European Heart Journal (2000) 21, 2026–2032 doi:10.1053/euhj.2000.2475, available online at http://www.idealibrary.com on
A randomized placebo-controlled trial to assess the efficacy of antiinflammatory therapy with methylprednisolone in unstable angina (MUNA trial) R. R. Azar1, S. Rinfret2, P. The´roux2, P. H. Stone3, R. Dakshinamurthy4, Y.-J. Feng4, A. H. B. Wu4, G. Range´2 and D. D. Waters 1
Division of Cardiology, San Francisco General Hospital and the University of California, San Francisco, CA, U.S.A.; 2The Montreal Heart Institute, Montreal, Canada; 3The Brigham and Women’s Hospital, Boston, MA, U.S.A.; 4Hartford Hospital, Hartford, CT, U.S.A.
Aims The purpose of this study was to assess the efficacy of antiinflammatory therapy with methylprednisolone during the acute phase of unstable angina. Methods This is a randomized ‘prospective’ double-blind, placebo-controlled trial. Patients with the diagnosis of unstable angina were randomized to a 48-h course of methylprednisolone (n=81) or placebo (n=85). Patient care and therapy were otherwise decided by their attending cardiologist. The primary end-point was a composite of in-hospital recurrence of angina, silent ischaemia on Holter recording, emergency coronary revascularization, readmission with unstable angina, and myocardial infarction or death during the 30-day follow-up. Results The two groups were well balanced and had similar clinical characteristics at baseline. Forty-eight hours after randomization, mean C-reactive protein levels decreased by 2·6 mg . l �1 in the methylprednisolone group, but increased by 1·6 mg . l �1 in the placebo group
Introduction Inflammation has been implicated in the pathogenesis of coronary disease and acute coronary syndromes[1–4]. Histological studies support the concept that atherosclerosis is a chronic inflammatory process leading to progressive narrowing and obstruction of the arterial Revision submitted 22 September 2000, and accepted 4 October 2000. Presented in part at the 72nd Scientific Sessions of the American Heart Association, Atlanta, GA, November, 1999. Correspondence: Rabih R. Azar, MD, MSc, FACC, Division of Cardiology, Hotel Dicu de France Hospital, Achrafreh, Beirut, Lebanon. 0195-668X/00/212026+07 $35.00/0
(P=0·03). The primary end-point occurred in 44% of the methylprednisolone patients and in 33% of the placebo patients (P=0·12). Coronary revascularization rates were equal between the two groups (38% and 40%). When adjustment was made for the difference in revascularization times, a trend towards better event-free survival was seen in the control group (67% vs 57%; P=0·09). Conclusion A 48 h course of antiinflammatory therapy with methylprednisolone given at the doses of this study did not improve the short-term outcome of patients with unstable angina. (Eur Heart J 2000; 21: 2026–2032, doi:10.1053/ euhj.2000.2475) � 2000 The European Society of Cardiology Key Words: Acute coronary syndromes, inflammation, corticosteroids. See page 1990 for the Editorial comment on this article
lumen[1]. Unstable angina is a shift from this chronic indolent course to the acute catastrophic consequences of plaque rupture or erosion. Unstable angina is characterized by activated circulating white cells, high levels of inflammatory cytokines and acute phase reactant proteins[3,5–10]. A growing body of evidence has implicated inflammation in plaque instability, endothelial dysfunction and increased thrombogenesis[11–16]. Unstable angina patients with high levels of inflammatory markers are at high risk for adverse cardiac events and death during hospitalization and following discharge[8–10]. These complications occur despite aggressive antiplatelet and antithrombotic therapies. These considerations raise the possibility that antiinflammatory therapy might reduce the event rate in unstable angina. As this therapeutic approach has not � 2000 The European Society of Cardiology
Methylprednisolone in unstable angina
2027
All patients who were admitted to the two participating institutions with unstable angina, or who developed unstable angina while hospitalized were considered for the study. The most recent episode of chest pain had to have occurred less than 24 h prior to randomization and administration of the first dose of the study drug. The diagnosis of unstable angina was based on a clinical history of chest pain suggestive of myocardial ischaemia, occurring at rest, and lasting for more than 5 min, with normal serum levels of creatine kinase-MB on admission. Ischaemic electrocardiographic changes were defined as deeply inverted or newly peaked positive T waves, or horizontal or downsloping ST segment depression d1 mm, or horizontal or upsloping transient ST segment elevation d1 mm. In the absence of electrocardiographic changes compatible with ischaemia, inclusion in the study required independent confirmation of the diagnosis by two cardiologists. Patients with any of the following conditions were excluded: persistent ST segment elevation consistent with acute myocardial infarction, left bundle branch block, myocardial infarction within 2 weeks, percutaneous revascularization within the preceding 6 months, bypass surgery within 3 months, any coexistent inflammatory or infectious condition, corticosteroid use within the previous month, digoxin therapy (because of interference with ST segment Holter monitoring) and any contraindication to steroid use (e.g. history of active peptic ulcer disease, uncontrolled diabetes mellitus). Patients older than 85 years and women of childbearing potential were also excluded.
