Program name:
Counselling patients on the latest developments in combination oral contraceptive dispensing devices
Faculty:
Deborah Rigby, BPharm GradDipClinPharm CGP FPS FASCP FACP AACPA FAICD
Accreditation information:
This version of the program is unaccredited and intended for informational purposes only. An accredited version is available online at www.mdbriefcase.com.au
Sponsor:
This program is sponsored by an educational grant from Bayer.
Page 1 of 29 © Copyright 2014 This version of the program is unaccredited and intended for informational purposes only. An accredited version is available online at www.mdbriefcase.com.au
Learning objectives After participating in this program, participants will be better able to:
Explain the role of oral contraceptives with flexible and extended regimens.
Recognise factors that influence non-adherence to oral contraception regimens and how to address them.
Evaluate the role of a delivery system in improving adherence to therapy.
Counsel patients on how to administer oral contraceptives through a digital dispensing system.
Counsel patients regarding adverse effects associated with oral contraceptives.
Page 2 of 29 © Copyright 2014 This version of the program is unaccredited and intended for informational purposes only. An accredited version is available online at www.mdbriefcase.com.au
MD Briefcase Pre-Course Survey 1. Please indicate the extent to which you agree or disagree with the following statements by using a scale of 1 to 10 where 1=strongly disagree and 10=strongly agree
Statements
Strongly disagree.........Strongly agree
1
2
3
4
5
6
7
8
9
10
1. Adverse effects associated with hormonal contraception such as headache, pelvic pain and cramping, breast tenderness, bloating, swelling, are associated with the pill-free interval rather than the hormonal phase, 2. Oral contraceptive regimens with a pill-free interval of 7 days are medically preferred over other regimens as they mimic the natural menstrual cycle. 3. I am proficient in addressing the concerns of younger patients regarding the long-term use of oral contraceptives. 4. I can confidently demonstrate and counsel patients on the latest developments in combination oral contraceptive dispensing devices. 5. I can confidently counsel patients on the importance of adherence to oral contraceptives. Page 3 of 29 © Copyright 2014 This version of the program is unaccredited and intended for informational purposes only. An accredited version is available online at www.mdbriefcase.com.au
Background Contraceptive use has increased exponentially in the past 50 years and is considered to be one of the most significant public health successes of the 20th century. In developing countries contraceptive prevalence has increased from 10% in the early 1960s to 60% in 2009 with >70% in developed countries using contraceptive methods.1 The combined oral contraceptive (COC) pill remains the most commonly used method of contraception in Australia as it is in the UK and US.2 In addition to the contraceptive effects, there are a number of benefits associated with the COC pill. The cycle is more regular and the menstruation is often less painful and bleeding is lighter.3 With the higher-dose COCs (50 μg ethinyloestradiol), there is evidence of a reduced risk of fibrocystic tumours of the breasts, ovarian cysts, pelvic inflammatory disease, ectopic pregnancy and endometrial and ovarian cancer. Whether this applies to lower-dosed COCs remains to be confirmed.3 Long-term use may also preserve fertility by decreasing and delaying the incidence of endometriosis.4 Combined oral contraceptives may also be useful in treating acne vulgaris.3 Understanding the needs of your patient Since the introduction of the contraceptive pill in the 1960s, attitudes to periods have changed. A study by Greig et al at an Australian university reported that 66% of surveyed students aged under 25 years have skipped their period at some time, with the most common reason cited being convenience (89%).5 Australia now has an oral contraceptive pill that offers different regimens to allow for greater flexibility and longer cycles without menstruation.3 Forum question In your opinion, what features of a COCP do women most appreciate?
Page 4 of 29 © Copyright 2014 This version of the program is unaccredited and intended for informational purposes only. An accredited version is available online at www.mdbriefcase.com.au
Selecting a COCP to meet patient needs Until recently, contraceptive development has focused on strategies to decrease the prevalence of unwanted adverse effects. Such strategies included a decrease in oestrogen and progestogen content, the development of specific progestogens and the use of phasic regimens. However, with a decreased steroid dose, concerns of escape ovulation and subsequent contraceptive failure arose. As a result, more recently there has been increased focus on shortening the pill-free interval (PFI) as a method of minimising any potential decrease in efficacy associated with low-dose COCPs.1 Use of extended COCPs may also help women with regard to flexibility in dosing and menstruating less frequently.3 Studies have shown that most women prefer at times to delay or avoid menstruation.6 There are several other potential advantages to decreasing the frequency of menstruation through continuous dosing, including:6
Improved adherence to COCPs
Less interference with daily activities or special events
Decreased expense for feminine hygiene products
Less menstruation-related absenteeism from work or school.
