of physical self-worth. Finally, changes in these subdomain-specific physical esteem measures were shown to be interrelated, suggesting change in one specific subdomain of physical self-esteem is likely to be associated with change in another. This latter finding also supports a multidimensional perspective to self-esteem. Two findings are of particular interest. First, results from this study indicated that changes in esteem are more dramatic in the first half of the intervention (i.e., the first 3 months) and maintained beyond that time, although the experimental participants were still experiencing more positive changes in esteem than the control group. The leveling off of the intervention effect in the later stage of the study measurement period may be due to (a) the frequency and intensity of the activity (i.e., meeting two times per week, using simplified movements) and (b) the attrition rate taking place during that
Li et al. / Tai Chi and Multidimensional Self-Esteem
85
period. The flattening of intervention effects argues for implementing strategies, including booster sessions, possibly at 3 months after an intervention begins. Second, although the global measure of self-esteem is expected theoretically to be stable, the observed change in this study is an interesting one. As noted earlier, Kutner et al. (1997) reported no change in global self-esteem between experimental groups or over time. It is not clear why this discrepancy between the two studies exist. The implications of the findings are clear: Tai Chi can be used to improve older adults’ perceptions of their physical ability. In addition, changes in the subdomains of physical self-esteem are positively correlated, indicating interrelated evaluative physical self-perceptions. The change in physical self-worth is important as it seems to influence change at a higher level and may carry mental well-being qualities of its own (Fox, 1997). Overall, because physical activity is generally associated with significant improvements in self-esteem (McAuley, 1994; Sonstroem, 1984), and self-esteem represents an important element of the emotional aspect of health-related quality of life and psychological well-being (Blascovich & Tomaka, 1991; Diener, 1984; Rejeski, Brawley, & Shumaker, 1997; Rosenberg, 1965; Rosenberg et al., 1995), the multifaceted improvements resulting from Tai Chi may be important for aging adults who experience negative life changes and transitions such as personal health changes and loss of functional productivity. The positive relationship between Tai Chi and physical self-esteem implies satisfaction and pride in one’s physical capabilities through physical activity participation and is likely to provide older adults with a positive mental outlook and emotional benefits. In this respect, future Tai Chi intervention studies that focus on older adults who have had their self-concept damaged through dramatic life events may prove to be particularly fruitful. The distinct advantages of Tai Chi serving as a form of physical activity are its capacity to be performed at any time or place and that it does not require special equipment. These characteristics are likely to motivate program involvement and adherence among elderly individuals who are often constrained by transportation and other limitations. This study, along with findings from other physiological- and psychological-based studies, provides hope that relatively simple community-based interventions might maintain or improve overall well-being in older adults. Despite the theoretically consistent findings of the study, there are several limitations that need to be considered when planning future research. First, having no physiological measures at baseline and end of the program prevented us from fully evaluating the exercise and self-esteem model (Sonstroem, 1997; Sonstroem & Morgan, 1989). Employing Sonstreom and Morgan’s exercise/
86
Journal of Applied Gerontology
self-esteem model in the future would allow us to examine whether changes in actual physical parameters influence changes in subdomain physical esteem (e.g., McAuley, Blissmer, Katula, Mihalko, & Duncan, 2000; McAuley, Mihalko, & Bane, 1997). Second, it is not possible to assess the long-term impact of Tai Chi on multidimensional self-esteem due to the absence of follow-up measures. Thus, future studies will benefit by considering follow-up measures that would allow researchers to determine whether observed effects are maintained following program conclusion. Third, the study sample was composed of volunteers who might have been more highly motivated to participate in activity than the typical sedentary older adult population. In addition, the mode of advertising the study (local newspapers, senior center flyers, retirement community notices) may create a selection bias toward people who receive and read newspapers and those who live in or visit certain locales in the community. Therefore, the sample might not be representative of the older adult population as a whole. Finally, although the randomized nature of the study is a strength, we must be mindful of the absence of an attentional control group. Our experimental protocol did not control for the influence of attention on the outcome measures. It is possible that the participants in the Tai Chi group were benefiting from the social support and attention provided in the classes with respect to both the outcome variables and compliance. Further studies should control for this effect by having the control participants attend nonexercise education classes in a group format (e.g., Wolf et al., 1996). The research findings presented in this study are preliminary. Tai Chi– induced effects at multidimensional hierarchical levels of self-esteem across populations need to be further documented. Subsequent research might be aimed at replicating and extending the present findings, especially with a larger sample and for a longer period. Direct comparisons between traditional physical activity modes and Tai Chi in enhancing self-perceptions would be helpful to further substantiate the benefits of Tai Chi. Also, further examination of social, cognitive, physical, behavioral, and environmental influences on self-esteem in the context of Tai Chi are called for, as is further validation of the measures and conceptual models employed in this area. In conclusion, results from this study indicated that Tai Chi could be useful as an alternative form of exercise for improving multidimensional physical self-esteem in older adults. The findings of this study, in conjunction with the existing research on tai chi, suggest that mental health may be enhanced without strenuous activity such as jogging. Given the host of psychological, social, and physical problems associated with aging (e.g., experiencing life changes and transitions such as loss of a partner or independence, negative
Li et al. / Tai Chi and Multidimensional Self-Esteem
87
personal health changes, loss of productivity, changing living arrangements), developing health-promoting, low-cost, and low-technology activities such as Tai Chi would appear to be particularly important for older adults to improve their psychological well-being, physical health, and ultimately, their quality of life.