trial medication was prepared by the pharmacy on a randomized double-blinded basis. Patients were divided into two equal groups. The active treatment group received methylprednisolone as a bolus followed by seven additional doses every 6 h. The dosage, given intravenously, was 125 mg for the bolus and 40 mg for the maintenance dose for patients with a weight d60 kg. Patients weighing 5 mg . l �1 were considered elevated. To assess the antiinflammatory effects of methylprednisolone, Creactive protein was also measured at 48 h following the study drug bolus in a subgroup of 39 randomly selected patients. All C-reactive protein results were blinded. Holter monitoring for the detection of silent ischaemia was performed for a maximal duration of 24 h, starting 8 h after the study bolus. Holter recordings were sent to the Holter Core Laboratory at the Brigham and Women’s Hospital where they were read by an independent cardiologist blinded to treatment assignment. Patient care decisions were made by the attending cardiologist, who was not involved in the study. In particular, no specific recommendations were made with regard to angiography or revascularization, which could be performed at any time.
Study design
Study end-points
Screening for the study was carried out in the emergency department or as soon as possible after admission. The
The primary end-point of the study was a composite of any of the following during the 30-day follow-up: death
yet been investigated, a study was designed to test the hypothesis that a short course of potent antiinflammatory treatment during the early acute phase of unstable angina, combined with the usual antithrombotic and antiischaemic regimen, would improve short-term outcome.
Methods This prospective, randomized, double-blind, placebocontrolled trial was designed to investigate the efficacy of 48 h treatment with intravenous methylprednisolone on the 30-day outcome of patients admitted with the diagnosis of unstable angina. Patients were recruited from Hartford Hospital in Hartford, Connecticut, and from the Montreal Heart Institute in Montreal, Canada. The study was approved by the institutional review boards of both hospitals. Informed consent was obtained from all patients prior to enrolment. Enrolment began in May 1996 and ended in April 1999.
Patient selection
Eur Heart J, Vol. 21, issue 24, December 2000
2028
R. R. Azar et al.
from any cause, acute myocardial infarction, emergency revascularization driven by ischaemia, silent ischaemia on the Holter recording, chest pain recurrence during hospitalization, or readmission with unstable angina. The secondary end-points were each of the components of the primary end-point taken separately, as well as the number of episodes of recurrent chest pain. Because methylprednisolone requires 6–8 h to exert its full antiinflammatory effects, only events occurring 8 h after the study bolus were considered as end-points. Data were collected on case-report forms by study coordinators at the clinical sites. Follow-up after hospital discharge was obtained by telephone or by a visit to the research clinic. Whenever an event was reported, it was confirmed by a review of hospital records. All patients completed the 30-day follow-up. All events were reviewed and confirmed by an independent investigator (D.D.W.) blinded to treatment allocation. Myocardial infarction was defined as typical chest pain associated with new Q waves on the 12-lead electrocardiogram, or with an at least twofold elevation above normal of the creatine kinase MB subfraction associated with abnormal total creatine kinase. Emergency revascularization was defined as recurrence of chest pain refractory to medical therapy requiring immediate coronary angiography and revascularization. Angina recurrence was defined as recurrence of chest pain similar to that on admission. If electrocardiographic changes suggestive of ischaemia were present, the chest pain was automatically retained as an end-point; however, in the absence of electrocardiographic changes, two cardiologists had to agree that the pain was due to myocardial ischaemia. Ischaemic ST changes on Holter recording analysis were defined as the development of reversible horizontal or downsloping ST segment depression d1 mm below the isoelectric line and d1 mm below the baseline ST segment, or as ST segment elevation d1 mm above the isoelectric line and d1 mm above the baseline ST segment. An episode of ischaemia had to last more than 1 min in order to be regarded as an end-point and at least 1 min had to elapse between episodes for them to be counted as separate events.
