Case Report ANCA-Associated Glomerulonephritis in Systemic-Onset Juvenile Idiopathic Arthritis Alexandre Belot, MD,1 Brigitte Bader-Meunier, MD,2 Patrick Niaudet, MD,3 Rémi Salomon, MD, PhD,3 Anne-Marie Prieur, MD,2 Laure-Hélène Noel, MD,4 and Pierre Quartier, MD2 Systemic-onset juvenile idiopathic arthritis is an inflammatory disease of unknown cause and is not commonly associated with kidney involvement. We describe 3 patients with systemic-onset juvenile idiopathic arthritis with high disease activity who developed antineutrophil cytoplasmic antibody (ANCA)-associated glomerulonephritis 1-6 years after the onset of systemic-onset juvenile idiopathic arthritis. Renal and systemiconset juvenile idiopathic arthritis remission occurred in one patient under anti–interleukin 1 (anti–IL-1) treatment associated with immunosuppressive drugs. The other 2 patients developed end-stage renal disease, and one of those patients died. This report suggests that the diagnosis of ANCA-associated glomerulonephritis must be considered in patients with systemic-onset juvenile idiopathic arthritis with persistently active systemic disease who present with proteinuria. Furthermore, use of an anti–IL-1 agent might be an effective therapeutic option. Am J Kidney Dis. 59(3):439-443. © 2012 by the National Kidney Foundation, Inc. INDEX WORDS: Crescent glomerulonephritis; antineutrophil cytoplasmic antibody (ANCA)-associated glomerulonephritis; ANCA-associated vasculitis; autoinflammatory disease; juvenile idiopathic arthritis; pediatrics.
J
uvenile idiopathic arthritis is one of the most common rheumatic diseases occurring in childhood, with a prevalence estimated at 2 in 10,000 children younger than 16 years.1 Systemic-onset juvenile idiopathic arthritis is characterized by spiking fever associated with skin rash, serositis, lymphadenopathy, and hepatosplenomegaly.2 Kidney lesions consist mainly of secondary amyloidosis, a complication for which the incidence has dramatically decreased after the introduction of effective treatment.3 Only a few cases of nonamyloid glomerular lesions have been reported, comprising membranous nephropathy,4,5 mesangial glomerulonephritis,6 focal segmental glomerulosclerosis,6 and antineutrophil cytoplasmic antibody (ANCA)-negative crescentic glomerulonephritis.5 ANCAs recognize lysosomal enzymes of human neutrophils and monocytes and are classified into 2 main groups. The first are ANCAs against myeloperoxidase (MPO) and more typically are found in ANCA-associated glomerulonephritis, microscopic polyangiitis, and Churg-Strauss syndrome. The second are against serine proteinase 3 (PR3) and are highly specific for granulomatosis with polyangiitis (Wegener). Here, we report what to our knowledge is the first description of children with systemic-onset juvenile idiopathic arthritis presenting with ANCAassociated necrotizing glomerulonephritis. We discuss the presentation, treatment, and outcome of 3 cases, as well as possible underlying immunologic disorders. Am J Kidney Dis. 2012;59(3):439-443
CASE REPORTS Case 1 Patient 1 was an 11-month-old girl who presented with typical symptoms of systemic-onset juvenile idiopathic arthritis (Table 1). Serologic investigations and the clinical course ruled out tumor- or infection-associated manifestations. Nonsteroidal anti-inflammatory drugs and aspirin failed to control the symptoms and oral corticotherapy was begun. Eleven months after disease onset, nephritic syndrome with acute kidney failure (estimated glomerular filtration rate [eGFR], 50 mL/min [0.83 mL/s] by the Schwartz formula7) led to the diagnosis of extracapillary glomerulonephritis with MPO-ANCA. Treatment consisted of high-dose steroid infusions along with pulsed intravenous (IV) cyclophosphamide and methotrexate. She experienced several episodes of melena during follow-up. Unfortunately, the child presented with end-stage renal disease (ESRD) at the age of 12 years and developed advanced