References Bandura, A. (1986). Self-efficacy mechanism in human agency. American Psychologist, 37, 122-147. Blascovich, J., & Tomaka, J. (1991). Measures of self-esteem. In J. P. Robinson, P. R. Shaver, & L. S. Wrightsman (Eds.), Measures of personality and social psychological attitudes (Vol. 1, pp. 115-160). San Diego, CA: Academic Press. Bryk, A. S., & Raudenbush, S. W. (1992). Hierarchical linear models: Applications and data analysis methods. Newbury Park, CA: Sage. Byrne, B. M. (1996). Measuring self-concept across the life span: Issues and instrumentation. Washington, DC: American Psychological Association. Chen, W. W., & Sun, W. Y. (1997). Tai Chi Chuan, an alternative form of exercise for health promotion and disease prevention for older adults in the community. International Quarterly of Community Health Education, 16, 333-339. Diener, E. (1984). Subjective well-being. Psychological Bulletin, 95, 542-575. Folkins, C. H., & Sime, W. E. (1981). Physical fitness training and mental health. American Psychologist, 36, 373-389. Fox, K. R. (1997). The physical self and processes in self-esteem development. In K. R. Fox (Ed.), The physical self: From motivation to well-being (pp. 111-139). Champaign, IL: Human Kinetics. Fox, K. R., & Corbin, C. B. (1989). The physical perception profile: Development and preliminary validation. Journal of Sport & Exercise Psychology, 11, 408-430. Hedeker, D., & Gibbons, R. D. (1997). Application of random-effects pattern-mixture models for missing data in longitudinal studies. Psychological Methods, 2, 64-78. Hughes, J. R. (1984). Psychological effects of habitual aerobic exercise: A critical review. Preventive Medicines, 13, 66-78. Jacobson, B. H., Chen, H-C., Cashel, C., & Guerrero, L. (1997). The effect of T’ai Chi Chuan training on balance, kinesthetic sense, and strength. Perceptual and Motor Skills, 84, 27-33. Kutner, N. G., Barnhart, H., Wolf, S. L., McNeely, E., & Xu, T. (1997). Self-report benefits of Tai Chi practice by older adults. Journal of Gerontology: Psychological Science, 5, P242-P246. Li, F., Duncan, T. E., Duncan, S. C., McAuley, E., Chaumeton, N. R., & Harmer, P. (2001). Enhancing the psychological well-being of elderly individuals through Tai Chi exercise: A latent growth curve analysis. Structural Equation Modeling: A Multidisciplinary Journal, 8, 53-83. Li, F., McAuley, E., Harmer, P., Duncan, T. E., Chaumeton, N. R., & Duncan, S. C. (2001). Tai Chi enhances self-efficacy and exercise behavior in older adults. Journal of Aging and Physical Activity, 9, 161-171. Little, R.J.A., & Yau, L. (1996). Intent-to-treat analysis in longitudinal studies with drop-outs. Biometrics, 52, 1324-1333.
88
Journal of Applied Gerontology
Marsh, H. W. (1997). The measurement of physical self-concept: A construct validation approach. In K.F.J. Fox (Ed.), The physical self: From motivation to well-being (pp. 27-58). Champaign, IL: Human Kinetics. McAuley, E. (1994). Physical activity and psychosocial outcomes. In C. Bouchard, R. J. Shephard, & T. Stephens (Eds.), Physical activity, fitness, and heath: The consensus knowledge (pp. 551-578). Champaign, IL: Human Kinetics. McAuley, E., Blissmer, B., Katula, J., Mihalko, S. L., & Duncan, T. E. (2000). Physical activity, self-esteem, and self-efficacy relationships in older adults: A randomized controlled trial. Annals of Behavioral Medicine, 22, 131-139. McAuley, E., Katula, J., Mihalko, S. L., Blissmer, B., Duncan, T. E., Pena, M., et al. (1999). Mode of physical activity and self-efficacy in older adults: A latent growth curve analysis. Journal of Gerontology: Psychological Sciences, 54B, P283-P292. McAuley, E., Mihalko, S. L., & Bane, S. M. (1997). Exercise and self-esteem in middle-aged adults: Multidimensional relationships and physical fitness and self-efficacy influences. Journal of Behavioral Medicine, 20, 67-83. Meredith, W., & Tisak, J. (1990). Latent curve analysis. Psychometrika, 55, 107-122. Rejeski, W. J., Brawley, L. R., & Shumaker, S. A. (1997). Physical activity and health-related quality of life. Exercise and Sport Science Reviews, 16, 1-50. Rosenberg, M. (1965). Society and the adolescent self-image. Princeton, NJ: Princeton University Press. Rosenberg, M., Schooler, C., Schoenbach, C., & Rosenberg, F. (1995). Global self-esteem and specific self-esteem: Different concepts, different outcomes. American Sociological Review, 60, 141-156. SAS Institute, Inc. (1992). SAS/STAT: User’s guide. Cary, NC: Author. Schaller, K. J. (1996). Tai