Safety considerations Because corticosteroid therapy has been reported to cause complications when used in acute myocardial infarction[17], the study protocol required that the study drug (whether methyprednisolone or placebo) be stopped immediately whenever there was any enzymatic evidence of myocardial infarction. During the trial, a total of 21 acute myocardial infarctions were reported, 15 of which occurred during the first 48 h when the patient was still on the study drug. The drug was discontinued before completion of the full eight doses of treatment in 13 of these 15 patients and continued until the last dose (in violation of the protocol) in the remaining two. The 13 patients who did Eur Heart J, Vol. 21, issue 24, December 2000
not complete the treatment because of early acute myocardial infarction received a mean of 2·1�1·7 doses per patient.
Sample size and statistical analysis The event rate for the primary end-point in the placebo group was predicted to be 40%, based on recent studies of unstable angina that included Holter-based ischaemic events and had comparable follow-up periods[18,19]. A sample size of 82 patients per group was required to detect a 50% reduction in the primary end-point in the active treatment group, using a two-tailed chi-square test with a significance level of 5% and a power of 80%. Continuous variables were expressed as the mean value �1 SD and were compared with a Student t-test. Categorical variables were presented as absolute values and percent, and were compared with a chi-square test. There was no interim data analysis. Statistical analyses of end-points were performed at the end of the trial based on the intention-to-treat principle. The 30-day outcomes in the two groups were compared using the chi-square test. To adjust for the finding that coronary revascularization was performed much earlier in the methylprednisolone group, the primary end-point was also analysed using Kaplan–Meier survival curves. Event-free survival for each group was plotted to the time of coronary revascularization or to completion of the 30-day follow-up (in cases where revascularization was not performed) and was compared using the logrank method. All statistical tests were two-tailed, and a P value 90% of patients in both groups received aspirin and heparin.
Methylprednisolone in unstable angina
Table 1
2029
Baseline clinical characteristics
Age Male gender Hypercholesterolaemia Hypertension Diabetes mellitus Current smoker Family history of CAD Previous UA Previous MI Previous PTCA Previous CABG Admission ECG Normal Ischaemic T waves ST depression ST elevation C-reactive protein on admission (mg . l �1) Elevated C-reactive protein* Elevated troponin† Abnormal stress test No. vessels with CAD‡ 0 1 2 3
Mpred (n=81)
Placebo (n=85)
62�12 48 (59%) 54 (67%) 49 (61%) 17 (21%) 30 (37%) 33 (41%) 41 (51%) 23 (28%) 12 (15%) 16 (20%)
62�12 58 (68%) 49 (58%) 50 (59%) 21 (25%) 24 (29%) 33 (39%) 47 (55%) 31 (37%) 24 (28%) 17 (20%)
37 (46%) 17 (21%) 23 (29%) 3 (4%) 7·9�10·7 30/73 (41%) 20/71 (28%) 19/37 (51%)
41 (48%) 22 (26%) 18 (21%) 4 (5%) 8·3�8·3 33/77 (43%) 23/72 (32%) 22/39 (56%)
6 (12%) 14 (28%) 10 (20%) 20 (40%)
4 (7%) 10 (19%) 16 (30%) 24 (44%)
P value ns ns ns ns ns ns ns ns ns 0·036 ns ns
ns ns ns ns ns
*Defined as >5 mg . l �1; †defined as >0·05 ng . ml �1; ‡defined as d50% diameter stenosis. CABG=coronary artery bypass surgery; CAD=coronary artery disease; ECG=electrocardiogram; MI=myocardial infarction; PTCA=percutaneous transluminal coronary angioplasty. Patients were excluded per protocol if myocardial infarction occurred within 2 weeks, CABG within 3 months, or PTCA within 6 months of enrolment.
