European Heart Journal (2004) 25, 1845–1852
Clinical research
Picotamide, a combined inhibitor of thromboxane A2 synthase and receptor, reduces 2-ye...
Picotamide, a combined inhibitor of thromboxane A2 synthase and receptor, reduces 2-year mortality in diabetics with peripheral arterial disease: the DAVID study Gian Gastone Neri Serneria, Sergio Coccherib,*, Ettore Marubinic, Francesco Violid, for the Committees and the Investigators of the Drug Evaluation in Atherosclerotic Vascular Disease in Diabetics (DAVID) Study Group a
University University c University d University b
of Florence, Italy of Bologna, Italy: Hospital St. Orsola, Paol. 24 40138, Bologna of Milan, Italy ‘‘La Sapienza’’, Rome, Italy
Received 19 February 2004; revised 10 June 2004; accepted 1 July 2004 Available online 24 August 2004
See page 1769 for the editorial comment on this article (doi:10.1016/j.ehj.2004.08.008)
KEYWORDS
Aims Patients with diabetes are at excessive risk of mortality and cardiovascular morbidity. Previous studies suggest that aspirin may be less effective in diabetic patients. In this multi-centre, randomized, double blind trial picotamide, a dual inhibitor of thromboxane A2 synthase and receptor, was compared with aspirin for the prevention of mortality and major cardiovascular events in diabetics with peripheral arterial disease (PAD). Methods and results A total of 1209 adults aged 40–75 years with type 2 diabetes and PAD were randomized to receive picotamide (600 mg bid) or aspirin (320 mg od) for 24 months. The cumulative incidence of the 2 years overall mortality was significantly lower amongst patients who received picotamide (3.0%) than in those who received aspirin (5.5%) with a relative risk ratio for picotamide versus aspirin of 0.55 (95% CI: 0.31–0.98%). Events were reported in 43 patients (7.1%) on picotamide and 53 (8.7%) on aspirin. The combined endpoint of mortality and morbidity had a slightly lower incidence in the picotamide group but this difference did not reach statistical significance. Conclusion Picotamide is significantly more effective than aspirin in reducing overall mortality in type 2 diabetic patients with associated PAD. c 2004 The European Society of Cardiology. Published by Elsevier Ltd. All rights reserved.
0195-668X/$ - see front matter c 2004 The European Society of Cardiology. Published by Elsevier Ltd. All rights reserved. doi:10.1016/j.ehj.2004.07.013
1846
Introduction An excessive mortality and morbidity rate, particularly as a result of cardiovascular complications, has been reported in patients with both types of diabetes mellitus. This was originally shown in prospective studies conducted in the 1970s and 1980s,1,2 and has been confirmed more recently.3,4 Numerous studies and two large metaanalyses of randomized trials have shown that aspirin is effective in preventing vascular events, including non-fatal myocardial infarction, non-fatal stroke, and death from vascular causes in patients with a variety of vascular conditions.5,6 However, the efficacy of aspirin and other antiplatelet agents is suggested to be low in diabetic patients. In a recent meta-analysis,6 the odds reduction of major vascular events with antiplatelet drugs in the diabetic subgroups with or without previous vascular events was only 7%, and did not achieve statistical significance. Regarding peripheral arterial disease (PAD), the use of aspirin is recommended by the American College of Chest Physicians;7 however, a Food and Drug Administration expert panel found insufficient evidence to approve labelling of aspirin as indicated for patients with PAD.8 It is clear therefore, that new drugs may be needed for better protection from death and morbidity in diabetic patients, and particularly in those with PAD. Picotamide, a derivative of methoxy-isophtalic acid, is an antagonist of thromboxane A2/prostaglandin endoperoxide H2 (TXA2/PGH2) receptors, and also inhibits thromboxane A2 (TXA2) synthase at equivalent concentrations.9–12 This results in effective inhibition of TXA2mediated events. This dual action may have potentially enhanced therapeutic efficacy in the prevention of thrombosis, including inhibition of platelet aggregation and accumulation of antiaggregatory prostaglandins (PGI2 and PGD2).13 Hence, picotamide may be useful in diabetic patients, who have increased platelet activation and TXA2 synthesis.14 In a double blind, placebo-controlled study15 in 2313 patients with PAD, picotamide significantly reduced the relative risk of combined major and minor cardiovascular events by 23% compared to placebo. A post hoc subgroup analysis of 438 PAD patients with diabetes suggested a reduction of 45.2% of the risk of combined major and minor events in those treated with picotamide.16 The encouraging results in this subgroup prompted us to investigate the efficacy of picotamide versus aspirin in a specifically designed, double blind, randomized study in diabetics with PAD.