Chi Chih: An exercise option for older adults. Journal of Gerontology Nursing, 22, 12-17. Sonstroem, R. J. (1984). Exercise and esteem. Exercise and Sport Sciences Reviews, 12, 123-153. Sonstroem, R. J. (1997). The physical self-system: A mediator of exercise and self-esteem. In K. R. Fox (Ed.), The physical self: From motivation to well-being (pp. 3-26). Champaign, IL: Human Kinetics. Sonstroem, R. J. (1998). Physical self-concept: Assessment and external validity. Exercise and Sport Sciences Reviews, 12, 133-164. Sonstroem, R. J., & Morgan, W. P. (1989). Exercise and self-esteem: Rationale and model. Medicine and Science in Sports and Exercise, 21, 329-337. Tse, S. K., & Bailey, D. M. (1992). T’ai Chi and postural control in the well elderly. American Journal of Occupational Therapy, 46, 259-300. Washburn, R. A., Smith, K. W., Jette, A. M., & Janney, C. A. (1993). The Physical Activity Scale for the Elderly (PASE): Development and evaluation. Journal of Clinical Epidemiology, 46, 153-162. Wolf, L. S., Barnhart, H. X., Kutner, N. G., et al. (1996). Reducing frailty and falls in older persons: An investigation of Tai Chi and computerized balance training. Journal of American Geriatrics Society, 44, 489-497. Wolfson, L., Whipple, R., Derby, C., Judge, J., King, M., Amerman, P., et al. (1996). Balance and strength training in older adults: Intervention gains and Tai Chi maintenance. Journal of American Geriatrics Society, 44, 498-506. Young, D. R., Appel, L. J., Jee, S., & Miller, E. R. (1999). The effects of aerobic exercise and T’ai Chi on blood pressure in older people: Results of a randomized trial. Journal of American Geriatrics Society, 47, 277-284.
Li et al. / Tai Chi and Multidimensional Self-Esteem
Article accepted April 7, 2000.
Fuzhong Li received a Ph.D. in human performance from Oregon State University and is a research scientist at Oregon Research Institute in Eugene, Oregon. His research interests include exercise health and motivation and statistical methodology. Recent work includes (with T. E. Duncan, E. McAuley, P. Harmer, & K. Smolkowski) “Latent Curve Analysis of Longitudinal Data on Aging” in the Journal of Aging and Health 12 (2001). Peter Harmer is an associate professor in the Department of Exercise Science at Willamette University in Salem, Oregon. He received an M.Ed. in special education and a Ph.D. in human movement studies from the University of Oregon in 1990. Research interests include epidemiology of injury in sport, cross-cultural aspects of physical activity, and ethics and ergogenic aids. Current publications include (with F. Li, E. McAuley, T. E. Duncan, N. R. Chaumerton, & S. C. Duncan) “Tai Chi Enhances Self-Efficacy and Exercise in Behavior in Older Adults” in the Journal of Aging and Physical Activity 9 (2001). Nigel Chumeton received his Ph.D. in exercise and movement science from the University of Oregon. He is currently associated with the Oregon Research Institute. His research interests include physical activity patterns of children and adults, fall prevention, and physician-patient communication. His published work includes (with W. Levinson) “Communication Between Surgeons and Their Patients During Routine Office Visits” in Surgery, 125 (1999). Terry E. Duncan earned a Ph.D. in physical education and measurement and statistics in 1989 from the University of Oregon. He is a research scientist at the Oregon Research Institute whose interests include statistical methods for longitudinal designs, structural equation modeling, approaches for the analysis of missing data, generalized linear models, the etiology of substance use and development, and exercise and health behavior. Recent publications include (with S. C. Duncan, N. Beauchamp, J. Wells, & D. V. Ary) “Development and Evaluation of an Interactive CD-ROM Refusal Skills Program to Prevent Youth Substance Use: ‘Refuse to Use’” in the Journal of Behavioral Medicine, 23 (2000). Susan D. Duncan received her Ph.D. in physical education from the University of Oregon and is currently a research scientist at the Oregon Research Institute. Her research interests focus on substantive, statistical, and methodological issues related to substance use, problem behaviors, and health-promoting behaviors in adolescents, as in her article (with L. A. Strycker & T. E. Duncan) “Exploring Associations in Developmental Trends of Adolescent Substance Use and Risky Sexual Behavior in a High-Risk Population” in the Journal of Behavioral Medicine, 22 (1999).
89