Table 2
Table 3 Mean C-reactive protein levels (mg . l �1) prior to randomization and 48 h later
In-hospital treatment
Aspirin Heparin Beta-blockers Intravenous nitroglycerin Calcium channel blockers ACE inhibitors PTCA CABG
Mpred (n=81)
Placebo (n=85)
P value
79 (97%) 75 (93%) 63 (78%) 39 (48%) 23 (28%) 15 (18%) 20 (25%) 11 (14%)
82 (96%) 80 (94%) 71 (83%) 32 (38%) 28 (33%) 18 (21%) 20 (24%) 14 (16%)
ns ns ns ns ns ns ns ns
ACE=angiotensin converting enzyme; CABG=coronary artery bypass graft surgery; PTCA=percutaneous transluminal coronary angioplasty.
Coronary angiography was performed in 104 patients (63%) and revealed at least one vessel disease (stenosis >50%) in 90% of cases.
C-reactive protein levels Immediately prior to randomization, C-reactive protein levels were similar between the steroid and the placebo group (7·9�10·7 vs 8·3�8·3; P=ns). In the 39 patients
CRP (admission) CRP (48 h) Change in CRP
Mpred (n=18)
Placebo (n=21)
P value
5·7�10·1 3·2�9·4* �2·6�2·7
6·8�11·2 9·4�11·1† 1·6�7·3
ns ns 0·03
*P=0·001 compared to C-reactive protein on admission; †P=ns compared to C-reactive protein on admission.
who had C-reactive protein measured at the time of randomization and 48 h later, mean C-reactive protein levels decreased by 2·6�2·7 mg . l �1 in the methylprednisolone group but increased by 1·6�7·3 mg . l �1 in the placebo group (P=0·03; Table 3).
30-day outcome During the first 8 h after the study drug bolus (time when events were not retained as end-points according to the study protocol), 30 patients (37%) in the methylprednisolone group and 23 patients (27%) in the placebo Eur Heart J, Vol. 21, issue 24, December 2000
2030
R. R. Azar et al.
Table 4
Thirty day outcome
Chest pain recurrence Ischaemia on Holter recording Emergency revascularization Readmission with UA MI Death MI or death Any event Time to revascularization (days)
Mpred (n=81)
Placebo (n=85)
P value
27 (33%) 9/70 (13%) 2 (2%) 4 (5%) 6 (7%) 2 (2%) 6 (7%) 36 (44%) 3·4�2·2
23 (27%) 7/74 (9%) 2 (2%) 4 (5%) 5 (6%) 2 (2%) 5 (6%) 28 (33%) 6·1�3·8
ns ns ns ns ns ns ns 0·12 0·002
UA=unstable angina; MI=myocardial infarction.
group had chest pain recurrence (P=ns) and one patient (in the methylprednisolone group) sustained a new myocardial infarction. All end-points were measured 8 h after the first dose of the study medication and were not statistically different between the two groups (Table 4). Slightly more patients in the methylprednisolone group had pain recurrence >8 h after the study drug bolus (33% vs 27%; P=ns), but the median number of chest pain recurrences in either group was two episodes. Holter recordings of adequate technical quality were obtained on 144 patients. Ischaemic ST segment changes were detected in nine patients (13%) in the methylprednisolone group (23 episodes, mean ischaemic time 81�180 min) and seven patients (9%) in the placebo group (13 episodes, mean ischaemic time 15�9·3 min; P=ns for all comparisons). The incidence of coronary revascularization in the two groups was equal, 38% vs 40% (Table 2). However, revascularization was performed much earlier in the methylprednisolone group than in the placebo group, at a mean of 3·4�2·2 compared to 6·1�3·8 days following the study drug bolus; (P=0·002). The incidence of emergency revascularization, a component of the primary end-point, was 2% in each group. Overall, 21 patients sustained an acute myocardial infarction. Of these infarctions, 11 occurred 8 h after the study drug bolus (six in the methylprednisolone and five in the placebo group) of which two in each group were of the Q-wave type. These 11 acute myocardial infarctions were retained as end-points. They occurred before coronary revascularization in seven cases and were a complication of the revascularization procedure in four patients (two patients in each group). Nine of these acute myocardial infarctions occurred during the initial hospitalization and two after hospital discharge. Overall, the interval between study drug Eur Heart J, Vol. 21, issue 24, December 2000
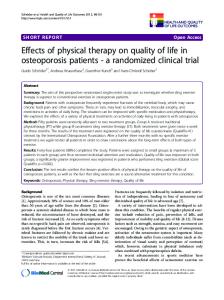
initiation and acute myocardial infarction was similar in the two groups (mean 5·1�8·7 days in the methylprednisolone group vs 6·4�2·9 days in the placebo group; P=ns). However, in the nine patients who had their infarct prior to hospital discharge, the time from randomization to acute myocardial infarction was shorter in the methylprednisolone group (1·6�0·5 vs 6·4�2·9 days; P=0·02). After hospital discharge, four patients in each group were readmitted with unstable angina. The 30-day mortality rate was 2% in the two groups. The causes of death were acute myocardial infarction and cardiogenic shock in three cases (one in the methylprednisolone and two in the placebo group) and septic shock following coronary artery bypass graft surgery in one patient (methylprednisolone group). Overall, methylprednisolone-treated patients had slightly more events than patients in the placebo group, both during hospitalization (42% vs 31%; P=ns) and at 30-day follow-up (primary end-point of the study; 44% vs 33%; P=ns). Kaplan–Meier event-free survival curves (Fig. 1) revealed that the majority of events occurred within the first 48 h after randomization. There was a trend toward better outcome in the placebo group (event-free survival 67% vs 57%; P=0·09).