Research also suggests that many of the adverse effects associated with COCPs such as headache, pelvic pain, back pain and oedema are reported more commonly in the PFI.7 Approximately 74% (95% CI 60-85%) of women (n=50) aged 19-50 with PFI-associated symptoms who were followed in a small prospective study reported that extending their oral contraceptive active pills delayed the onset and decreased the severity of the symptoms experienced during the PFI.8 Research by Sulak et al tracked symptoms of 262 women throughout their cycle. They concluded that all symptoms assessed were significantly worse during the 7 day hormone free interval. 9 Table 1 illustrates the proportion of COCP-related side-effects which occurred during the PFI in this study.7, 9
Page 5 of 29 © Copyright 2014 This version of the program is unaccredited and intended for informational purposes only. An accredited version is available online at www.mdbriefcase.com.au
Table 1: Distribution of COCP-related complaints which occurred during the pill-free interval.7, 9
From data of Sulak et al.9
Test yourself question: Which COCPs currently available in Australia do not follow the traditional 21/7 day cycle?
Addressing patient concerns In the past, women had infrequent menstruation due to marriage at a younger age, multiple pregnancies and breastfeeding for longer periods of time. Women in previous generations are reported to have had less than 160 menstruations per lifetime whilst women today will have approximately 450 menstruations. 6, 10
Did you know? COCPs were originally designed with a 21/7 day cycle due to cultural and societal pressures.10 Dr. Gregory Pincus, the principal contributor to the development of oral contraceptives, decided upon the 21/7 day cycle when developing the new product. He believed that a traditional 21/7 day cycle mimicked naturally occurring menstrual cycles and would therefore be more acceptable to women, clinicians and churches. The decision was founded upon cultural and social pressures rather than biological considerations.6, 10 During the last 10 years there has been much interest in extended pill regimens. Continuous pill regimens are not new; their use has been available in the US for some years. Continuous regimens involve taking a low-dose COCP for 3 or 4 months continuously followed by a standard 7-day PFI.1
Page 6 of 29 © Copyright 2014 This version of the program is unaccredited and intended for informational purposes only. An accredited version is available online at www.mdbriefcase.com.au
Extended pill regimens are equally efficacious as traditional regimens in preventing pregnancy. However continuous use may result in increased breakthrough bleeding and spotting compared to the traditional 21/7 day cycle.1 Although breakthrough bleeding commonly occurs in the first few months of extended COCP use, it usually decreases with each subsequent cycle and is comparable to rates seen in traditional 21/7 day cycles by the fourth extended cycle.4 A Cochrane review published in 2006 evaluated the use of COCPs for contraception when used in a cyclic or continuous manner. The review included six randomised controlled trials with results and conclusions as follows: 6
Contraceptive efficacy and compliance were similar in both the continuous and cyclic arms of the trials.
Five out of six studies found that bleeding patterns were similar or improved with continuous-dosing regimens.
Continuous dosing reduced associated symptoms such as menstrual headaches, genital irritation, tiredness, bloating and menstrual pain.
For further information on the Cochrane review, please click here. The knowledge regarding fertility after discontinuation of continuously used COCPs seems limited. A study of 34 women who ceased continuous therapy with a COCP when they planned on becoming pregnant found the pregnancy rate was 57% [95% CI (34-78%)] at three months and 81% [95% CI (58-95%)] at 12 months following discontinuation. The median time from treatment discontinuation to conception was four months.10 From the available literature it is not possible to conclude whether the fertility after discontinuation of OCs after continuous use is the same as for conventionally applied OCs but the pregnancy rate in this study after cessation is not very different from that of the background population. 10 Forum question In your opinion, is the continuous use of COCPs a concern for your patients? How do you counsel these women?
Page 7 of 29 © Copyright 2014 This version of the program is unaccredited and intended for informational purposes only. An accredited version is available online at www.mdbriefcase.com.au
Contraindications to consider when commencing COCPs include:3
Presence or history of venous or arterial thrombotic events
Presence or history of prodromi of a thrombosis
History of migraine with focal neurological symptoms
Diabetes mellitus with vascular involvement
Presence of a severe or multiple risk factor(s) for venous or arterial thrombosis may also constitute a contraindication
Pancreatitis or a history thereof if associated with severe hypertriglyceridemia
Severe hepatic disease as long as liver function values have not returned normal
Severe renal insufficiency or acute renal failure
Presence or history of liver tumours (benign or malignant)
Known or suspected sex-steroid influenced malignancies
Undiagnosed vaginal bleeding
Hypersensitivity to any of the ingredients contained in the COCP
Known or suspected pregnancy
Although the risk of VTE is considered low in COC users (4-5 events per 10,000 women years in non-pregnant COC users, 9-10 events per 10,000 women years in women using COCs, 29 events per 10,000 women years in pregnancy, and may be as high as 300-400 events per 10,000 women years in the immediate postpartum period),11 the risk of VTE increases with: age, smoking, a positive family history, obesity, prolonged immobilisation, new starters or re-starters of combined oral contraceptives (risk is highest during the first year of use), dyslipidaemia, hypertension, migraine, valvular heart disease, and atrial fibrillation.3 Test yourself question: Name three contraindications to COCP use.