Methods Study design and organization The drug evaluation in atherosclerotic vascular disease in diabetics (DAVID) study was a multi-centre, randomized, double blind, parallel group trial. Prior to participation in the study, all patients provided written informed consent. The study was
G.G. Neri Serneri et al. performed in accordance with the Declaration of Helsinki and its Amendments, and the protocol was approved by the Institutional Review Board (IRB) at each centre before initiation. The study involved 86 clinical centres from various regions of Italy and followed US Investigational New Drug regulation and European Good Clinical Practice Guidelines as well as local requirements. The Steering Committee formed by five University-based scientists, had overall responsibility for the design, execution and reporting of the study. An independent external Safety and endpoint Validation Committee was responsible for validation of all clinical events occurring during enrolment and follow-up. At the end of the trial and before the statistical analysis, all the clinical events were reviewed and validated by the Steering and Safety Committees in joint meetings. The statistical analysis was performed by an independent statistical University centre in Milan. The study protocol was designed by the Steering Committee, which also surveyed all phases of the trial. Site monitoring and data collection were performed by a designated contract research organization.
Patients eligibility Patients of both sexes, between 40 and 75 years of age and with a history of type 2 diabetes for 5 years or more and PAD were eligible for inclusion in the study. PAD was defined as the presence of two or more of the following: (1) history of intermittent claudication lasting more than 2 months (WHO, leg pain on walking, disappearing in less than 10 min on standing); (2) loss of posterior tibial pulse in the foot; (3) ankle/arm pressure ratio 1.30 in the posterior or anterior tibial artery of the foot (measured by Doppler probe); (4) amputation or reconstructive surgery in patients with previous history of intermittent claudication; (5) angioplasty with no persisting complication from intervention. The exclusion criteria were: (1) myocardial infarction, stroke or unstangina in the 6 months prior to enrolment; (2) severe neurological or mental deficits likely to make the patient noncompliant; (3) severe co-morbidity likely to limit patient’s life expectancy to less than 2 years; (4) serum creatinine >2.0 mg/ dl; (5) high risk of endo-ocular bleeding; (6) alanine aminotransferase (ALT) or aspartate aminotransferase (AST) over three times the upper limit of normal (ULN); (7) platelets 20 min) chest pain; elevation of CK, CK-MB, LDH or AST to 2· upper limit of laboratory normal; typical ECG changes (development of new >40 ms Q waves in at least two adjacent leads or new dominant R wave in V1 or evolutionary ST-T changes). Ischaemic stroke was taken to be an acute neurological vascular event with focal signs for P24 h and a CT scan recognition of a proper ischaemic lesion, without evidence of intracranial haemorrhage. Amputation was defined as major if performed above the ankle and not because of trauma or cancer.
Picotamide, a combined inhibitor of thromboxane A2 synthase and receptor
Procedures After the screening phase, eligible patients were randomly allocated to one of two treatment groups to receive either one picotamide 600 mg tablet twice daily or one aspirin 320 mg tablet once daily in the morning plus one placebo tablet once daily in the evening and followed for 24 months. Blinding was maintained by the use of indistinguishable active drugs and placebo tablets in separate bottles labelled for morning and evening intake. The randomization list was performed stratified by centre with treatment in balanced blocks of four patients within each centre; a 1:1 treatment allocation was used. Study visits were scheduled at 4 month intervals (baseline, 4, 8, 12, 16, 20 and 24 months) after enrolment. Routine clinical and safety check-ups were performed at each visit and blood samples for haematological and biochemical assessments were taken for analysis at baseline and 12 and 24 months thereafter. Electrocardiograms (ECG) were performed according to normal practice at each centre. At each study visit, compliance was assessed by counting the tablets returned by the patient. Concomitant medications were monitored by questioning patients at each visit. No concomitant medications that affected platelet function or blood coagulation were permitted during the 24 month study period. Adverse events were monitored throughout the trial.
Statistical analysis The sample size of the trial was calculated to show a difference between treatments in 2 year overall mortality based on published mortality and risk reduction data. It has been reported that 2-year mortality in patients with type 2 diabetes mellitus is 8.4%.17 Considering a 23–25% risk reduction due to treatment with aspirin, as reported by the Antiplatelet Trialist’s (APT) Collaboration5 and more recently by the Antithrombotic Trialist’s (ATT) Collaboration,6 a 2-year overall mortality rate of 6.3– 6.5% could be predicted for the aspirin group. Assuming a 2-year mortality rate of 6.5% in the aspirin group of our study, we surmised that an absolute reduction of mortality under picotamide of 3.5% in 2 years, equivalent to little more than 1.5% per year, could offer acceptable clinical relevance and allow for a reasonable number of the study population. In fact, we calculated that 584 patients per group were required to detect this difference, with a power of 80% and a significance level set at 0.05 (twosided). We therefore aimed at recruiting a target sample size of 1200 patients (600 patients per group). As regards overall 2-year mortality, time from randomization to the date of death for any cause was considered the response; for survivors the length of observation was censored at the date of the last follow-up visit. Comparison of mortality between the two arms was carried out by the log-rank test. The Kaplan–Meier method was used to estimate survival probabilities; their complement to one is the cumulative incidence of mortality and was used to draw the pertinent curves of mortality for the length of time to death. As regards the combined endpoint, time from randomization to the date of the first event, regardless of its nature, was considered the response; for patients withdrawn alive without events, time of observation was censored at the date of the last follow-up visit (after some 24 months). As the censoring of patients lost to follow-up could be informative, loss to follow-up was considered to be a competing risk cause for the combined endpoint. Therefore the comparison between treatment groups was accomplished using Gray’s test;18 coherently the crude cumulative incidence19 curves were drawn to depict the pattern for the length of time to first event, whichever its nature, in the combined endpoint.