Discussion This is the first randomized clinical trial assessing the efficacy of antiinflammatory therapy in unstable angina. The hypothesis of the study was that treatment with methylprednisolone would result in a 50% reduction in event rates at 30-day follow-up. The two groups were well matched for baseline clinical characteristics and for in-hospital medical therapy. The study drug was well tolerated and significantly reduced C-reactive protein levels in actively treated patients compared to controls. Contrary to expectation however, all the components of the primary end-point were either equal or slightly worse in the methylprednisolone group. The difference in the primary composite end-point was not statistically significant. Methylprednisolone-treated patients underwent coronary revascularization earlier than control patients
Methylprednisolone in unstable angina
100
90
%
80
70
Placebo
60
Methylprednisolone P = 0·09 by log-rank test
0
10 20 Days following randomization
30
Figure 1 Event-free survival until coronary revascularization or 30 days had elapsed. There is a trend toward better event-free survival in the placebo group, 67% vs 57% (P=0·09). (P=0·001). Their rates of recurrent angina, number of ischaemic episodes and total ischaemia time on Holter monitoring were all slightly higher than the rates in the placebo group, even though the placebo patients were left without revascularization for nearly twice as long, a mean of 6·1 vs 3·4 days. A trend toward better event-free survival was seen in the control group (Fig. 1). Thus, the results of this study support the conclusion that methylprednisolone therapy is of no benefit in unstable angina. It should be emphasized however, that most of the events that comprised the primary end-point were episodes of chest pain or myocardial ischaemia on Holter recording. The incidence of hard end-point events, such as death or acute myocardial infarction, was similar between the two groups but too low to eliminate the possibility of a treatment benefit.
Rational for antiinflammatory therapy in unstable angina Recent studies have provided convincing evidence that unstable angina is an acute inflammatory state. Atherectomy specimens from patients with unstable angina have revealed a more abundant inflammatory cell infiltrate than was seen in specimens from patients with stable angina[12]. Degradative enzymes, such as the metalloproteinases, are actively synthesized and secreted during unstable angina and can undermine the structural integrity of the plaque[20–22]. Patients with unstable angina exhibit activated circulating leukocytes, increased leukocyte function and secretion, and high levels of interleukins and leukotrienes, and acute phase reactant proteins such as C-reactive protein[5–10]. Monocytes from patients with unstable angina have an increased expression of tissue factor[14–16]. This contributes toward shifting the thrombosis–fibrinolysis balance toward thrombosis. Inflammatory cytokines and oxygen free
2031
radicals can cause direct endothelial dysfunction, resulting in an increased propensity for thrombosis and vasospasm. They can also directly depress myocardial function[23]. Unstable angina patients with high levels of inflammatory markers are at higher risk for adverse cardiac events[8–10]. All these findings suggest that antiinflammatory drugs might be useful in unstable angina. Methylprednisolone is a potent antiinflammatory agent with an excellent safety profile, especially during short-term use. In this study, methylprednisolone decreased C-reactive protein levels at 48 h following initiation of treatment, while C-reactive protein levels increased in controls. This is direct evidence that a substantial antiinflammatory effect was achieved with therapy. The major mechanisms for this antiinflammatory action are inhibition of phospholipases and transcription of various cytokines[24,25[. Glucocorticoids also inhibit polymorphonuclear leukocyte accumulation in inflamed tissue[26]. The full antiinflammatory effects of methylprednisolone via these mechanisms are delayed for many hours following administration of the drug.