Page 8 of 29 © Copyright 2014 This version of the program is unaccredited and intended for informational purposes only. An accredited version is available online at www.mdbriefcase.com.au
Facilitating adherence Computer assisted telephone interviews completed by a random sample of 9,134 Australian women aged 16-59 between mid-2001 and mid-2002 reported that just over 70% of women interviewed used contraception.12 However, despite the high level of contraceptive use, a 2008 survey conducted by Marie Stopes International of Australian women of reproductive age highlighted that 50% of Australian women surveyed had experienced an unplanned pregnancy.13 The BEACH (Bettering the Evaluation and Care of Health) survey, a continuous crosssectional survey of GP activity in Australia (between April 2007 and March 2011), concluded that better understanding of patient perspectives on contraceptive choices could lead to more effective contraceptive use.2 A study by Molloy et al, published in 2012, surveyed 130 female university students taking oral contraception.14 The study found that 52% of women missed their contraceptive pill with 14% missing their pill twice or more per month.14 The study also found that 90% of the sample who never miss their oral contraceptive takes it at the same time each day. Forming a time-related habit to take the pill may be a key in bettering the adherence to oral contraceptives.14 Did you know? Some data has highlighted dispensing larger quantities (1-year supply) of oral contraceptives may reduce unplanned pregnancies compared with smaller quantities (three or one-month supplies).15 A US study by Foster et al, which included 84,401 women, reported that dispensing multiple packets of COCP at once also increased adherence rates. The study which compared rates for women who received a one-year, three-month or one-month supply of oral contraceptive pills, found that dispensing a one-year supply decreased the odds of unplanned pregnancy by 30% and decreased the odds of having an abortion by 46%.15 The study concluded that supplying higher quantities of COCPs improves accessibility and in turn may reduce the incidence of unplanned pregnancy and abortion.15 The role of pharmacists in improving adherence One problem associated with COCP use is discontinuation of treatment and therefore careful counselling prior to commencement is an important aspect of improving adherence.16 Women are often concerned with irregular or break-through bleeding in the initial few months and some may be concerned that this implies a lack of contraceptive effect.16 It is important to reassure women that this is common in the first few months and does not indicate reduced contraceptive cover. Moreover the irregular bleeding usually diminishes over time.16 Page 9 of 29 © Copyright 2014 This version of the program is unaccredited and intended for informational purposes only. An accredited version is available online at www.mdbriefcase.com.au
Many women taking COCPs may develop tolerance to some adverse effects within the first three months of use.17 Certain initial and common side-effects, such as nausea, may be relieved by taking the COCP at night. Taking the time to counsel women when dispensing repeat prescriptions is important as it provides an opportunity for monitoring and enables the pharmacist to offer encouragement and dispel any misconceptions regarding COCP use.16 Potential for medication interactions It is important to note that the prescribing information for some COCPs states the following precaution regarding interactions with antibiotics: “Some clinical reports suggest that enterohepatic circulation of oestrogens may decrease when certain antibiotic agents are given, which may reduce ethinyloestradiol concentrations (e.g. penicillins, tetracyclines). Women prescribed antibiotics (except rifampicin or griseofulvin) should use a barrier method until 7 days after completing a course of antibiotics. During the period in which the barrier method is used, tablet-taking should not be interrupted by a tablet-free interval.”3 Pregnancies have been reported following concomitant use of COCs and a wide range of antimicrobial agents, including penicillins, tetracyclines, macrolides, fluoroquinolones and imidazole antifungal drugs. The main hypothesis that has been used to explain contraceptive failures in antibiotic users is that broad-spectrum antibiotics temporarily reduce colonic bacteria, which may in turn reduce the enterohepatic recycling of ethinyloestradiol. However there is no evidence to prove such interactions.18 There has, however, been a recent shift in evidence regarding the concomitant use of COCPs and antibiotics. Current guidelines no longer advise the need for additional precautions when using COCPs with antibiotics that are not enzyme inducers. Rifampicin-like medications are particularly potent enzyme inducers and may reduce serum levels of ethinyloestradiol.6 For the most recent information on use of COCs and antibiotics, please see the following online resources:
NPS MedicineWise: Will antibiotics affect my contraceptive? (http://www.nps.org.au/media-centre/mediareleases/repository/Will-antibiotics-affect-my-contraceptive)
Royal College of Obstetrics and Gynaecology, faculty of sexual and reproductive health: drug interactions with hormonal contraception (http://www.fsrh.org/pdfs/CEUguidancedruginteractionshormonal.pdf)
Horn JR, Hansten PD. Antibiotics and Oral Contraceptive Failure. Pharmacy Times November 2003:64-65. (http://www.hanstenandhorn.com/hh-article11-03.pdf) Page 10 of 29
© Copyright 2014 This version of the program is unaccredited and intended for informational purposes only. An accredited version is available online at www.mdbriefcase.com.au
If patients have any further questions regarding concomitant use of antibiotics and the COCP, please refer them back to their doctor. Tip for pharmacists: When counselling patients regarding side effects such as breakthrough bleeding, it is important to identify whether this may be attributed to missed pills, diarrhoea, vomiting or drug interactions. In cases where missed pills may be problematic, try to encourage good adherence by taking the pills at the same time each day, for example at bedtime or with breakfast. By linking pill taking with the daily routine, adherence may be improved.