1847
To describe the occurrence of each event, the cumulative incidence was computed. The comparison of frequency of gastrointestinal discomfort between treatments was analysed with the v2 test. The statistical analyses were performed on all randomized patients following the intention-to-treat approach and all the tests were two-sided.
Results Study population A total of 1209 patients at 86 centres were enrolled in the study between February 1996 and October 1998. Of these, 603 patients were randomly allocated to receive picotamide and 606 to receive aspirin (Fig. 1). The median duration of the follow-up was 2 years (interquartile range 1.9–2.1). During the study, 32 patients (5.3%) in the picotamide group and 26 (4.3%) in the aspirin group were lost to follow-up and therefore had no endpoint data. In total, 319 patients (26.4%) prematurely discontinued study drugs. Of these, 159 (26.4%) patients were in the picotamide group and 160 (26.4%) in the aspirin group. The reasons for premature withdrawal from the study were similar in the two groups. Adverse events were the most common reason for discontinuation (11.9% and 14.4% in the picotamide and aspirin groups, respectively) followed by withdrawal of consent (10.1% and 8.6%), taking contraindicated medications (1.5% and 1.3%), non-compliance (1.2% and 0.8%) and other reasons (1.7% and 1.3%).
Demographics and baseline characteristics The treatment groups were well-matched with respect to sex, age, BMI, mean values of blood pressure (systolic and diastolic), heart rate, cardiovascular risk factors (smoking, hypertension, hyperlipidaemia) and previous stroke or coronary heart disease. Diabetes treatment and other cardiovascular therapies were also distributed similarly between the two groups (Table 1).
Endpoints and related observations Overall mortality Mortality data were available for 571 (94.7%) and 580 (95.7%) patients in the picotamide and aspirin group, respectively.
Randomized n = 1209
Assigned picotamide n = 603 (49.9%)
Assigned aspirin n = 606 (50.1%) Lost to follow-up n = 26 (4.3%)
Lost to follow-up n = 32 (5.3%) Completed trial n = 571 (94.7%)
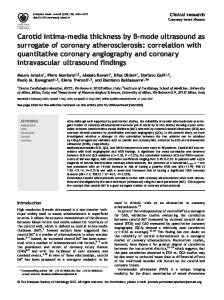
Causes of death according to treatment group are given in Table 2. The cumulative incidence of the two years overall mortality in the two groups is given in Fig. 2 and the results of the pertinent log-rank test is v2 = 3.9299 (p = 0.0474).
No. at risk Picotamide Aspirin
603 606
594 596
Log rank test: χ2 = 3.9299
577 583
561 575
553 562
540 546
490 496
p = 0.0474
Fig. 2 Kaplan–Meier analysis of the time-to-death according to treatment assignment.
Overall mortality, the predefined primary endpoint, was significantly lower amongst patients who received picotamide (3.0%) than in those who received aspirin (5.5%). The relative risk of death in the picotamide group compared to the aspirin group was 0.55 (95% CI: 0.31– 0.98%). Mortality and morbidity Morbidity data were available for 491 (80.4%) and 504 (83.2%) patients in the picotamide and aspirin group, respectively. Events were reported in 43 patients (7.1%) receiving picotamide and in 53 (8.7%) receiving aspirin (Table 3). Analysis of the predefined secondary endpoint of combined mortality and morbidity showed a slightly lower incidence in the picotamide group over the course of the study (Fig. 3). However, this difference did not reach statistical significance (Gray’s test z = 1.072, p = 0.300).
Table 2 Mortality according to treatment groups Picotamide (n = 603)
Picotamide, a combined inhibitor of thromboxane A2 synthase and receptor
1849
Table 3 Mortality and morbidity events by treatment groups Type of event
Picotamide (n = 603)
Aspirin (n = 606)
n
Cumulative incidence (%)
n
Cumulative incidence (%)
Myocardial infarction (fatal and non-fatal) Stroke (fatal and non-fatal) Amputation Other deaths
15 14 4 12
2.9 2.7 0.8 2.2
19 12 4 19
3.6 2.2 0.8 3.8
At least one event
43
53
of bleeding events leading to hospitalisation was 0.2% in the picotamide group (one hospitalisation) and 1.2% in the aspirin group (seven hospitalisations). One patient in the aspirin group died due to a haemorrhagic event, namely a cerebral haemorrhage. The frequency of gastrointestinal discomfort was significantly lower in the picotamide than in the aspirin group (10.9% versus 18.3%, respectively; p < 0.0001) (Table 4). The proportion of patients prematurely discontinuing study drug due to adverse events was comparable in both treatment groups [11.9% (72 patients) in the picotamide group versus 14.4% (87 patients) in the aspirin group].