Possible reasons for the lack of efficacy of methylprednisolone There are several potential explanations for the lack of benefit from methylprednisolone in this study. The duration of therapy might have been too short. Also, treatment may have been initiated too late; the delay from the onset of chest pain to treatment was 8 h, and an additional 8 h probably elapsed before the full antiinflammatory activity of the drug would take effect. By this time, plaque erosion or rupture had already occurred, and significant and possibly irreversible damage may have been caused by activated leukocytes. In addition to its antiinflammatory activity, methylprednisolone is also an immunosupressant[25]. Prior studies have shown that unstable angina is accompanied by activation of humoral and cellular immunities, and that inadequate activation of these systems is associated with higher event rates[27]. The recent reports linking infectious agents to acute coronary syndromes is relevant to these findings. If this link is confirmed, immunosuppressive agents may turn out to be contraindicated in unstable angina, and antibiotics might become a component of routine care[28,29]. Finally, the systemic acute inflammatory response seen in unstable angina may be a consequence of plaque rupture rather than its cause, and may not be incriminated in the pathogenesis of complications, but only be a marker of increased risk.
Study limitations This study is limited by its small sample size. The routine use of aspirin and heparin have reduced the incidence of acute myocardial infarction and death in unstable angina to less than 4%[30]. This trial was not powered to Eur Heart J, Vol. 21, issue 24, December 2000
2032
R. R. Azar et al.
show a significant difference in these hard events. The primary end-point was a composite of clinical events, including chest pain recurrence. Coronary angiography and revascularization were allowed any time during the study course. Early revascularization might have masked the full effect of corticosteroid therapy, either beneficial or detrimental. However, early intervention and discharge are a common approach in patients with acute coronary syndromes. The results of this trial are thus applicable in the context of how unstable angina is currently managed.
Conclusion A 48-h course of antiinflammatory therapy with methylprednisolone given at the doses of this study does not improve the short-term outcome of patients with unstable angina. This, however, does not prove that suppression of acute inflammation is of no value in acute coronary syndromes. Other more selective antiinflammatory drugs with a more rapid onset of action and without immunosuppressive activity may yield different results and may be a safe and synergistic addition to the current antithrombotic and antiischaemic therapies.
References [1] Ross R. Atherosclerosis — An inflammatory disease. N Engl J Med 1999; 340: 115–26. [2] Mehta JL, Saldeen TGP, Rand K. Interactive role of infection, inflammation and traditional risk factors in atherosclerosis and coronary artery disease. J Am Coll Cardiol 1998; 31: 1217–25. [3] Azar RR, Waters DD. The inflammatory etiology of unstable angina. Am Heart J 1996; 132: 1101–6. [4] Buja LM, Willerson JT. Role of inflammation in coronary plaque disruption. Circulation 1994; 89: 36–44. [5] Mazzone A, DeServi S, Ricevuti G et al. Increased expression of neutrophil and monocyte adhesion molecules in unstable coronary artery disease. Circulation 1993; 88: 358–63. [6] Mehta J, Dinerman J, Mehta P et al. Neutrophil function in ischemic heart disease. Circulation 1989; 79: 549–56. [7] Ghaisas NK, Shahi CN, Foley B et al. Elevated levels of circulating soluble adhesion molecules in peripheral blood of patients with unstable angina. Am J Cardiol 1997; 80: 617–9. [8] Liuzzo G, Biasucci LM, Gallimore JR et al. The prognostic value of C-reactive protein and serum Amyloid A protein in severe unstable angina. N Engl J Med 1994; 331: 417–24. [9] Biasucci LM, Liuzzo G, Grillo RL et al. Elevated levels of C-reactive protein at discharge in patients with unstable angina predict recurrent instability. Circulation 1999; 99: 855–60. [10] Morrow DA, Rifai N, Antman E et al. C-reactive protein is a potent predictor of mortality independently of and in combination with troponin T in acute coronary syndromes: A TIMI 11A substudy. J Am Coll Cardiol 1998; 31: 1460–5. [11] Van der Wal AC, Becker AE, van der Loos CM, Das PK. Site of intimal rupture or erosion of thrombosed coronary athero-