Test yourself question: Interactions between COCPs and other medications may lead to breakthrough bleeding and/or contraceptive failure. What are some of the medications that can interact with COCPs?
Tip for pharmacists: The National Prescribing Service has a helpful resource called Will antibiotics affect my contraceptive? Consider referring patients to this website as part of your comprehensive patient education program. It is available at: http://www.nps.org.au/medicines/infections-and-infestations/antibioticmedicines/antibiotics-for-respiratory-tract-infections/for-individuals/how-do-i-take-my-antibiotics/antibiotics-andcontraceptives Facilitating adherence through a digital dispensing device17
Adapted from The ClykTM dispenser: instructions for use. Bayer Australia Ltd. 2012. Page 11 of 29 © Copyright 2014 This version of the program is unaccredited and intended for informational purposes only. An accredited version is available online at www.mdbriefcase.com.au
A digital dispensing device can help women manage their YAZ® Flex pills with a visual and audible reminder of where they are in their cycle, and helps monitor and guide the management of missed pills. The dispenser is designed to hold cartridges of YAZ® Flex pills which are released as a single pill when dispensed. The device helps women manage their YAZ® Flex pills by:17
Keeping track of time using a clock-like ring of 24 hollow tiles
Providing a visual and an audible reminder to take their pill (the audible alarm is optional)
Reminding women when they are late in taking their pill by counting hours since the missed dose
Displaying how many pills the woman is required to take in the event of missed pills
Indicating when additional contraception is needed (with initial commencement of pills or when pills are missed)
Displaying the current day of the cycle and when women may (or must) commence a 4-day PFI
Indicating when five or fewer pills remain in the cartridge and it requires replacement
Page 12 of 29 © Copyright 2014 This version of the program is unaccredited and intended for informational purposes only. An accredited version is available online at www.mdbriefcase.com.au
Case 1: Jacinta Case presentation Jacinta, a 29-year-old lawyer, presents at your city pharmacy at lunchtime with a script for a COCP with a digital tablet dispenser (ethinyloestradiol (as betadex clathrate) and drospirenone - YAZ® Flex). You ask Jacinta several questions such as whether she is currently taking a contraceptive pill and if she has ever taken one before? Jacinta replies that she has never used a COCP and has been using condoms until now for contraception. She explains that she is engaged to be married and would like to commence a COCP. Counselling women on the use of YAZ® Flex® with the ClykTM dispensing device The YAZ® Flex extended regimen is designed to be used in conjunction with the ClykTM digital dispensing device. The flexible regimen allows women to choose to have their withdrawal bleed anytime between days 25120 of the regimen. As demonstrated in figure 1, the flexible regimen consists of two phases:3, 17 1. Fixed phase where one pill is taken every day for 24 days 2. Flexible phase where women may continue taking daily pills for up to 120 days and can choose to take a 4-day PFI during days 25-120 to start a new cycle. Withdrawal bleeding usually occurs during the 4-day pillfree break Figure 1: Two phases of the YAZ® Flex extended regimen.3
Adapted from approved product information: YAZ® Flex Bayer. 2013.