From the 1Service de Néphrologie et Rhumatologie Pédiatriques et CNRS UMR5239, Hôpital Femme Mère Enfant, Lyon; 2 Service d’Immuno-Hémato-Rhumatologie, Hôpital Necker-Enfant Malades, 3Service de Néphrologie Pédiatrique et U574, and 4 Service d’Anatomie Pathologique, Hôpital Necker-Enfants Malades, Paris, France. Received March 5, 2011. Accepted in revised form September 28, 2011. Originally published online December 22, 2011. Address correspondence to Alexandre Belot, MD, Service de Néphrologie & Rhumatologie Pédiatrique, Blvd Pinel, Hôpital Femme Mère Enfant, 69677 Bron Cedex, France (E-mail:
[email protected]) or Pierre Quartier, MD, Service d’Immunologie, Hématologie et Rhumatologie Pédiatriques, Hôpital Necker-Enfants Malades, 149, rue de Sèvres 75015, Paris, France (E-mail:
[email protected]). © 2012 by the National Kidney Foundation, Inc. 0272-6386/$36.00 doi:10.1053/j.ajkd.2011.11.002 439
440 Table 1. Patients’ Characteristics ANCA Level Patient No. Sex/Age at Diagnosisa
Symptoms at Diagnosis
Lab Data at Diagnosis
ESR ⬎100 mm/h; WBC, 20 ⫻ 103/L; ANA titer, 1/120; SCr, 0.7 mg/dL ESR, 77 mm/h; WBC, 18 ⫻ 103/ L; platelet count, 1,150 ⫻ 103/ L; ANA titer, 1/200; AST, 2N; ALT, 2N; SCr, 0.9 mg/dL
1: F/11 mo
Fever, polyarthritis, cutaneous rash, splenomegaly
2: F/4 y
Fever, polyarthritis, cutaneous rash, hepatosplenomegaly
3: M/1.5 y
Fever, severe polyarthritis, ESR ⬎80 mm/h; WBC, 23 ⫻ 103/ hepatomegaly, L; ANA, undetectable; SCr, abdominal pain 0.5 mg/dL
Time to GNb (y)
At Diagnosis
1
ND
pANCA⫹
Articular destruction, Corticosteroids, NSAID, ESRD, HD, death CYP, MTX
6
—c
MPO-ANCA, 20 U/L (pretransplant, 35 U/L; peak during recurrence, 49 U/L)
4
—c
MPO-ANCA, 23 U/L (range, —c to 43 U/L)
Articular destruction, Corticosteroids, AZA; ESRD, kidney after kidney transplant, GN transplant: MMF, recurrence corticosteroids, rituximab Articular destruction, Corticosteroids, NSAID, normal kidney MTX, anti–TNF-␣, function thalidomide, rituximab, anti–IL-1
At GN Onset (and f/u)
Outcome
Treatment
Belot et al
Am J Kidney Dis. 2012;59(3):439-443
Note: Conversion factor for units: SCr in mg/dL to mol/L, ⫻88.4; no conversion necessary for WBC and platelet counts in ⫻ 103/L and ⫻ 109/L. Abbreviations: 2N, twice the normal level; ALT, alanine aminotransferase; ANA, antinuclear antibodies; ANCA, antineutrophil cytoplasmic antibody; AST, aspartate aminotransferase; AZA, azathioprine; CYP, cyclophosphamide; ESR, erythrocyte sedimentation rate; ESRD, end-stage renal disease; f/u, follow-up; GN, glomerulonephritis; HD, hemodialysis; IL-1, interleukin 1; lab, laboratory; MMF, mycophenolate mofetil; MPO, myeloperoxidase; MTX, methotrexate; ND, not done; NSAID, nonsteroidal anti-inflammatory drug; pANCA, perinuclear antineutrophil cytoplasmic antibody; SCr, serum creatinine; TNF-␣, tumor necrosis factor ␣; WBC, white blood cell. a Diagnosis refers to diagnosis of systemic-onset juvenile idiopathic arthritis. b Interval between juvenile idiopathic arthritis and GN. c Undetectable.
Still Disease and MPO-ANCA Glomerulonephritis
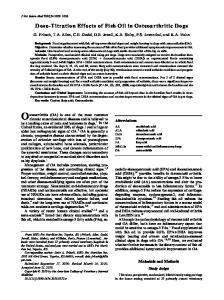
Figure 1. Kidney biopsies of patients (Pts) (A) 2 and (B) 3. (A) Upper panels show fibrocellular crescent responsible for flocculo-capsular adhesion (black arrow) associated with periglomerular inflammation (red arrow; original magnification, ⫻250). Lower panels show one glomerulus with isolated segmental necrosis (black arrow) and 2 glomeruli with sclerosis associated with extracapillary proliferation (red arrows; original magnifications, ⫻400 and ⫻250, respectively). (B) Upper panels show a cellular crescent (black arrow; light green trichrome) and, by immunofluorescence, segmental fixation of antifibrinogen antibody (original magnification, ⫻400). Lower panels show a segmental fibrous lesion (red arrow) and fibrocellular crescent corresponding to the evolution of a cellular crescent (black arrow; original magnification, ⫻400).
cachexia. Four years later, she developed intestinal obstruction, sepsis, and acute respiratory failure associated with cricoarytenoid arthritis and died.