Discussion Fig. 3 Crude cumulative incidence curves of first event for combined endpoint, considering lost to follow-up a competing risk.
Vascular and non-vascular mortality Vascular mortality alone was not a predefined endpoint, and involved a considerably lesser number of events than overall mortality (34 vascular out of 48 deaths) (Table 2). A reduction in vascular mortality consistent with that of total mortality was seen in the picotamide group, although it did not reach statistical significance (data not reported). The proportion of non-vascular over total deaths was similar in the two groups.
Safety Analysis of adverse events revealed no unusual findings in either treatment group. Bleeding events were reported in eight patients (1.3%) in the picotamide group and in 12 patients (2.0%) in the aspirin group. The frequency
In this double blind study picotamide, an inhibitor of thromboxane synthase and of platelet thromboxane and endoperoxide receptors, was compared with aspirin in patients with type 2 diabetes mellitus and PAD. The predefined primary endpoint of the study was overall mortality. Treatment with picotamide was associated with an almost halved 2-year mortality rate, with a relative risk of 0.55 versus aspirin, and was statistically significant. The secondary study endpoint, mortality plus non-fatal vascular events, was only slightly reduced under picotamide. The evaluation of this combined endpoint may have been partially flawed by the proportion of patients (around 20% in each group) lost to follow-up for non-fatal events. Being ‘‘lost to follow-up’’ was considered as a competing risk and the calculations were performed only on the ‘‘intention to treat’’ population. Thus, the number of non-fatal events recorded is likely to be underestimated, possibly affecting the outcome of this endpoint.
The efficacy of antiplatelet drugs (in particular, aspirin) in patients with type 2 diabetes, who are at high risk of vascular mortality and morbidity, is still a matter of debate.20 Although aspirin is generally considered effective in diabetic subjects, many of the results on which this belief is based originate from subgroup data of trials or meta-analyses including both diabetic and (mainly) non-diabetic patients, rather than from trials carried out in diabetics alone. More recently, in an analysis of the diabetic subgroup of a large study of primary prevention of cardiovascular events, aspirin was found non-effective on the composite endpoints of cardiovascular death, stroke and myocardial infarction.21 Although results from subgroup analyses should be considered with reservations, similar data had also been obtained in a large specific trial of patients with diabetes, the Early Treatment of Diabetic Retinopathy (ETDR) study, in which aspirin did not reduce the incidence of major cardiovascular events.22 While only few of the diabetic patients enrolled in the EDTR study had previously suffered major vascular events, those included in the present trial had type 2 diabetes plus associated PAD. In this regard it should be recalled that PAD, also independently of associated diabetes, carries an increased risk of major vascular events.23 In fact, in patients with PAD there is clear evidence of a systemic atherothrombotic state24 and the burden of cardiovascular risk is greatly increased.25 Patients with both PAD and diabetes appear to be even at a higher risk, regarding both limb deterioration and vascular morbidity and mortality.26 With regard to antiplatelet prophylaxis in overall PAD patients, in the 1994 APT meta-analysis5 the observed relative risk reduction (17.8%) was not statistically significant. If the results are recalculated by including only the trials using aspirin,21 the resulting relative risk reduction amounts to only 6.7%. It is true that in the more recent ATT meta-analysis,6 the specific subgroup with intermittent claudication showed a risk reduction of 19%, reaching statistical significance; however much of the additional evidence in respect to the previous metaanalysis came from the ADEP trial15 in which the study drug was precisely picotamide. On the other hand specific studies of antithrombotic prophylaxis in patients with both diabetes and PAD are scanty. The only prospective study to our knowledge27 investigated the efficacy of aspirin and dipyridamole in preventing disease progression and major vascular events in diabetic patients with critical limb ischaemia or recent amputation. Antiplatelet treatment had no effect on vascular death and subsequent amputation, and a slight, non-significant effect on the combined endpoint of stroke and TIA. The present trial was aimed at the evaluation of an antiplatelet drug, picotamide, which has a mechanism of action potentially advantageous versus that of aspirin, particularly in diabetic patients. A major feature of our study was to have chosen overall mortality as the primary endpoint. This was certainly a difficult challenge for the study drug, but ultimately proved rewarding, as it yielded unequivocal evidence of efficacy in favour of
G.G. Neri Serneri et al.