Page 13 of 29 © Copyright 2014 This version of the program is unaccredited and intended for informational purposes only. An accredited version is available online at www.mdbriefcase.com.au
Did you know? Women should be advised to commence a 4-day pill-free break if they experience three or more consecutive days of breakthrough bleeding or spotting. This may reduce the total number of days of bleeding.3 Case continuation Jacinta tells you that her doctor mentioned that YAZ® Flex will enable her to delay her period until after her honeymoon, but she is unclear on the details of how to take the pill to ensure this happens. She asks you to review how to use the dispensing device and how to take the pill to delay her period. Activating the ClykTM digital dispensing device To activate the ClykTM dispenser for the first time, women should be counselled to follow these steps:17 1. Only open and insert the YAZ® Flex cartridge on the day of starting. 2. Remove the ClykTM dispenser from its package. 3. Hold the dispenser in the palm of the hand so the viewing window for pills may be seen. 4. Insert the cartridge in the dispenser, pushing it all the way in. The pills are now visible through the viewing window. 5. Turn the dispenser over to view the display screen on the front. The screen should now indicate the ClykTM dispenser is on and ready to use. 6. When ready to take the first pill, hold the ClykTM dispenser upright, then squeeze both soft sides at the same time with one hand, to release a pill into the other hand. The dispenser will track the cycle according to this first pill release (Figure 2). 7. Take the next (second) pill 24 hours later, at the reference time. At this time, the countdown will reach the arrow at the top of the screen, the reminder symbol will flash and a beep will be heard if the reminder sound is activated. Figure 2: Activating the ClykTM digital dispensing device.17
Adapted from the ClykTM dispenser: instructions for use. Bayer Australia Ltd. 2012. Page 14 of 29 © Copyright 2014 This version of the program is unaccredited and intended for informational purposes only. An accredited version is available online at www.mdbriefcase.com.au
Did you know? Releasing the first pill sets the Reference Time for the ClykTM dispenser to remind the woman to take her pill. For this reason, it is important for the woman to set her ‘reference time’ to a convenient time for her to take her pill. If the dispenser is activated and a pill is not dispensed within 48 hours, the dispenser switches to ‘inactive mode’ and all pills must be discarded before the dispenser can be reactivated by inserting a new cartridge.17 Using the ClykTM digital dispensing device A normal day using the ClykTM digital dispensing device is demonstrated in figure 3. Note that hollow tiles indicate a pill has been taken and the number of hollow tiles indicates the number of hours remaining until the next pill should be taken.17 Figure 3: A normal day using the ClykTM digital dispensing device.17
Adapted from the ClykTM dispenser: instructions for use. Bayer Australia Ltd. 2012.
Browsing through the menu on the digital dispensing device allows women to quickly view when their next scheduled pill should be taken, where they are in their cycle, how many pills remain in the cartridge and when their next period may be scheduled. Figure 4 illustrates how this would appear.17
Page 15 of 29 © Copyright 2014 This version of the program is unaccredited and intended for informational purposes only. An accredited version is available online at www.mdbriefcase.com.au
Figure 4: Browsing through the menu, an example of day 10.17
Adapted from the ClykTM dispenser: instructions for use. Bayer Australia Ltd. 2012.
The digital dispensing device can help women schedule a 4-day PFI and will indicate whether a PFI is appropriate.17 Figure 5 demonstrates how this would appear on the ClykTM dispensing device.
Page 16 of 29 © Copyright 2014 This version of the program is unaccredited and intended for informational purposes only. An accredited version is available online at www.mdbriefcase.com.au
Figure 5: Scheduling a 4-day pill-free interval.17
Adapted from the ClykTM dispenser: instructions for use. Bayer Australia Ltd. 2012.
Forum question Jacinta admits that she is worried that ‘skipping her period’ is unhealthy. How would you counsel Jacinta?
Case conclusion You review the benefits of YAZ® Flex with Jacinta as being reliable contraception with the ability to delay monthly periods for up to four months. You also discuss its limitations which include the need to strictly adhere to daily on-time administration, with a scheduled withdrawal bleed starting on day 25-120 of the cycle. Jacinta is pleased with the added flexibility of determining the timing of her period, but asks you to again review how to set up and use the digital tablet dispenser. She asks if you can demonstrate with the first pill, and you counsel her on the intrinsic features of the device, which include the fact that the pills are scheduled to be taken at the same time each day, and if she initiated the cycle at lunchtime, the alarm will sound at the same time each day. You recommend that she carefully considers the time of day that best suits her for daily administration, and suggest that she start on waking or at bedtime. Once the ClykTM dispensing device is activated she must start using it Page 17 of 29 © Copyright 2014 This version of the program is unaccredited and intended for informational purposes only. An accredited version is available online at www.mdbriefcase.com.au
within two days. You describe the process of loading the cartridge and that this automatically activates the timer. You direct her to the www.myperiods.com.au/clyk web site for further patient information. Forum question What other sexual health or contraceptive advice do you offer women when commencing a COCP?