Case 2 Patient 2 was a 4-year-old girl who presented with polyarthritis, rash, and spiking fever with increased erythrocyte sedimentation rate (77 mm/h). Laboratory examinations, including infection screening (by serology and polymerase chain reaction testing) and bone marrow aspiration, ruled out malignancy and infection. Despite treatment with nonsteroidal anti-inflammatory drugs, methotrexate, azathioprine, cyclosporine, cyclophosphamide, aspirin, and IV immunoglobulins, systemic symptoms persisted with an erythrocyte sedimentation rate ⬎70 mm/h. At the age of 10, she presented with nephritic syndrome with kidney failure (eGFR, 63 mL/min [1.05 mL/min]) related to extracapillary glomerulonephritis (Fig 1). MPO-ANCA titer became positive (20 U/L). Initial treatment consisted of pulsed IV steroids followed by azathioprine and oral steroids. A second biopsy was performed 6 months after the first and showed persistent acute lesions in half the glomeruli. The glomerulonephritis led to ESRD, and she needed hemodialysis therapy at the age of 18 years. Systemic symptoms were still present. A kidney transplant was performed at the age of 19 years, allowing restoration of kidney function. Five years after transplant, the patient developed progressive proteinuria, with protein excretion ⬎1 g/24 h leading to a new kidney biopsy. MPO-ANCA titer peaked at 49 U/L, and biopsy confirmed ANCA-associated glomerulonephritis (Fig 1). Pulsed IV steroid bolus, rituximab, and mycophenolate mofetil treatment resulted in partial regression of proteinuria.
Case 3 Patient 3 was a young boy with a history of congenital scoliosis, anorexia, and abdominal pain. He needed oral tube feeding during the first months of life. At the age of 16 months, he presented with polyarthritis, fever, and erythrocyte sedimentation rate up to 80 mm/h. Bone marrow and blood investigations ruled out infections and malignancies. Autoantibody screening was negative for rheuAm J Kidney Dis. 2012;59(3):439-443
matoid factor, ANCA, and antinuclear antibody. Persistent inflammation led to the diagnosis of systemic-onset juvenile idiopathic arthritis. Despite treatment with nonsteroidal anti-inflammatory drugs, steroids, methotrexate, thalidomide, and anti–tumor necrosis factor agents, arthritis became erosive and systemic inflammation persisted. When he was 6 years old, he presented with macroscopic hematuria, proteinuria, and abdominal pain. Creatinine level was slightly increased (0.5 mg/dL [44.2 mol/L], corresponding to eGFR of 80 mL/min [1.33 mL/min]) at diagnosis. Kidney biopsy showed extracapillary glomerulonephritis (Fig 1). MPO-ANCA titer was positive (23 U/L). Initial treatment consisted of steroid pulses and rituximab. Rituximab was replaced by mycophenolate mofetil after the third infusion because of severe allergic symptoms (Quinck edema). A control biopsy was performed 5 months after the onset and showed evolution into fibrous scars without acute lesions. ANCA titer remained at 29 U/L. Interleukin 1 (IL-1) receptor antagonist (anakinra) treatment (daily dose, 5 mg/kg of body weight) was started, and rapid improvement was observed for both fever and arthritis. MPO-ANCA became undetectable. At the age of 8 years, proteinuria disappeared, kidney function was normal, and the child experienced no more active arthritis or fever. Anakinra therapy was switched to the anti–IL-1 monoclonal antibody canakinumab and mycophenolate mofetil therapy was stopped. At last follow-up 5 years later, systemic-onset juvenile idiopathic arthritis was in complete remission and kidney function was normal without proteinuria.