picotamide. It can be added that, considering the size of the benefit (13–15 %) of antiplatelet drugs on total mortality shown in the APT meta-analyses, and in the light of the recent debate on the efficacy of aspirin in preventing fatal events,28 it seems especially relevant that picotamide almost halved all-cause mortality in PAD patients with type 2 diabetes in comparison with aspirin. Moreover this result was achieved with a tolerability profile somewhat advantageous over that of aspirin, especially because of fewer bleeding events requiring hospitalisation and fewer cases of gastric discomfort. This study was clearly not designed to investigate the mechanisms by which picotamide is especially effective in preventing fatal events in diabetic patients with PAD. According to some studies,29,30 particularly high amounts of thromboxane and endoperoxides are produced in diabetics through the increased platelet turnover mechanisms alternative to the cyclo-oxygenase pathway,31,32 and an exceedingly high thromboxane production could be relevant in the pathogenesis of the more severe, and hence the fatal complications of diabetes. During the time elapsed from submission of this paper, it has been reported that platelets from type 2 diabetic patients frequently show reduced ex vivo response to aspirin33 and the clinical relevance of this finding has been commented upon in an editorial by one of us.34 The combined properties of picotamide to antagonize TxA2 receptors and inhibit TxA2 synthase9,11 may result in a more effective inhibition of TxA2-mediated effects. Moreover, picotamide is provided with other properties, which appear to confer additional advantages over aspirin. Aspirin remains in plasma in its active, acetylated form for only a few minutes and is unable to reach the extravascular spaces.35 Conversely, picotamide remains active in plasma for 8–10 h36 and easily diffuses from the plasma to the arterial wall.37 At this location, it binds to TXA2/PGH2 receptors on smooth muscle cells and may inhibit TXA2 locally formed by TXA2 synthase.38 In conclusion, the main message of this study is that picotamide, a dual inhibitor of thromboxane A2 synthase and thromboxane-endoperoxide receptor, is significantly more effective than aspirin in reducing overall mortality in type 2 diabetic patients with associated peripheral arterial disease. However, this was a survival study and a possible advantage of picotamide versus aspirin on vascular events could not be firmly established. Thus, further confirmatory studies with this agent seem worthwhile in the future.
Committees and investigators Steering Committee: G G Neri Serneri, S Coccheri, G Agrifoglio, P Rizzon, B Trimarco Safety and Validation Committee: M Cortellaro, F Violi, E Marubini (statistician) Writing Committee: G G Neri Serneri, S Coccheri, E Marubini, F Violi
Picotamide, a combined inhibitor of thromboxane A2 synthase and receptor Investigators: A Pezzarossa, A Guberti (Cattedra di Endocrinologia, Dipartimento di Medicina Interna e Scienze Metaboliche, Universita ` di Parma), M Messina, S Gamba (U O A Endocrinologia-Diabetologia, Ospedale Maria Vittoria, Torino), G Allochis, C Cusaro (U O A Malattie Metaboliche e Diabetologia, Ospedale Maggiore della Carita `, Novara), E Ansaldi, M Battezzati (U O A Malattie Metaboliche e Diabetologia, Ospedale SS Antonio e Biagio e C Arrigo, Alessandria), G Bargero, G Ghezzo (U O A Diabetologia, Ospedale Santo Spirito, Casale Monferrato), S Fontana, L Dimitri (U O Medicina B, Ospedale di Biella), L Cataldi, C Bordone (Servizio di Diabetologia, A O San Martino, Genova), D Bessarione, G Grillo (U O Medicina Interna Generale, A O S Martino, Genova), M Domanin, A Gotti (Istituto di Chirurgia Vascolare e Angiologia, Universita ` di Milano), G Pizzi, O Disoteo (Centro di Diabetologia e Malattie Metaboliche, Ospedale Niguarda Ca ` Granda, Milano), G Testori (U O Diabetologia, A O Fatebenefratelli, Milano), M Puttini, P R Barbano (S C Chirurgia Vascolare, Ospedale Niguarda Ca ` Granda, Milano), G Emanuelli, P Vigano ` (Modulo di Chirurgia Vascolare, A O San Gerardo, Monza), C Mazzi, G Morandi (Divisione di Endocrinologia e Medicina Costituzionale, Ospedale S Antonio Abate, Gallarate), U G Cereda, V Vinci (U O Medicina 2, Ospedale di Saronno), E Costantini Brancadoro, A M Socrate (Chirurgia Vascolare, Ospedale di Busto Arsizio), P Bossolo, A Vailati (Medicina Interna e Oncologia Medica, Policlinico San Matteo, Pavia), A Giustina, A Burattin (Sezione di Endocrinologia, Dipartimento di Scienze Mediche e Chirurgiche, Universita ` di Brescia), W