Page 18 of 29 © Copyright 2014 This version of the program is unaccredited and intended for informational purposes only. An accredited version is available online at www.mdbriefcase.com.au
Case 2: Rachel Case presentation Rachel is 18 years old and presents with a repeat prescription for her oral contraceptive script. Rachel explains that although she is generally pleased with her COCP (as she has noticed her acne has improved since commencing the pill), she tends to forget taking it and is concerned about pregnancy if she skips a dose or two. She is also planning to backpack overseas with her boyfriend for 6 months. You outline some of Rachel’s other options (including a vaginal ring, hormonal intra-uterine device, an implant and an OC with a digital dispensing device) and recommend that she speaks with her doctor for a contraceptive that will give her more peace of mind. Case continuation Rachel returns after a week with a prescription for a COCP with a digital dispensing device. Rachel’s doctor recommended sticking with the hormonal preparations that had proven helpful with her acne, and Rachel liked the idea of being in control in determining when she was going to get her period. Rachel also likes the idea of being reminded when she misses a tablet and being prompted on the appropriate course of action. Managing missed pills Counselling women on how to manage missed COCP pills is an important aspect of ensuring the correct use of the COCP. As demonstrated below, the extended regimen associated with YAZ® Flex and the ClykTM dispensing device requires different counselling points compared to other COCPs. Missed pills when taking YAZ® Flex3 YAZ® Flex can only be used in combination with the dedicated Clyk™ tablet dispenser, designed to support the user in following the regimen.3 If the user is less than 24 hours late in taking a YAZ® Flex tablet, contraceptive protection is not reduced. The woman should take the YAZ® Flex tablet as soon as she remembers and continue to take the tablets at the usual time. If the user is more than 24 hours late in taking a YAZ® Flex tablet, contraceptive protection may be reduced. The management of missed tablets can be guided by the following two basic rules: 1. The recommended tablet-free interval is 4 days, tablet- taking must never be discontinued for longer than 7 days. 2. Seven days of uninterrupted tablet-taking are required to attain adequate suppression of the hypothalamic-pituitary-ovarian-axis Page 19 of 29 © Copyright 2014 This version of the program is unaccredited and intended for informational purposes only. An accredited version is available online at www.mdbriefcase.com.au
In case of severe gastro-intestinal disturbances, absorption may not be complete and additional contraceptive measures should be taken.3 If vomiting occurs within 3-4 hours after taking, absorption may not be complete. In such an event, the advice concerning missed tablets is applicable.3 If the woman does not want to change her normal tablet-taking schedule, she has to take the extra tablet(s) from the tablet dispenser.3 In the event of a missed pill, the digital dispensing device will automatically alert and guide women towards the appropriate action.17 Figure 6 illustrates how the dispensing device will appear when a pill is forgotten. Figure 6: Managing forgotten pills through the digital dispensing device.17
Adapted from the ClykTM dispenser: instructions for use. Bayer Australia Ltd. 2012.
Forum question In your opinion, what are the benefits of the digital dispensing device? Case conclusion You take the time to counsel Rachel on how to activate her device and start taking her pill. You also explain the main features and benefits of the device. Rachel agrees that this new dispensing system would help her remember to take the pills and you advise she commences a trial prior to travelling overseas. Rachel asks if you think she can delay her period for the entire six-month duration of her trip, and you counsel against this, reinforcing the fact that the product may be used continuously for up to 120 days. She will have a minimum of one withdrawal bleed through her 6-month trip and she is able to determine when to take a break within the designated time for her period. Page 20 of 29 © Copyright 2014 This version of the program is unaccredited and intended for informational purposes only. An accredited version is available online at www.mdbriefcase.com.au
Forum question In your opinion, what are the most important counselling points when discussing the digital dispensing device?
Key messages
Today’s women appreciate the option of a more convenient lifestyle without the need for a monthly withdrawal bleed.10
Extended use of COCPs may help women with regard to flexibility in dosing and bleeding less frequently.6
Rates of contraceptive efficacy are similar in both the continuous and cyclic COCP regimens.6
Forming a time-related habit may be a key to better adherence to oral contraceptives.14
A digital dispensing device can assist women manage their COCP use by visually reminding women when to take their pill, where they are in their cycle, and helping the management of missed pills.3, 17
The YAZ® Flex extended regimen consists of a fixed phase for 24 days which is then followed by a flexible phase. This allows women to continue taking daily pills for up to 120 days and choose to take a 4-day pill-free break during days 25-120.3, 17
Practice tips
Pharmacists can advise that many common adverse effects associated with COCPs such as headache, pelvic pain, breast tenderness, bloating and swelling may occur more commonly during the PFI and may in some cases be reduced with the use of extended COCPs.7
It is important to reassure women that although breakthrough bleeding commonly occurs in the first few months of extended COCP use, it usually decreases with each subsequent cycle and is comparable to rates seen in traditional 21/7 day cycles by the fourth extended cycle.4
Contraindications to consider when commencing COCPs include:3 o Presence or history of venous or arterial thrombotic events o Presence or history of prodromi of a thrombosis o History of migraine with focal neurological symptoms o Diabetes mellitus with vascular involvement o Presence of a severe or multiple risk factor(s) for venous or arterial thrombosis may also constitute a contraindication Page 21 of 29
© Copyright 2014 This version of the program is unaccredited and intended for informational purposes only. An accredited version is available online at www.mdbriefcase.com.au
o Pancreatitis or a history thereof if associated with severe hypertriglyceridemia o Severe hepatic disease as long as liver function values have not returned to normal o Severe renal insufficiency or acute renal failure o Presence or history of liver tumours (benign or malignant) o Known or suspected sex-steroid influenced malignancies o Undiagnosed vaginal bleeding o Hypersensitivity to any of the ingredients contained in the COCP. o Known or suspected pregnancy
When dispensing emergency contraception, it is important to recall that poor adherence to oral contraception is reported to be one of the reasons for seeking emergency contraception.14
Taking the time to counsel women when dispensing repeat prescriptions is important, as it provides an opportunity for monitoring and enables the pharmacist to offer encouragement and dispel any common misconceptions regarding COCP use.