DISCUSSION To our knowledge, we report for the first time cases of MPO-ANCA–associated glomerulonephritis during the course of systemic-onset juvenile idiopathic arthritis. All 3 patients had persistently active systemic disease with destructive polyarthritis and fulfilled systemic-onset juvenile idiopathic arthritis diagnosis criteria.2 ANCA appeared when glomerulonephritis was diagnosed. Anti–IL-1 treat441
Belot et al
ment induced remission of systemic-onset juvenile idiopathic arthritis and glomerulonephritis in one patient. The diagnosis of systemic-onset juvenile idiopathic arthritis was made on the basis of typical systemic features, including spiking fever in all patients, and erosive polyarthritis with cartilage destruction. Because ANCA-related vasculitis is responsible for nondestructive arthritis, it is unlikely that the initial disease was ANCA-related vasculitis. In addition, ANCA was undetectable at disease onset in 2 cases (patients 2 and 3) and unknown in the other case (patient 1). A few drugs may induce ANCA-related vasculitis, such as D-penicillamine or propylthiouracil, but none was used in our patients. Strikingly, ANCA specificity was MPO in our 3 cases. Two of them presented with digestive symptoms, such as abdominal pain, melena, and anorexia, that might be part of the microscopic polyangiitis spectrum. Nevertheless, no lung involvement or skin vasculitis was present, although these are classic features of microscopic polyangiitis. Kidney involvement is very uncommon in patients with juvenile idiopathic arthritis. In addition to secondary amyloidosis, nonamyloid glomerular lesions have been reported in few patients. When present, they usually consist of membranous nephropathy,5 mesangial glomerulonephritis,6,8 focal segmental glomerulosclerosis,6 or crescentic glomerulonephritis.5,9 The presence of ANCA-associated vasculitis seems to be associated with a particularly poor renal outcome in systemic-onset juvenile idiopathic arthritis. Here, 2 patients developed ESRD and 1 died. We found 3 patients with juvenile idiopathic arthritis in the literature with ANCA-associated disease, 2 who developed kidney lesions and ESRD despite immunosuppressive treatments6,9,10 (Table S1, available as online supplementary material). In contrast, typically only a quarter of patients with ANCA-associated glomerulonephritis experience a poor renal outcome.11 In addition, recurrence of ANCA-associated glomerulonephritis after transplant is very uncommon12; hence, the outcome of patient 2 who experienced recurrence of ANCAassociated vasculitis on the transplanted kidney also suggests that ANCA-associated vasculitis is particularly aggressive in patients with systemic-onset juvenile idiopathic arthritis.12 Interestingly, the presence of perinuclear ANCA in patients with rheumatoid arthritis seems to be a marker of progressive erosive disease and is associated with kidney disease.13 Strikingly, in all 3 reported cases and in the literature, ANCA was directed against MPO. MPO-ANCA was monitored in patients 2 and 3, showed a titer increase during posttransplant recurrence in patient 2, and levels were undetectable after IL-1 antagonist introduction in patient 3, suggesting that ANCA titer correlates 442
with kidney disease activity. In patients with systemiconset juvenile idiopathic arthritis with persistently active systemic disease and erosive arthritis, careful kidney function assessment is mandatory. If proteinuria or kidney failure appears, ANCA-associated glomerulonephritis might be considered in addition to amyloidosis. Systemic-onset juvenile idiopathic arthritis and ANCA-associated diseases might share a common pathogenesis. In our patients, when ANCA-associated glomerulonephritis developed, systemic inflammation was not controlled despite a large combination of immunosuppressants. IL-1 is a cornerstone of systemic-onset juvenile idiopathic arthritis pathogenesis,14 and patient 3 achieved remission of both systemic-onset juvenile idiopathic arthritis and ANCAassociated kidney disease with anti–IL-1 treatment. Additional reports indicate that IL-1 gene polymorphisms favor ESRD in PR3-ANCA glomerulonephritis.15 Proinflammatory stimuli and ANCA are believed to synergize and contribute directly to vascular inflammation,16 and the systemic-onset juvenile idiopathic arthritis proinflammatory cytokine environment might promote ANCA-associated diseases. Interestingly, crescentic glomerulonephritis also has been reported as part of hyperimmunoglobulin D syndrome,17 which is associated with increased IL-1 production. In conclusion, this report suggests that the diagnosis of ANCA-associated glomerulonephritis must be considered in patients with systemic-onset juvenile idiopathic arthritis with persistently active systemic disease who present with proteinuria. An anti–IL-1 agent was associated with remission of both systemic-onset juvenile idiopathic arthritis and ANCA-associated kidney disease in one patient, which raises the question of IL-1 inhibitor use in patients with systemic inflammation and ANCAassociated vasculitis.