Colosio (Divisione Medicina, A O Mellino Mellini, Chiari), G Pascal, F Saggiani (Struttura Complessa di Medicina Generale, Ospedale Carlo Poma, Mantova), E Bobbio Pallavicini, C Cazzalini (Divisione di Medicina, Ospedale Maggiore, Crema), A Ballini, G Maccagni (Divisione di Medicina Interna 2, Ospedali Riuniti, Treviglio), M Marchesi, C Tomasi (Divisione di Medicina Interna 1, Ospedale di Bolzano), R Mingardi, G Erle (U O Malattie Metaboliche, Ospedale di Vicenza), A Tiengo, S Vigili de Kreutzenberg (Cattedra Malattie del Metabolismo, Universita ` di Padova), D Fedele, G Bax (Servizio di Diabetologia, Dietetica e Nutrizione Clinica, Universita ` di Padova), N Simioni, S Donazzan (Servizio di Diabetologia, Presidio Ospedaliero di Cittadella), E Arosio, S De Marchi (Divisione di Riabilitazione Cardiovascolare, Universita ` di Verona), G Monesi, F Mollo (U O Malattie Metaboliche e Diabetologia, Ospedale di Rovigo), A Ceriello, A Russo (Cattedra di Medicina Interna, Universita ` di Udine), M Moretti (Centro Antidiabetico, Presidio Ospedaliero di Portogruaro), A M Cernigoi (Servizio di Diabetologia, Presidio Ospedaliero di Monfalcone), S Bottazzo, P Zanchi (Centro Prevenzione Aterosclerosi, Ospedale Umberto I, Mestre), A Bonanome, A Pagnan (Cattedra di Medicina Interna, Universita ` di Padova, sede di Castelfranco Veneto), A Megha (Day-Hospital Medico-Chirurgico, Colorno), D G Pierfranceschi (U O Diabetologia, Presidio Ospedaliero di Piacenza), T Curti, A Tedesco (Cattedra di Chirurgia Vascolare, Universita ` di Bologna), A De Fabritiis, L Martini (Cattedra e Divisione di Angiologia, Policlinico S Orsola-Malpighi, Bologna), G Scondotto (U O C Angiologia, Azienda USL Citta ` di Bologna, Bologna), G Coppi, R Marra (U O Chirurgia Vascolare, Modena), I Portioli, E Manicardi (Centro Diabete e Malattie Metaboliche, Medicina 2, A O Santa Maria Nuova, Reggio Emilia), L Poggesi, P A Modesti (Istituto di Clinica Medica e Cardiologia, Universita ` di Firenze), A Lagi, G Bandinelli (U O Medicina Interna, P O Santa Maria Nuova, Firenze), C Pratesi, R Pulli (Cattedra e Scuola di Specializzazione di Chirur-
1851
gia Vascolare, Universita ` di Firenze), G Sabbatini (Sezione di Diabetologia e Malattie Metaboliche, Azienda USL 9, Grosseto), F Galeone, A V Magiar (Servizio Autonomo di Diabetologia e Malattie Metaboliche, Azienda USL 3, Pescia), D Vanni, L Ricci (U O Medicina Interna I, Ospedale S Donato, Arezzo), F Santeusanio, S Bistoni (Dipartimento di Medicina Interna e Scienze Endocrine e Metaboliche, Universita ` di Perugia), U Senin, G Aisa (Sezione di Gerontologia e Geriatria, Dipartimento di Medicina Clinica e Sperimentale, Universita ` di Perugia), M Massi Benedetti, M Orsini Federici (Dipartimento di Medicina Interna, Scienze Endocrine e Metaboliche, Universita ` di Perugia), M Lunetta, A Chiavetta (Servizio di Diabetologia, A O Cannizzaro, Catania), M Belvedere, V Scafidi (Dipartimento di Medicina Clinica e delle Patologie Emergenti, Universita ` di Palermo), G Testa, A Mancini (Servizio di Diabetologia e Malattie Metaboliche, Ospedale S Camillo, Roma), G Pollari, V Tonelli (U O C Angiologia, Ospedale Sandro Pertini, Roma), V Coto, U Oliviero (III Divisione di Medicina Interna, Dipartimento di Medicina Clinica e Scienze Cardiovascolari, Universita ` Federico II, Napoli), R Izzo, L Guerrera (Centro per la Diagnosi e la Cura dell’Ipertensione Arteriosa, Universita ` Federico II, Napoli), G Bracale, M Porcellini (Cattedra di Chirurgia Vascolare, Universita ` Federico II, Napoli), R Carleo, A Gatti (U O C Malattie Metaboliche, Presidio Ospedaliero San Gennaro, Napoli), A Salucci, U Amelia (Servizio di Diabetologia ed Endocrinologia, Ospedale di Nocera Inferiore), V Prisco, R Greco (Centro di Angiologia Medica, Presidio Ospedaliero di Mercato San Severino), A M Terracciano, F Carlino, Centro Antidiabetico A I D, Caserta, N Alberti, A Longo (U O Chirurgia Vascolare, A O Bianchi-Melacrino-Morelli, Reggio Calabria), A Venezia, R Morea (U O Diabetologia e Malattie Metaboliche, Ospedale Madonna delle Grazie, Matera), B Cretella, L Senatore (Servizio Diabetologia e Malattie Metaboliche, Crotone); M Ciccone, P Caputo (Istituto di Malattie dell’Apparato Cardiovascolare, Universita ` di Bari), A Bellomo Damato, S Perrini (Istituto di Clinica Medica, Endocrinologia e Malattie Metaboliche, Universita ` di Bari), C Pellegrino, L Ferrozzi (U O Chirurgia Generale, Ospedali Riuniti di Foggia), G Sabella, M Grilli (Medicina Generale, Ospedale Casa Sollievo della Sofferenza, San Giovanni Rotondo), G Ignone, A D’Adamo (U O Cardiologia, A O Di