Dispensing larger quantities of oral contraceptives may improve adherence rates. 15
Women on the extended COCP regimens should be advised to commence a 4-day pill-free break if they experience three or more consecutive days of breakthrough bleeding or spotting. 3
In the event of a missed pill, the Clyk™ digital dispensing device will automatically alert and guide women towards the appropriate action.17
It is important to set the Clyk™ Reference Time at a convenient time for the woman to take her pill. If the dispenser is activated and a pill is not dispensed within 48 hours, the dispenser switches to ‘inactive mode’ and all pills must be discarded before the dispenser can be reactivated by inserting a new cartridge.17
Page 22 of 29 © Copyright 2014 This version of the program is unaccredited and intended for informational purposes only. An accredited version is available online at www.mdbriefcase.com.au
Post-test Multiple-choice questions 1. Which of the following is the most commonly-used contraceptive method in the developed world? a. Condoms b. Oral contraceptive pills c. Intrauterine devices d. Vaginal rings 2. What are the benefits of COCP use? a. Decreased risk of breast, lung, ovarian and endometrial cancer b. Decreased risk of myocardial infarction and hypertension c. Decreased risk of osteoporosis d. Decreased risk of diabetes and metabolic disease 3. Which of the following statement is correct? a. Dispensing a one-month supply of COCP is the most effective method of improving adherence. b. Developing a time-related habit with regard to taking oral contraception at the same time every day has no effect on rates of adherence and contraceptive efficacy. c. Dispensing larger quantities of COCPs does not help improve adherence rates. d. Poor adherence to oral contraception is reported to be one of the reasons for seeking emergency contraception. 4. Which of the following are some of the contraindications to COCPs? a. Dry eye, hot flushes, vaginitis b. History of venous thromboembolism, stroke, ischaemic heart disease, breast cancer or liver disease c. Headache, insomnia, anaemia d. History of urinary tract infections, hypertension,
Page 23 of 29 © Copyright 2014 This version of the program is unaccredited and intended for informational purposes only. An accredited version is available online at www.mdbriefcase.com.au
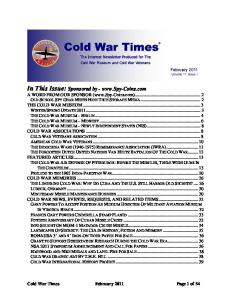
5. The Clyk™ dispensing device allows women to choose a pill-free break within which phase of the YAZ® Flex regimen? a. Days 1-24 (fixed phase) b. Days 25-120 (flexible phase) c. Days 25-365 d. Days 121-365 6. What does this image from the Clyk™ dispensing device indicate?
a. The audible alarm is on. The pill has been taken and the 22 hollow tiles indicates there are 22 hours before the next pill needs to be taken b. The pill has been missed and the 22 hollow tiles indicates that 22 hours have passed since the scheduled pill should have been taken c. The 22 hollow tiles indicates that 22 days have passed since the last pill was taken d. The 22 hollow tiles indicate there are 22 pills remaining in the cartridge 7. Once the Clyk™ dispensing device has been activated, a pill must be released within: a. 24 hours b. 48 hours c. One week d. One month Answer: B If the woman activates the dispenser and doesn’t use a pill within 48 hours, the dispenser switches to ‘inactive mode’ and all pills must be discarded before re-activation of the dispenser with a new cartridge.17
Page 24 of 29 © Copyright 2014 This version of the program is unaccredited and intended for informational purposes only. An accredited version is available online at www.mdbriefcase.com.au
8. Karen is a 29-year-old patient who missed her YAZ® Flex pill on day 97 of her cycle. What would you recommend? a. Provided that only one pill has been missed and the previous seven days have been taken correctly, no additional contraception is required. b. One option is to take the missed pill as soon as she remembers even if that means taking two pills at the same time and then continue to take the pills until she has taken at least 7 consecutive pills without interruption. c. One option is to decide to have a pill-free interval of 4 days, which includes the days missed, in order to induce a withdrawal bleed and subsequently commence a new cycle. d. All of the above. 9. Anna, a 32-year-old mother of two children, presents to your pharmacy as she is currently taking YAZ® Flex and has had breakthrough bleeding for the last 3 days. She is currently on day 44 of her cycle and this is her second cycle with the extended COCP. What would you advise her? a. Don’t worry about it, breakthrough bleeding is normal and has no effect on contraceptive efficacy. There is not much she can do about the breakthrough bleeding and it will eventually stop. b. Commence a 4 day pill-free interval to induce menstruation and commence a new cycle. c. Don’t worry about the breakthrough bleeding, it does not have any effect on contraceptive efficacy however if it doesn’t stop after 4 weeks then commence a 4 day pill-free interval. d. Cease YAZ® Flex and trial a new COCP.