Eur Heart J, Vol. 21, issue 24, December 2000
[12] [13] [14]
[15]
[16] [17] [18] [19]
[20] [21]
[22]
[23] [24] [25] [26] [27]
[28] [29]
[30]
sclerotic plaques is characterized by an inflammatory process irrespective of the dominant plaque morphology. Circulation 1994; 89: 36–44. Moreno PR, Falk E, Palacios IF, Newell JB, Fuster V, Fallon JT. Macrophage infiltration in acute coronary syndromes: implication for plaque rupture. Circulation 1994; 90: 775–8. Kaartinen M, van der Wal AC, van der Loos CM et al. Mast cell infiltration in acute coronary syndromes: implications for plaque rupture. J Am Coll Cardiol 1998; 32: 606–12. Jude B, Agraou B, McFadden EP et al. Evidence for timedependent activation of monocytes in the systemic circulation in unstable angina but not in acute myocardial infarction or in stable angina. Circulation 1994; 90: 1662–8. Moreno PR, Bernardi VH, Lopez-Cuellar J et al. Macrophages, smooth muscle cells, and tissue factor in unstable angina. Implication for cell-mediated thrombogenicity in acute coronary syndromes. Circulation 1996; 94: 3090–7. Seneri GGN, Abbate R, Gori AN et al. Transient intermittent lymphocyte activation is responsible for the instability of angina. Circulation 1992; 86: 790–7. Roberts R, DeMello V, Sobel B. Deleterious effects of methylprednisolone in patients with myocardial infarction. Circulation 1976; 53: I204–I206. Serneri GGN, Modesti PA, Gensini GF et al. Randomized comparison of subcutaneous heparin, intravenous heparin and aspirin in unstable angina. Lancet 1995; 345: 1201–4. Holdright D, Patel D, Cunningham D et al. Comparison of the effect of heparin and aspirin vs aspirin alone on transient myocardial ischemia and in-hospital prognosis in patients with unstable angina. J Am Coll Cardiol 1994; 24: 39–45. Brown DL, Hibbs MS, Kearney M, Loushin C, Isner JM. Identification of 92-kD gelatinase in human coronary atherosclerotic lesions. Circulation 1995; 91: 2125–31. Kai H, Ikeda H, Yasukawa H et al. Peripheral blood levels of matrix metalloproteases-2 and -9 are elevated in patients with acute coronary syndromes. J Am Coll Cardiol 1998; 32: 368–72. Dinerman JL, Mehta JL, Saldeen TGP et al. Increased neutrophil elastase release in unstable angina pectoris and acute myocardial infarction. J Am Coll Cardiol 1990; 15: 1559–63. Fauler J, Frolich JC. Cardiovascular effects of leukotrienes. Cardiovasc Drug Ther 1989; 3: 499–505. Williams TJ, Yarwood H. Effect of glucocorticoids on microvascular permeability. Am Rev Respir Dis 1990; 141: S39– S43. Goldfien A. Adrenocorticosteroids and adrenocortical antagonists. In: Katzung BG, ed. Basic and Clinical Pharmacology. Appleton and Lange, California, U.S.A., 1998: 635–41. Dale DC, Fauci AS, Guerry D, Wolff SM. Comparison of agents producing a neutrophilic leukocytosis in men. J Clin Invest 1975; 56: 808–13. Caligiuri G, Liuzzo G, Biasucci LM, Maseri A. Immune system activation follows inflammation in unstable angina: pathogenetic implications. J Am Coll Cardiol 1998; 32: 1295– 304. Gurfinkel E, Bozovich G, Daroca A, Beck E, Mautner B. Randomised trial of roxithromycin in non-Q-wave coronary syndromes: ROXIS pilot study. Lancet 1997; 350: 404–7. Gupta S, Leatham EW, Carrington D, Mendall MA, Kaski JC, Camm J. Elevated Chlamydia penumoniae antibodies, cardiovascular events, and azithromycin in male survivors of acute myocardial infarction. Circulation 1997; 96: 404–7. The´ roux P, Ouimet H, McCans J et al. Aspirin, heparin or both to treat acute unstable angina. N Engl J Med 1988; 319: 1105–11.