ACKNOWLEDGEMENTS We acknowledge Uzma Hasan for proofreading and corrections. Support: None. Financial Disclosure: The authors declare that they have no relevant financial interests.
SUPPLEMENTARY MATERIAL Table S1: Cases of ANCA-associated diseases in juvenile idiopathic arthritis. Note: The supplementary material accompanying this article (doi:10.1053/j.ajkd.2011.11.002) is available at www.ajkd.org
REFERENCES 1. Quartier P, Prieur AM. [Juvenile idiopathic arthritis. (I) Clinical aspects]. Rev Prat. 2007;57(11):1171-1178. 2. Petty RE, Southwood TR, Manners P, et al. International League of Associations for Rheumatology classification of juveAm J Kidney Dis. 2012;59(3):439-443
Still Disease and MPO-ANCA Glomerulonephritis nile idiopathic arthritis: second revision, Edmonton, 2001. J Rheumatol. 2004;31(2):390-392. 3. Immonen K, Savolainen HA, Hakala M. Why can we no longer find juvenile idiopathic arthritis-associated amyloidosis in childhood or in adolescence in Finland? Scand J Rheumatol. 2007;36(5):402-403. 4. Suzuki K, Tanaka H, Ito E, Waga S. Therapy-related membranous nephropathy in juvenile idiopathic arthritis with Turner syndrome. Pediatr Int. 2004;46(3):377-379. 5. Foster BJ, Duffy CM, Sharma AK. Systemic juvenile rheumatoid arthritis complicated by two different renal lesions. Pediatr Nephrol. 1998;12(2):113-116. 6. Gedalia A, Mendez EA, Craver R, Vehaskari M, Espinoza LR. Renal involvement in juvenile rheumatoid arthritis: report of two cases. Clin Rheumatol. 2001;20(2):153-156. 7. Schwartz GJ, Munoz A, Schneider MF, et al. New equations to estimate GFR in children with CKD. J Am Soc Nephrol. 2009;20(3):629-637. 8. Kari JA, Bamashmous H, Mahan JD. Steroid-sensitive nephrotic syndrome and juvenile idiopathic arthritis. Pediatr Nephrol. 2002;17(11):975-976. 9. Dhib M, Prieur AM, Courville S, et al. Crescentic glomerulonephritis in juvenile chronic arthritis. J Rheumatol. 1996;23(9):1636-1640. 10. Wedderburn LR, Kwan JT, Thompson PW, Rudge SR. Juvenile chronic arthritis and Wegener’s granulomatosis. Br J Rheumatol. 1992;31(2):121-123.
Am J Kidney Dis. 2012;59(3):439-443
11. Lionaki S, Hogan SL, Jennette CE, et al. The clinical course of ANCA small-vessel vasculitis on chronic dialysis. Kidney Int. 2009;76(6):644-651. 12. Gera M, Griffin MD, Specks U, Leung N, Stegall MD, Fervenza FC. Recurrence of ANCA-associated vasculitis following renal transplantation in the modern era of immunosupression. Kidney Int. 2007;71(12):1296-1301. 13. Mustila A, Korpela M, Mustonen J, et al. Perinuclear antineutrophil cytoplasmic antibody in rheumatoid arthritis: a marker of severe disease with associated nephropathy. Arthritis Rheum. 1997;40(4):710-717. 14. Pascual V, Allantaz F, Arce E, Punaro M, Banchereau J. Role of interleukin-1 (IL-1) in the pathogenesis of systemic onset juvenile idiopathic arthritis and clinical response to IL-1 blockade. J Exp Med. 2005;201(9):1479-1486. 15. Borgmann S, Endisch G, Hacker UT, Song BS, Fricke H. Proinflammatory genotype of interleukin-1 and interleukin-1 receptor antagonist is associated with ESRD in proteinase 3-ANCA vasculitis patients. Am J Kidney Dis. 2003;41(5):933942. 16. Heeringa P, Huugen D, Tervaert JW. Anti-neutrophil cytoplasmic autoantibodies and leukocyte-endothelial interactions: a sticky connection? Trends Immunol. 2005;26(11):561564. 17. Cailliez M, Garaix F, Rousset-Rouviere C, et al. Crescentic glomerulonephritis is part of hyperimmunoglobulinemia D syndrome. Pediatr Nephrol. 2006;21(12):1917-1918.
443