Page 25 of 29 © Copyright 2014 This version of the program is unaccredited and intended for informational purposes only. An accredited version is available online at www.mdbriefcase.com.au
Resource centre Guidelines and recommendations Contraception: an Australian clinical practice handbook 3rd ed. 2012. Produced and published by Family Planning New South Wales (FPNSW), Family Planning Queensland (FPQ) and Family Planning Victoria (FPV). Articles Family planning 2011: better use of existing methods, new strategies and more informed choices for female contraception. Hum Reprod Update. 2012;18(6):670-81. Hee L, Kettner LO, Vejtorp M. Continuous use of oral contraceptives: an overview of effects and side-effects. Acta Obstet Gynecol Scand. 2013;92(2):125-36. Edelman A, Gallo MF, Nichols MD, Jensen JT, Schulz KF, Grimes DA. Continuous versus cyclic use of combined oral contraceptives for contraception: systematic Cochrane review of randomized controlled trials. Hum Reprod. 2006;21(3):573-8. Hicks CW, Rome ES. Menstrual manipulation: options for suppressing the cycle. Cleve Clin J Med. 2010;77(7):445-53. Mazza D, Harrison C, Taft A, Brijnath B, Britt H, Hobbs M, et al. Current contraceptive management in Australian general practice: an analysis of BEACH data. Med J Aust. 2012;197(2):110-4. Molloy GJ, Graham H, McGuinness H. Adherence to the oral contraceptive pill: a cross-sectional survey of modifiable behavioural determinants. BMC Public Health. 2012;12:838. Foster DG, Hulett D, Bradsberry M, Darney P, Policar M. Number of oral contraceptive pill packages dispensed and subsequent unintended pregnancies. Obstet Gynecol. 2011;117(3):566-72.
Page 26 of 29 © Copyright 2014 This version of the program is unaccredited and intended for informational purposes only. An accredited version is available online at www.mdbriefcase.com.au
MD Briefcase Post-Course Survey 1. Please indicate the extent to which you agree or disagree with the following statements by using a scale of 0 to 10 where 0 =strongly disagree and 10=strongly agree
Statements
Strongly disagree.........Strongly agree
01 2
3
4
5
6
7
8
9
10
1. Younger women want an oral contraceptive pill that offers flexibility in dosing and longer cycles with minimum bleeding and adverse effects. 2. Oral contraceptive regimens with a pill free interval of 7 days are healthier as they mimic the natural menstrual cycle. 3. I am proficient in addressing the concerns of younger patients regarding the extended and long-term use of oral contraceptives. 4. I can confidently demonstrate and counsel patients on the use of the new digital dispensing device. 5. I can confidently counsel patients on the importance of adherence to oral contraceptives.
Page 27 of 29 © Copyright 2014 This version of the program is unaccredited and intended for informational purposes only. An accredited version is available online at www.mdbriefcase.com.au
Page 28 of 29 © Copyright 2014 This version of the program is unaccredited and intended for informational purposes only. An accredited version is available online at www.mdbriefcase.com.au
References 1. 2. 3. 4. 5. 6. 7. 8. 9. 10. 11. 12. 13. 14. 15. 16. 17. 18.
Family planning 2011: better use of existing methods, new strategies and more informed choices for female contraception. Hum Reprod Update. 2012;18(6):670-81. Mazza D, Harrison C, Taft A, Brijnath B, Britt H, Hobbs M, et al. Current contraceptive management in Australian general practice: an analysis of BEACH data. Med J Aust. 2012;197(2):110-4. Approved product information: Yaz Flex Bayer. 2012. Hicks CW, Rome ES. Menstrual manipulation: options for suppressing the cycle. Cleve Clin J Med. 2010;77(7):445-53. Greig AJ, Palmer MA, Chepulis LM. Hormonal contraceptive practices in young Australian women (