Summa, Brindisi), M Nuzzo, G Formoso (U O Endocrinologia, A O Vito Fazzi, Lecce), S Novo, R Caruso (Cattedra Malattie dell’Apparato Cardiovascolare, Universita ` di Palermo), G Licata, S Paterna (Istituto di Clinica Medica, Universita ` di Palermo), G Bompiani, S Verga (Istituto di Clinica Medica, Universita ` di Palermo), S S Signorelli, L Di Pino (Dipartimento di Medicina Interna e Medicina Specialistica, Universita ` di Catania), R Giannarelli, A Coppelli (Dipartimento di Endocrinologia e Metabolismo, Universita ` di Pisa), A Saitta, M Bonaiuto (Dipartimento di Medicina Interna, Cattedra di Terapia Medica, Universita ` di Messina), G M Baule, A Manca (III Divisione Medicina e Servizio di Diabetologia e Malattie del Metabolismo, Presidio Ospedaliero di Sassari), R Seguro (Servizio di Diabetologia, A O Brotzu, Cagliari), L Vincis, P Melis (Centrio Diabetologico, Presidio Ospedaliero Sirai, Carbonia), G Bonfardeci, C Cimminiello (Patologia Vascolare e Trombotica, III Divisione Medica, Ospedale San Carlo Borromeo, Milano), A Di Carlo (Servizio di Diabetologia e Malattie Metaboliche, Presidio Ospedaliero di Lucca), G Chesi, M G Dieci (U O Medicina Interna, Castel San Giovanni); A Cardinale, L Tantalo (U O Cardiologia, Ospedale di Matera), C Allegra, I Schachter (Day Hospital Angiologia, A O San Giovanni-Addolorata, Roma) M Trignano, I Pisano
1852 (Istituto di Patologia Chirurgica, Universita ` di Sassari), S Pientini, R Carloni (U O Geriatria e Riattivazione, Universita ` di Firenze).
Acknowledgements N.B. Financial support to the study was provided by Novartis S.p.a., Milan, Italy, as payment of fees to an independent CRO in charge of monitoring. The authors declare they have no conflicts of interest.
References 1. Garcia ML, Mc Namara PM, Gordon T et al. Morbidity and mortality in diabetes in the Framingham population: sixteen year follow-up study. Diabetes 1974;23:105–11. 2. Panzram G. Mortality and survival in type 2 diabetes (non insulindependent diabetes). Diabetologia 1987;30:123–31. 3. Portuese E, Orchard T. Mortality in insulin-dependent diabetes. In: National Diabetes Data Group, editor. Diabetes in America. Bethesda (MD): National Institute of Health; 1995:233–55 (NIH Publication No. 95-1468). 4. Geiss LS, Herman WH, Smith PJ. Mortality in non-insulin-dependent diabetes. In: National Diabetes Data Group, editor. Diabetes in America. Bethesda (MD): National Institute of Health; 1995:233–55 (NIH Publication No. 95-1468). 5. Antiplatelet Trialist’s Collaboration. Collaborative overview of randomized trials of antiplatelet therapy. Prevention of death, myocardial infarction, and stroke by prolonged antiplatelet therapy in various categories of patients. BMJ 1994;308:81–106. 6. Antithrombotic Trialist’s Collaboration. Collaborative meta-analysis of randomized trials of antiplatelet therapy for prevention of death, myocardial infarction and stroke in high risk patients. BMJ 2002;324:71–86. 7. Jackson MR, Clagett GP. Antithrombotic therapy in peripheral arterial occlusive disease. Chest 1998;114:666S–82S. 8. Food and Drug Administration. Internal analgesic, antipyretic, and antirheumatic drug products for OTC human use: final rule for professional labeling of aspirin, buffered aspirin, and aspirin in combination with antacid drug products. Fed Regist 1998;63:56802–19. 9. Gresele P, Deckmyn H, Arnout J et al. Characterization of N,N0bis(3-pycolil)-4-methoxy-isophtalamide (picotamide) as a dual thromboxane synthase inhibitor/thromboxane A2 receptor antagonist in human platelets. Thromb Haemost 1989;61:479–84. 10. Modesti PA, Colella A, Abbate R et al. Competitive inhibition of platelet thromboxane A2 receptor binding by picotamide. Eur J Pharmacol 1989;169:85–93. 11. Watts IS, Wharton KA, White BP et al. Thromboxane (Tx) A2 receptor blockade and TxA2 synthase inhibitor alone and in combination: comparison of antiaggregatory efficacy in human platelets. Br J Pharmacol 1991;121:158–63. 12. Modesti PA, Cecioni I, Colella A et al. Binding kinetics and antiplatelet activities of picotamide, a thromboxane A2 receptor antagonist. Br J Pharmacol 1994;112:81–6. 13. Gresele P, Deckmyn H, Nenci GG et al. Thromboxane receptor antagonists and dual blockers in thrombotic disorders. Trends Pharmacol Sci 1991;121:158–63. 14. Davi G, Catalano I, Averna M. Thromboxane biosynthesis and platelet function in type 2 diabetes mellitus. NEJM 1990;322:1769–74. 15. Balsano F, Violi F and ADEP Group. Effect of picotamide in the clinical progression of peripheral vascular disease. A double blind placebo-controlled study. Circulation 1993;87:1563–9.
G.G. Neri Serneri et al. 16. Milani M, Longoni A, Maderna M. Effects of picotamide, an antiplatelet agent, on cardiovascular events in 438 claudicant patients with diabetes:a retrospective analysis of the ADEP study. Br J Clin Pharmacol 1996;42:782–5. 17. Muggeo M, Verlato G, Bonora E et al. The Verona diabetes study: a population-based survey on known diabetes mellitus prevalence and 5-year all-cause mortality. Diabetologia 1995;38:318–25. 18. Gray JR. A class of K-sample test for comparing the cumulative incidence of a competing risk. Ann Stat 1998;16:1141–54. 19. Marubini E, Valsecchi MG. Analysing survival data from clinical trials and observational studies. New York: Wiley; 1995. 20. Cimminiello C, Milani M. Diabetes mellitus and peripheral vascular disease: is aspirin effective in preventing vascular event. Diabetologia 1996;39:1402–4. 21. Sacco M, Pellegrini F, Roncaglioni MC et al on behalf of the PPP Collaborative Group. Primary prevention of cardiovascular events with low-dose aspirin and Vitamin E in type 2 diabetic patients. Results of the Primary Prevention Project (PPP) trial. Diabetes Care 2003;26:3264–72. 22. EDTRS Investigators. Aspirin effects on mortality and morbidity in patients with diabetes mellitus. Early treatment diabetic retinopathy study report. JAMA 1992;268:1292–1300. 23. Coffman JD. Intermittent claudication. Not so benign. Am Heart J 1986;112:131–3. 24. Makin A, Silverman SH, Lip GYH. Peripheral vascular disease and Virchow’s triad for thrombogenesis. Q J Med 2002;95:199–210. 25. Coccheri S, Palareti G. The cardiovascular risk burden of intermittent claudication. Eur Heart J Suppl 2002;4(Suppl. B):B46–9. 26. Dormandy J, Murray G. The fate of the claudicant. A prospective study of 1968 claudicants. Eur J Vasc Surg 1991;5:131–3. 27. Colwell JA, Bingham SF, Abraira C et al. Veterans Administration cooperative study group on antiplatelet agents in diabetic patients after amputation for gangrene. Effect of aspirin and dipyridamole on atherosclerotic vascular disease rates. Diabetes Care 1986;9:140–8. 28. Cleland JGF. Preventing atherosclerotic events with aspirin (editorial). Br Med J 2002;324:103–5. 29. Yudkin JS. Which diabetic patients should be taking aspirin? Br. Med. J. 1995;311:641–2. 30. Ceriello A, Motz E. Prevention of vascular events in diabetes mellitus. Diabetologia 1996;39:1405–6. 31. Morrow JD, Harris TM, Roberts LJ. Non cycloxygenase formation of a series of novel prostaglandins: analytical ramifications for measurement of eicosanoids. Proc Natl Acad Sci USA 1990;87:9383–7. 32. Mullarkey CJ, Edelstein D, Brownlee M. Free radical generation by early glycation products: a mechanism for accelerated atherogenesis in diabetes. Biochem Biophys Res Commun 1990;173:932–9. 33. Watala C, Golanski J, Pluta J, Boncler M et al. Reduced sensitivity of platelets from type 2 diabetic patients to acetylsalicilic acid (aspirin): its relation to metabolic control. Thromb Res 2004;113:101–13. 34. Di Minno G, Violi F. Aspirin resistance and diabetic angiopathy: back to the future – editorial. Thromb Res 2004;113:97–9. 35. Insel PA. Analgesic-antipyretic and antinflammatory agents. In: Godman A, Gilman A, Rall TW, Niec AS, editors. The pharmacological basis of therapeutics. 9th ed. New York: Pergamon Press; 1996. p. 1712. 36. Berrettini M, De Cunto M, Parise P et al. In vitro and ex vivo effects of picotamide, a combined thromboxane A2-synthase inhibitor and receptor antagonist, on human platelets. Eur J Clin Pharmacol 1990;39:495–500. 37. Modesti PA, Colella A, Cecioni I et al. Capacity of picotamide to diffuse into the arterial wall and bind to receptor of vascular muscle cells. Thromb Haemost 1995;73:1323. 38. Neri Serneri GG, Abbate R, Gensini GF et al. TxA2 production by human arteries and veins. Prostaglandins 1983;25:753–65.